Introduction
POI is a post-surgical complication mediated by stress and
systemic inflammation, often causing temporary impairment of
gastrointestinal dynamics and prolonging recovery time, mainly
manifested by abdominal pain, bloating, nausea and vomiting,
no exhaust and defecation, and diminished bowel sounds, which
were the main causes of high morbidity, prolonged hospital stay,
and high utilization of medical resources [1,2]. Data provided by a
healthcare provider indicate that hospitalization costs for patients
who develop POI after colectomy are twice as high as those who
do not develop intestinal paralysis, that more than half of patients
with intestinal paralysis develop at least one adverse outcome,
and that additional complications that occur lead to increased
mortality [3]. Current mechanistic studies on POI have focused
on the complex interactions related to neurogenic, inflammatory,
humoral, electrolyte, and pharmacological components [2]. The
first phase is neurally mediated and involves intraoperative and
postoperative activation of adrenergic neurons by incisional trauma, which activates pro-adrenocorticotropic releasing factors and
causes acute intestinal paralysis. The second phase, starting 3-4
h postoperatively, is mediated by inflammation, where various
types of inflammatory factors activate macrophages in the intestine, triggering the migration of leukocytes to the outer muscular
layer, and macrophages inhibit smooth muscle contraction by releasing nitric oxide and prostaglandins. Electrolyte disturbance is
one of the risk factors for POI. Low potassium decreases smooth
muscle excitability and diastolic function and reduces gastrointestinal motility; Fluid overload also prolongs postoperative recovery
of gastrointestinal function. In addition, the use of opioid analgesics decreases gastrointestinal nerve activity and delays transit
function [4].
In terms of treatment, we generally use anti-infection, rehydration, analgesia, enteral nutrition, and other nursing treatment
plans for POI. With the emergence of the Enhanced Recovery After Surgery (ERAS) concept, accelerating postoperative gastrointestinal recovery has become a topic of research for many scholars, aiming to shorten hospital stays, improve patients’ quality
of life, and reduce postoperative complications and readmission
rates, for which many studies have proposed innovative therapies. Watanabe, J and Eamudomkarn, N et al. suggested [5,6]
that postoperative coffee consumption shortens the time to first
defecation and accelerates gastrointestinal recovery without side
effects. Its effects are mediated through caffeine and chlorogenic
acid, with caffeine dilating blood vessels to promote gastrointestinal recovery and chlorogenic acid acting as an anti-inflammatory,
edema-inhibiting agent and improving pain. However, coffee consumption raises blood pressure and heart rate, which has limitations for patients with hypertension. Short, V et al [7] conducted
a meta-analysis of chewing gum to promote postoperative bowel
obstruction suggesting that chewing gum shortens the time to
first defecation and bowel movement after surgery but has a large
effect on colorectal surgery and a small effect on cesarean section. However, one perioperative care guideline [8] for colorectal
surgery does not recommend oral coffee drinking or gum chewing for postoperative patients, both of which reduce the duration
of postoperative intestinal paralysis but lack large, high-quality
confirmatory studies, and the exact mechanisms need to be further elucidated. Therefore, there is an urgent need for a safer and
more effective treatment method.
Acupuncture and moxibustion have been experienced in China
for thousands of years, sprung from the Neolithic era, have a complete academic theoretical system, and have become one of the
major medical resources in China and some other Asian countries.
Acupuncture has also been increasingly accepted by practitioners
and patients around the world, bringing more benefits to patients
with various functional gastrointestinal disorders because of its
ease of use, low cost, significant efficacy, and few complications
[9]. In a randomized controlled trial of 129 patients with primary colorectal cancer [10], electroacupuncture at Zusanli (ST 36)
shortened the time to first defecation after surgery and was more
tolerant of a liquid diet than the control group. A meta-analysis
evaluating the efficacy of EA for post-abdominal surgery intestinal
paralysis [11] showed that EA is a safe and effective therapeutic
method, in which Zusanli (ST36), Shangjuxu (ST37), and Xiajuxu
(ST39) are the preferred acupoints for the treatment of POI, but
its efficacy in terms of postoperative analgesia is poor. Research
on the analgesic aspects of acupuncture is somewhat controversial, and further clinical studies are needed to add to the evidence
for evidence-based medicine.
Case presentation
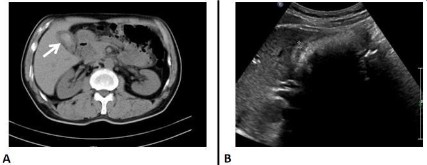
The patient was a 60-year-old man with a history of cholecystolithiasis for 10 years. He came to our hospital with right upper
abdominal pain for 6 days. Physical examination showed a normal
abdominal profile, soft abdominal muscles, and right upper abdominal pressure pain without rebound pain. Murphy’s sign was
positive. The clinic examination of blood routine suggests a high
inflammatory index, abdominal CT suggests: gallbladder stones,
and possible cholecystitis. He was given oral moxifloxacin and
dexamethasone tablets, and his symptoms were relieved, but he
still had paroxysmal abdominal pain. Subsequently, abdominal ultrasound showed thickening of the gallbladder wall and gallbladder-filled gallbladder stones (Figure 1).
The patient’s condition was considered stable and the operative treatment was decided after communicating with his family.
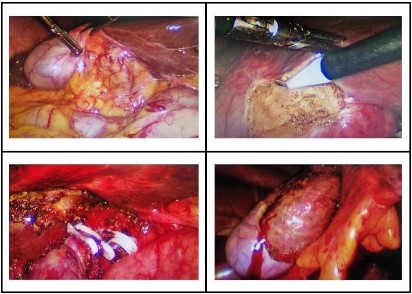
Therefore, laparoscopic cholecystectomy was performed on January 31, 2023. After successful anesthesia, the patients
were taken supine position and made 1, 1, 0.5 and 0.5 cm incisions at the lower edge of the umbilicus, the middle xiphoid process of the upper abdomen, the middle line of the right clavicle,
the right costal margin and the front line of the right armpit respectively. A pneumoperitoneum needle was inserted through
the incision at the lower edge of the umbilicus. The size of the
gallbladder was about 8 x 6 x 3 cm, the serosa of the gallbladder
was hyperemia and edema, and the common bile duct was not
dilated. The triangle of the gallbladder was dissected, the cystic
duct was dissociated, clipped, and clipped, the cystic artery was
dissociated and clipped, the gallbladder was completely separated from the gallbladder bed by electric hook, and the gallbladder
was removed from the body through the incision under the xiphoid process. The operation went well, with good intraoperative
anesthesia, and the patient returned to the ward safely after the
operation (Figure 2).
After the operation, the drainage tube was put in for the treatment of anti-infection, fluid replacement, and nutritional support.
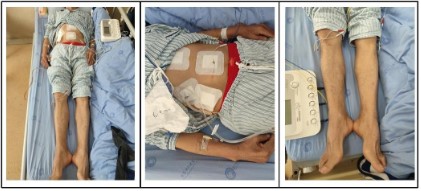
On the second postoperative day, the patient complained of incisional pain but tolerable, abdominal distension, and the anus was deflated but not defecated. The patient was treated with EA,
the pain of the incision was relieved after the treatment and the
patient defecated on the 2nd day.
Treatment: Tianshu (ST25), Zhigou (TE6), Zusanli (ST36), Yanglingquan (LR3), taichong straight acupuncture; ST25, ST36, LR3
plus electroacupuncture for 30 minutes (Figure 3).
After EA treatment, the patients defecated at 67.5 h after the
operation, and the visual Analogue Scale (VAS) of pain was reduced, the time of tolerance to diet was shortened, and the I-FEED score was decreased (Table 1-2).
Discussion
In this case, since electroacupuncture was intervened after
the patient had already deflated, the primary observation was
the time to first postoperative defecation (i.e., counting from
the postoperative period), and the secondary observations were
VAS score, time to tolerate diet (fluid or semifluid), I-FEED score,
and length of hospital stay. We found that patients experienced a sensation of defecation immediately after the first treatment and
that defecation started after the second treatment; Pain scores
decreased after each treatment, but not significantly. POI is due
to transient impairment of gastrointestinal function, while the I-FEED scale is a new index developed by expert consensus for assessing postoperative gastrointestinal recovery, measured by five
main elements, namely intake, nausea, vomiting, physical examination, and duration; the higher the score, the longer the hospital
stay [12]. The scores of I-FEED in this patient gradually decreased
after treatment, suggesting the recovery of gastrointestinal function. In conclusion, EA treatment can promote the recovery of
gastrointestinal function in patients with POI.
Table 1: Recovery of gastrointestinal function.
| Primary outcome |
|
| (1) Time to first defecation(h) |
67.5 |
| Secondary outcome |
|
| (1) Time tolerability of liquid food(h) |
14 |
| (2) Time tolerability of semiliquid food(h) |
70 |
| (3) Length of postoperative hospital stay(d) |
4 |
Table 2: Severity of postoperative symptoms/assessment scale.
|
Day 1 |
Day 2 |
Day 3 |
Day 4 |
| VAS pain score |
4 |
3 |
3 |
2 |
| I-FEED score |
4 |
4 |
3 |
2 |
As described previously, POI is the result of neurological, inflammatory, and pharmacological interactions. Intraoperative
anesthesia, stretching, and other manipulations can impair the
integrity of the organism and cause postoperative gastrointestinal
dysfunction. Although the potential mechanisms of electroacupuncture treatment have not yet been fully elucidated, there has
been considerable research into the anti-inflammatory mechanisms of acupuncture. EA stimulation of the ST36 promotes
contraction of the distal colon via the cholinergic pathway [13];
however, Fang, J F et al. suggested [14] that EA stimulation does
shorten postoperative gastrointestinal transit time and promotes
gastric emptying, but its mechanism of action is mediated mainly
by stimulation of Nucleus Tractus Solitaries (NTS) neurons rather
than by activation of the cholinergic anti-inflammatory pathway,
and no reduction in inflammatory cell infiltration was observed
in the experiment. Subsequently, Yang, N N et al [15] found that
EA could attenuate peripheral inflammatory expression by suppressing the local immune response and correlated with acupoint
selection and stimulation frequency. They also suggested [16]
that EA stimulation of the ST36 could inhibit GABAA receptor expression in the Dorsal Nucleus of the Vagus nerve (DMV) and that
the excited vagus nerve suppressed inflammatory responses triggered by intestinal manipulation and promoted gastrointestinal
motility through activation of the α7nAChR-mediated JAK2/STAT3
signaling pathway. Therefore, the mechanism by which acupuncture promotes POI recovery needs to be further studied.
POI is a common post-surgical complication that affects patients' quality of life and prolongs their hospital stay. The concept
of ERAS runs through the preoperative, intra-operative, and post-operative stages. It refers to the use of evidence-based medical
strategies through multidisciplinary cooperation to optimize peri-operative management measures to reduce surgical stress, pain,
and complications, restore the function of all organs as soon as
possible, and facilitate their postoperative rehabilitation process.
A study on the effect of preoperative walking on POI found that
preoperative walking reduced the time to first defecation and
bowel movement after gynecological surgery and decreased the
incidence of POI, but the exact mechanism was not clear, perhaps
related to faster colonic and rectal transit time for physical activity
[17]. There is a large body of clinical research on post-surgical interventions to reduce the duration of intestinal paralysis and less
research on preoperative prehabilitation. Preoperative prehabilitation can avoid the limitation of postoperative incision to local
treatment, and whether it can prevent POI, or accelerate gastrointestinal rehabilitation, is a direction worthy of further research
efforts in the future, and provide new ideas for clinical treatment.
Conclusion
POI is a common postoperative complication mediated by inflammation, which is characterized by high morbidity, high utilization of medical resources, low quality of life, and prolonged hospital stay, with postoperative inflammatory infection as its main
cause. A recent multicenter randomized clinical trial successfully
confirmed the effectiveness of EA for POI [18], similar to the intervention in this case. EA can accelerate the recovery of gastrointestinal function in POI patients, greatly shorten their hospitalization
time, improve their quality of life, and have no clinical adverse
effects, which is a guiding meaning for clinical treatment. We can
further study the clinical mechanism of EA and add evidence for
evidence-based medicine.
Conflict of interest statement: No conflict of interest.
Funding: This case report received no funding.
References
- Iyer S, Saunders WB, S. Stemkowski. Economic burden of post-operative ileus associated with colectomy in the United States. J
Manag Care Pharm. 2009; 15: 485-94.
- Bragg D, et al. Postoperative ileus: Recent developments in pathophysiology and management. Clin Nutr. 2015; 34: 367-76.
- Tevis SE, et al. Postoperative Ileus-More than Just Prolonged
Length of Stay? J Gastrointest Surg. 2015; 19: 1684-90.
- Kurz A, DI Sessler. Opioid-induced bowel dysfunction: Pathophysiology and potential new therapies. Drugs. 2003; 63: 649-71.
- Watanabe J, et al. Effect of Postoperative Coffee Consumption on
Postoperative Ileus after Abdominal Surgery: An Updated Systematic Review and Meta-Analysis. Nutrients, 2021; 13.
- Eamudomkarn, N, et al. Effect of postoperative coffee consumption on gastrointestinal function after abdominal surgery: A systematic review and meta-analysis of randomized controlled trials.
Sci Rep. 2018; 8: 17349.
- Short V, et al. Chewing gum for postoperative recovery of gastrointestinal function. Cochrane Database Syst Rev. 2015: CD006506.
- Oodit R, et al. Guidelines for Perioperative Care in Elective Abdominal and Pelvic Surgery at Primary and Secondary Hospitals in
Low-Middle-Income Countries (LMIC’s): Enhanced Recovery After
Surgery (ERAS) Society Recommendation. World J Surg. 2022; 46:
1826-1843.
- Ouyang H, JD Chen. Review article: Therapeutic roles of acupuncture in functional gastrointestinal disorders. Aliment Pharmacol
Ther. 2004; 20: 831-41.
- Yang JW, et al. Effect of acupuncture on postoperative ileus after laparoscopic elective colorectal surgery: A prospective, randomised, controlled trial. E Clinical Medicine. 2022; 49: 101472.
- Chen KB, et al. Electro acupuncture or transcutaneous electro acupuncture for postoperative ileus after abdominal surgery: A systematic review and meta-analysis. Int J Surg. 2019; 70: 93-101.
- Alsharqawi N, et al. Validity of the I-FEED score for postoperative
gastrointestinal function in patients undergoing colorectal surgery.
Surg Endosc. 2020; 34: 2219-2226.
- Luo, D, et al. Electro acupuncture at acupoint ST-36 promotes contractility of distal colon via a cholinergic pathway in conscious rats.
Dig Dis Sci. 2008; 53: 689-93.
- Fang JF, et al. Electro acupuncture treatment partly promotes the
recovery time of postoperative ileus by activating the vagus nerve
but not regulating local inflammation. Sci Rep. 2017; 7: 39801.
- Yang NN, et al. Effects of electro acupuncture on the intestinal motility and local inflammation are modulated by acupoint selection
and stimulation frequency in postoperative ileus mice. Neurogastroenterol Motil. 2020; 32: e13808.
- Yang, N.N, et al. Electro acupuncture ameliorates intestinal inflammation by activating α 7nAChR-mediated JAK2/STAT3 signaling pathway in postoperative ileus. Theranostics. 2021; 11: 4078-4089.
- Özdemir İA, et al. Impact of pre-operative walking on post-operative bowel function in patients with gynecologic cancer. Int J Gynecol Cancer. 2019; 29: 1311-1316.
- Wang Y, et al. Electro acupuncture vs Sham Electro acupuncture in
the Treatment of Postoperative Ileus After Laparoscopic Surgery
for Colorectal Cancer: A Multicenter, Randomized Clinical Trial.
JAMA Surg. 2023; 158: 20-27.