Introduction
Ankyloglossia or tongue-tie is a singularly congenital case
qualified by a specific no elastic and dense frenum within lingual
muscle. Also it’s occurs when there is an union of the tongue’s
body to the mouth’s floor, reducing her motion [1]. Its prevalence
ranged of 0.02% to 12%. Lack of unified consensus may explain
these rates changing on prevalence of ankyloglossia [2]. A higher
incidence revealed in studies exploring neonates in comparison to those realized in other population was revealed by Reddy et
al. 2014 [3]. The authors suggested the resolution of beginner
variants of ankyloglossia during development justifying the age
related difference of prevalence [4].
Ankyloglossia limits physiological tongue movement and may
induce numerous functional, behavioral and speech difficulties
[5,6]. In order to rectify these situations the treatment of
ankyloglossia would requires frenal excision ensuring lingual motion [2]. The aim of this paper review illustrated with 2 clinical
cases is to allow clarification of the basis, consequences and
surgical management of severe tongue-tie.
Case presentation
Case I
A 14-years boy complains of lingual adhesion associated to
speech trouble. In examination, the subject suffer from tongue-tie
and his lingual mobility was limited (protrusion with a feeling of
pulling, atypical swallowing, and inability of the tongue to reach
retro palatal incisor region). The sign of severe ankyloglossia is
clinically revealed by a deformity of the tongue and is classified
as Class III using Kotlow’s assessment (Figure 1). The challenge
was dental crowding, malocclusion due to maxillary cleft and an
atypical swallowing. No genetic implication was observed in the
parents.
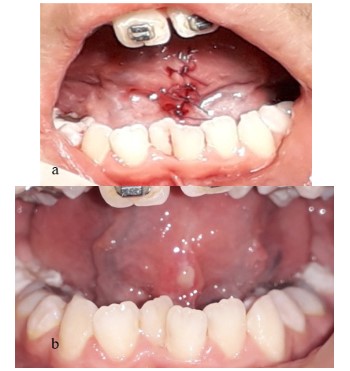
The management of this case is illustrated in Figure 2.
Under local anesthesia, first an hemostat was clamped into the
basis of the lingual frenum and followed by an incision at the upper side of the instrument. To close wound edges, superficial layer
muscle fibres were dissected. Sutures were made to promote primary healing to reduce scar formation.
The post-operative period was asymptomatic without bleeding
or pain (analgesic level 1 for 3 days). Sutures were removed after
7 days, lingual mobility was improved (Figure 3). Lingual rehabilitation and follow-up with the speech therapist was recommended
for this patient.
Case II
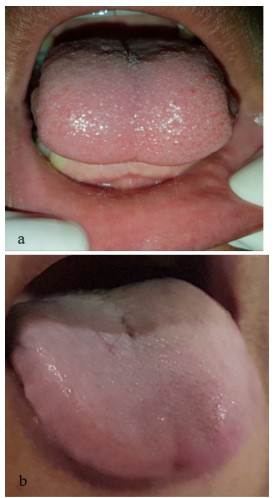
A 45-years male in apparently good general health, presented
a short lingual frenum. The diagnosis show reduced lingual movements, and ankyloglossia Class III in Kotlow’s classification (Figure
4). No genetic implication was declared by the patient and no intervention before was in taking.
Under local anesthesia, first an hemostat was clamped into
the basis of the lingual frenum and followed by an incision at the
upper side of the instrument. To reach easily closure superficial
layer muscle fibres was dissected. Sutures were made to promote
primary healing to reduce scar formation on the tongue's tip and
buccal floor.
Just after the intervention, the patient was able to move more
easily his tongue (Figure 5).
At the follow-up a better protrusion of the tongue and normal
posture were possible without difficulty (Figure 6).
Discussion
At the beginning, a U-shaped split is formed on either sides of
the tongue [7]. Before 8 years old, the body of the tongue gradually becomes free from the sides and the floor of the mouth [8,3].
A median fold of mucosal tissue is persistent near from the tip [3].
This procures lingual mobility, except at the region of attachment
of lingual frenum [7]. Failure in apoptosis process of embryonic
cells express fibrous and brief lingual frenulum linking tongue to
its buccal floor [9].
Many morphological, anatomical and functional classifications
have been cited in the literature [9]. The most used and simple is
the Kotlow’s classification [9]. According to its observations, we
can define four types of ankyloglossia in relation to free tongue
movement [3]. To achieve the diagnosis, a clinical-functional assessment has been suggested by Olivi et al. in 2012 [10].
In a review, Pompéia et al. in 2017 [11] concluded that clinicians approved negative effects of lingual frenum’s anatomic and
functional changes over craniofacial evolution and development.
As described, numerous studies revealed link of those clinical outcomes and tongue mobility.
• Restriction of lingual frenulum and orthognathic development:
- The ankyloglossia can result in a reduction of maxillary development [12],
- A link in limited lingual movement with an elongation of the
soft palate was demonstrated [13],
- The development of skeletal Class III malocclusion [8], and
the predilection of mandibular prognathism were related to
tongue-tie [3],
• Restriction of lingual frenulum and functions of the
tongue:
- The tongue tie is reveled as an obstructive sleep apnea a
phenotype in children [14], it also maintain the atypical swallow [3], and may alter oral speech [15],
• Restriction of lingual frenulum and Oral hygiene:
- A short lingual frenulum may regularly limit the capacity of
cleaning teeth. It seems to increase the prevalence of tooth
decay [2],
• Restriction of lingual frenulum and Periodontal health:
- Tongue tie can alter the gum and contribute to periodontal
problems with apparition of gingival recession as described by
Nathan in 2017 [16]. According to Veyssiere et al. in 2015 [9], this
condition can be painful, may lead to poor oral hygiene, which
in turn accelerate periodontal disease. In recent paper report of
Bahadure et al. in 2019 [17], a rare and unique pattern of ankyloglossia where lingual frenulum was exceptionally attached and
merged with lower labial frenum was described.
Managing tongue-tie is related to age, the location of the
frenulum, the restriction degree, functional conditions, or social
troubles [1,18]. In summary, current best practice should include
frenectomy as a complete excision of the frenum with release of lingual muscle fibers [6]. The aim is to separate the lingual body
from its frontal join close to mucosal jaw [9]. This intervention
gives maximum motion of the tongue’s tip [16].The treatment
of ankyloglossia can be realized via scalpel, electrocautery using
multiple electrodes, or with laser surgery providing simultaneous
cutting and cautery of soft tissue [16]. Even if laser offers advantages on surgery, some surgeons choose scalpel technique procuring more precise dissection. The variation on size of connective
and fibrous compounds would determine the best technique of
frenectomy [16].
According to literature, minor nerve or vascular vessels were
objectified in middle of lingual frenum. In general, It’s considered
as a safe inferior plane as concluded by Hou et al. in 2012 [19]. The
lingual topography and anatomy are at risk of multiple intraoperative or postoperative issues [6]. Among these complications, we
can cite: hemorrhage, hematoma, paresthesia, infection. Also the
re-establishment of frenal bond and scars may exerce a restriction
in tongue movement [6]. Additionally, the lingual surgery on ventral area would induce Blandin-Nuhn gland mucocele, or blockage
of Wharton’s duct as described by Hungund et al. in 2013 [20] and
Barot et al. in 2014 [18].
Conclusion
Ankyloglossia can apply deleterious effect on daily life. Those
worse outcomes can be explained by neglecting this congenital
anomaly. It is suggested that early diagnosis and treatment of abnormal frenum are essential to optimal oral development. Different groups have to intervene for better tongue tie management.
Declarations
Conflicts of interest statements: There is no conflict of interests affecting any author.
Funding sources: This research has not received any specific source funding.
References
- Garrocho-Rangel A, Herrera-Badillo D, Pérez-Alfaro I, Fierro-Serna
V, Pozos-Guillén A. Treatment of ankyloglossia with dental laser in
paediatric patients: Scoping review and a case report. Eur J Paediatr Dent. 2019; 2: 155–63.
- Walsh J, McKenna Benoit M. Ankyloglossia and Other Oral Ties.
Otolaryngol Clin North Am. 2019; 52: 795-811.
- Reddy N, Marudhappan Y, Devi R, Narang S. Clipping the (tongue)
tie. J Indian Soc Periodontol. 2014; 18: 395-398.
- Chaubal T, Dixit M. Ankyloglossia and its management. J Indian Soc
Periodontol. 2011; 15: 270-272.
- Komori S, Matsumoto K, Matsuo K, Suzuki H, Komori T. Clinical
Study of Laser Treatment for Frenectomy of Pediatric Patients. Int
J Clin Pediatr Dent. 2017; 10: 272-277.
- Varadan M, Chopra A, Sanghavi AD, Sivaraman K, Gupta K. Etiology
and clinical recommendations to manage the complications following lingual frenectomy: A critical review. J Stomatol Oral Maxillofac Surg. 2019; 120: 549-553.
- Meenakshi S, Jagannathan N. Assessment of Lingual Frenulum
Lengths in Skeletal Malocclusion. J Clin Diagn Res. 2014; 8: 202-204.
- Jang S-J, Cha B-K, Ngan P, Choi D-S, Lee S-K, et al. Relationship between the lingual frenulum and craniofacial morphology in adults.
Am J Orthod Dentofacial Orthop. 2011; 139: e361-7
- Veyssiere A, Kun-Darbois JD, Paulus C, Chatellier A, Caillot A, et
al. Diagnostic et prise en charge de l’ankyloglossie chez le jeune
enfant. Rev Stomatol Chir Maxillo-Faciale Chir Orale. 2015; 116:
215-220.
- Olivi G, Signore A, Olivi M, Genovese MD. Lingual frenectomy:
functional evaluation and new therapeutical approach. Eur J Paediatr Dent. 2012; 13: 101-106.
- Pompéia LE, Ilinsky RS, Ortolani CLF, Faltin Júnior K. ankyloglossia and its influence on growth and development of the stomatognathic system. Rev Paul Pediatr. 2017; 35: 216-221.
- Srinivasan B, Chitharanjan AB. Skeletal and dental characteristics
in subjects with ankyloglossia. Prog Orthod. 2013; 14: 44.
- Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, et al. Ankyloglossia
as a risk factor for maxillary hypoplasia and soft palate elongation:
A functional - morphological study. Orthod Craniof ac Res. 2017;
20: 237-244.
- Zaghi S, Valcu-Pinkerton S, Jabara M, Norouz-Knutsen L, Govardhan C, , et al. Lingual frenuloplasty with myofunctional therapy:
Exploring safety and efficacy in 348 cases. Laryngoscope Investig
Otolaryngol. 2019; 4: 489-496.
- Marchesan IQ, Martinelli RL, Gusmão RJ. Lingual frenulum: changes after frenectomy. J Soc Bras Fonoaudiol. 2012; 24: 409-412.
- Nathan JE. The Indications, Timing, and Surgical Techniques for
Performing Elective lingual and Labial Frenulectomies for Infants
and Children. Inter J Otorhinolaryngol. 2017; 4: 3.
- Bahadure R, Jain E, Singh P, Pandey R, Chuk R. Labial ankyloglossia:
A rare case report. Contemp Clin Dent. 2016; 7: 555.
- Barot VJ, Vishnoi SL, Chandran S, Bakutra GV. Laser: The torch of
freedom for ankyloglossia. Indian J Plast Surg. 2014; 47: 418-422.
- Hou T, Shao J, Fang S. The definition of the V zone for the safety
space of functional surgery of the tongue. The Laryngoscope. 2012
Jan;122(1):66–70.
- Hungund S, Dodani K, Kambalyal P, Kambalyal P. Comparative Results Of Frenectomy By Three Surgical Techniques- Conventional,
Unilateral Displaced Pedicle Flap And Bilateral Displaced Pedicle
Flap. Dentistry. 2013; 04: 183.