Introduction
Ameloblastoma represents 1% of all oral tumors and 11% of
odontogenic tumors. They are located much more frequently on
mandibular bone, rather than maxillary bone, more often in the
posterior region instead of the anterior one, except for the African black race which is localized more frequently at the symphysis. It’s extremely rare to find these tumors in extra-mandibular
locations, because of the association between their etiology and
dental structures. However, extra bony localizations at the alveolar mucosa known as peripheral or extraosseous ameloblastomas are described. Based on the aspects found in pathological
anatomy, it is possible to recognize the following four histological subtypes: conventional (also called solid or multicystic), unicystic, desmoplastic, and peripheral (extraosseous). Current evidences support the contention that peripheral ameloblastoma is
the most common epithelial odontogenic tumor of the gingival/
alveolar mucosa, but it represents 4.5% of ameloblastomas. It is
characterized by a histological picture that can be superimposed
on follicular ameloblastoma, that is an unicystic subtype. The
surface of the peripheral ameloblastoma may be ulcerated, usually does not infiltrate the bone and does not present radio logically with features of radio transparency. It is limited to the gum
or alveolar mucosa; it infiltrates the surrounding tissues, mostly
the gum connective tissue, but does not involve the underlying
bone. Peripheral ameloblastoma originates from residues of the
dental plate, the so-called glands of Serres, pluripotent cells located in the basal cell layer of the mucosal epithelium and in the
minor salivary glands and often a continuity with the basal cells
of the gingival epithelial plate. Almost all oral pathologists and
dentists are experienced in diagnosing peripheral/extraosseus
ameloblastoma but unfortunately, several authors chose to use
the terminology “peripheral alveolar type or typical epulis” for
ordinary intraosseous ameloblastomas that breached the alveolar bone, grew in the gingiva and exhibited the same clinical appearance as epulis. The most common clinical presentation is a
painless and gradually growing swelling, not involving mandibular
bone. Peripheral ameloblastoma usually shows several histologic
characteristics of an intraosseous infiltrating ameloblastoma, but
the disease with histologically low-grade malignant features is extremely rare. Extraosseous ameloblastoma was first reported in
the literature by Kuru in 1911 [1], and nowadays a case report by
Stanley and Krogh published in 1959 is considered to be the first
well-established case of peripheral ameloblastoma [2]. Even more
frequently extraosseous ameloblastoma is an incidental finding
during a routine dental examination; as such, to make the correct
diagnosis at its first presentation is always challenging for medical
doctors. More specific radiological imaging modalities, such as a
CT scan and MRI, should be included in the diagnostic process
as they can most of the time demarcate the lesions better than
a traditional bi dimensional orthopantomography performed by
the dentist. This is because in most cases, the lesions are located
near the bone and within the normal tissue margins. Bone involvement of the peripheral ameloblastoma is usually represented by cupping or saucerization that refers to a depression made
from the pressure of the tumor on the bone. However, patients
affected by peripheral ameloblastoma with bone involvement are
a rare finding and it is usually mild with no neoplastic invasion
or marrow infiltration. Thanks to the dense fibrous tissue of the
gingiva and periosteum and the cortical plate of the alveolar process, a well defined physical barrier could be represented to the
bone infiltration of the peripheral ameloblastoma. The biological
features of peripheral ameloblastoma are similar with that of a
hamartoma or persistent hyperplasia rather than that of a neoplasm. Moreover, the clinical characteristic of peripheral ameloblastoma, for example the course of disease, lesion growth and
patient symptoms, are not specific for peripheral ameloblastoma
and this makes it difficult to distinguish between this kind of neoformation and other type lesions growing on the gingival mucosa.
Neoformations that should be considered with similar manifestation could be epulis, fibroma, squamous cell carcinoma, and lymphoma and all of these are lesions that should be investigated
when thinking about differential diagnosis. For intraoral lesions,
ultrasonic examination is rarely performed and the tumor could
be incorrectly diagnosed as epulis or periapical fistula. This makes
this way of studying this lesion not reliable in helping for peripheral ameloblastoma diagnosis. Instead, the diagnosis of PA should
be considered if: the mass grows slowly without pain and trismus;
no cauliflower-like changes in the superficial mucosa could be observed; less mucosal lesion than submucosal mass is represented;
CT scan imaging or MRI shows clear demarcation between bone
and medial pterygoid muscle, uniform density and less enhanced
images. In these cases, fine needle aspiration or incisional biopsy
is strongly recommended to prevent unnecessary surgical intervention such as overtreatment. When approaching small lesions,
conservative supra-periosteal surgical excision with an adequate
margin free from disease is recommended even in case diagnosis
is not confirmed. While when large lesions are approached, incisional biopsies should be performed since differential diagnosis
include malignant tumor before proceeding with surgical procedures. Partial bone should be resected if cup-like or saucerized
bone involvement is detected during surgery. Anyway, after surgical treatment, continuous follow up is necessary due to the possibility of late recurrence or malignant changes, even if they are
rarely described.
Materials and methods
A 31-year-old female was referred to Maxillo-facial Surgery Department, University of Siena, in July 2020 from her dentist. The
patience reported the presence of a mandibular growth, that she
first noticed one month earlier. She presented no pain or bleeding
in that area. Anamnestic information about the patient revealed
that patient has no systemic disease and no drug use; she also
reported no use of cigarette and alcohol. Thanks to an extraoral
examination a swelling in the left emimandible region was detected. No lymphadenopathy was noticed. Through the intraoral
examination the presence of a swelling, that spanned from the
left second premolar to the left third molar region was observed;
sizes were around 3 x 1,5 cm and overlying mucosa was flushed.
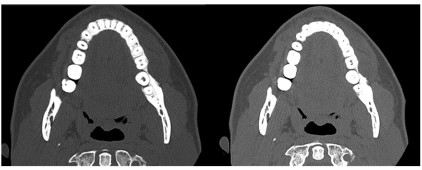
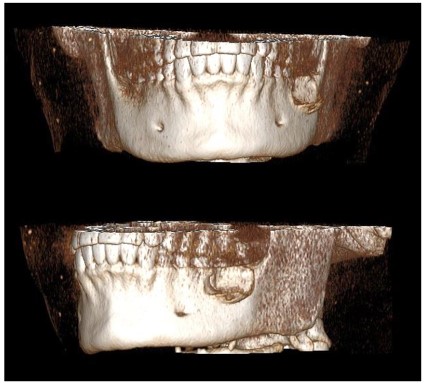
No intraoral fistula was noticed and there was no pain at the palpation of the lesion. A dental CT scan was performed by the patience. The radiological examination confirmed the presence of
an osteolytic unicystic lesion ranged from left second premolar
to left third molar in mandibular bone; no cortical bone invasion
was observed (Figures 1-3). According to clinical and radiological
evidences, the authors decided to proceed with lesion removal.
Results
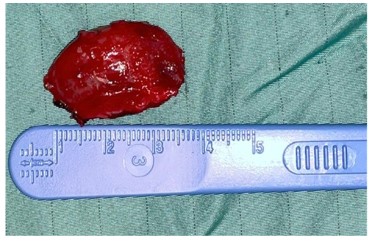
In September 2020 a surgical procedure was performed. Using transoral approach, after local anesthesia infiltration, an interpapillary incision was performed between first premolar and
retromolar trigone of left hemimandible. The unycistc lesion was
identificated, adherent to cortical bone and excised (Figures 4,5).
Moreover, the lesion was formalin-fixed and prepared for being
submitted to a definitive histological examination. No major or
minor intraoperative complications had occurred and the operative time was around 1 hour and half. The patient hospitalization
lasted for about 1 night. After clinical, histological and radiological
examinations lesion was described as a “peripheral unicystic ameloblastoma with intraluminal growth”. At the follow-up examination scheduled two weeks later there was no recurrence and
patient had no complaint. At the follow-up performed one month
and two months after the excision there’s was still no evidence
of recurrence. Further surgical approach (a radical resection) was
deemed unnecessary and wound healing was good (Figure 6). Additionally, patient was informed about the importance of regular
follow-up that were made during one year after excision for early
diagnosis of possible recurrences. After two months the lesion
area was clinically unchanged. A second CT performed 10 months
later did not show the superficial bone resorption, confirming the
tumor was not infiltrating the bone. Patient consent form was obtained by the patient for participation in this case report.
Discussion
Ameloblastoma represents 1% of all oral tumors and 11% of
odontogenic tumors [3]. Current evidence supports the contention that PA is the most common epithelial odontogenic tumor
of the gingiva/ alveolar mucosa [4]. Most ameloblastomas are
characterized by benign behavior and slow growth, with features
of local aggression due to their infiltrative ability that can result
in significant clinical conditions that may require an aggressive
surgical approach. Ameloblastomas are considered locally aggressive tumors that through bone can also invade surrounding soft
tissues if not treated in time, however, ameloblastoma remains
a benign tumor, therefore lymph node or distant metastases are
rare and it define the behavior of the neoplasm as malignant, as
happens in less than 1% of cases. Most of patients usually present
symptoms for the first time between the ages of 30 and 40 years;
according to literature, our case patient was in fact 31 years old.
Despite African people may often present it at an earlier appearance; this tumor has been reported to be more prevalent in Asian
or African-Caribbean individuals which was another characteristic
of our patient. New neoformations can be classified depending
by histological features, and, according to the most recent World
Health Organization (WHO) classification system [5], it is possible
to distinguish four types of ameloblastoma: conventional (also
called solid or multicystic), unicystic, desmoplastic, and peripheral (extraosseous). Peripheral ameloblastoma (PA) represents a rare subtype, comprising only 1% to 5% of all ameloblastomas,
and it features more benign behavior than other types, characterized by minimal bone involvement. This makes diagnosis of the
peripheral subtype an important finding because treatment may
consequently be much more conservative. Moreover, peripheral
ameloblastomas are generally common at one location. Only Hernandez et al. reported one case that was placed at two different
locations at the same time [6]. These benign tumors usually occur
primarily in mandibular premolar area, followed by lower anterior
and maxillary tuber areas. Mean age of appearance is 52.1, but
it can be seen at ages raging from 9 to 92. In contrast to other
ameloblastomas subtypes, they are more common in men with a
male/female ratio of 1.9:1 [7]. The most common presentation is
a painless and gradually growing swelling. The deep margin does
not tend to invade bone extensively, nevertheless radiographically
it may result as a scalloped lesion. On the other hand, sometimes
peripheral ameloblastoma could invade bone structures, create
nerve damage that could involve inferior alveolar nerve. However, innovative microsurgical repairing techniques exist today to
fix the issue [8,9]. Peripheral ameloblastoma differential diagnosis should include reactive swelling such as peripheral giant cell
granuloma, peripheral odontogenic fibroma, peripheral ossifying fibroma, papilloma, pyogenic granuloma, epulis, and fibroma
[10]. Basal cell carcinoma of the gingiva is also considered as an
analogous neoformation to peripheral ameloblastoma. However,
the way these diseases manifest is similar. Radiological and histological investigations are necessary to make differential diagnosis
through specific characteristics. Malignant transformation of the
PA is exceedingly rare [11].
Consequently, 3-dimensional imaging such as Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) helps to
demarcate the lesions accurately. Despite this characteristic appearance, certain diagnosis requires histological examination to
exclude other peripheral odontogenic tumors. In this case patient’s characteristic and radiological findings were suggestive
of peripheral ameloblastoma so the authors decided to proceed
with surgery without histological diagnosis. Rationale for the
management has been questioned. In many cases, the traditional
approach using extensive resection is avoided in favor of the more
conservative techniques. However, due to its rarity, there is no
strong consensus relating to the surgical margins and, although
less aggressive than other types of ameloblastoma, excision using
a local conservative approach [12] or more extensive aggressive
treatment [13] has been suggested.
Conclusion
The purpose of this case report is to present our surgical equipe experience approaching a rare pathology. In the reported case
PA appeared as a swelling range from left second premolar and
left third molar region and the patient didn’t have symptoms. According to literature, after the tumor was locally excised and during follow-up, no bone’s invasion was observed, confirming the
lesion was completely extra osseus. Further surgical approaches
were judged as unnecessary over treatments. Although recurrence rate of peripheral ameloblastomas are low, long-term follow-ups are suggested [14]. It was reported that a benign peripheral ameloblastoma was recurrated as an ameloblastic carcinoma
[15]. Additionally, a metastatic peripheral ameloblastoma and a
recurrence of a peripheral ameloblastoma which shows dysplasia was reported too [16,17]. Due to such information, long term and
regular controls should be mandatory.
Declarations
Conflicts of interest: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funding: The authors report no involvement in the research by
the sponsor that could have influenced the outcome of this work.
Authors’ contributions: All authors contributed equally to the
manuscript and read and approved the final version of the manuscript.
References
- Kuru H. Ueber das adamantinom. Zentralblatt für allgemeine.
Pathol Anat.1911; 22: 291-295.
- Stanley H, Krogh H. Peripheral ameloblastoma; report of a case.
Oral Surg Oral Med Oral Pathol.1959; 12: 760-765.
- Bertossi D, Favero V, Albanese M, De-Santis D, Martano M, et al.
Peripheral ameloblastoma of the upper gingiva: report of a case
and literature review. J Clin Exp Dent. 2014; 6: e80-84.
- Vered M, Muller S, Heikinheimo K. Ameloblastoma, extraosseous/
peripheral type. In: El-Naggar AK, Chan JKC, Grandis JR, Takata
T, Slootweg PJ, editors. WHO classification of head and neck tumours. 4th ed. Lyon: IARC; 2017; 218.
- El-Naggar AK, Chan JK, Grandis JR, et al., editors. WHO classification of head and neck tumours. 4th ed. IARC Publications; 2017.
- Hernandez G, Sanc G, Caballesp T, Moskow BS. A case of multicentric peripheral ameloblastoma of the gingiva: A light and electron microscopic study. J Clin Periodontol. 1992; 23: 188.
- On D, Kang M, Ryu J, Kang M. Peripheral ameloblastoma of the
pterygomandibular space: a case report. J Oral Maxillofac Surg
Med Pathol 2019; 31: 192-195.
- Gennaro P, Chisci G, Gabriele G, Iannetti G. Conservative surgical
and microsurgical techniques for the management of dental implants that impinge on the inferior alveolar nerve. British Journal
of Oral and Maxillofacial Surgery. 2014; 52: 566-568.
- Gennaro P, Gabriele G, Mihara M, Kikuchi K, De Caris F Side-to-end
trigeminal to trigeminal fascicular neurorrhaphy to restore lingual
sensibility: A new technique. Journal of reconstructive microsurgery. 2014; 30: 211-214.
- Philipsen HP, Reichart PA, Nikai H, Takata T, Kudo Y. Peripheral ameloblastoma: biological profile based on 160 cases from the literature. Oral Oncol. 2001; 37: 17-27.
- Baden E, Doyle JL, Petriella V. Malignant transformation of peripheral ameloblastoma. Oral Surg Oral Med Oral Pathol. 1993; 75:
214-219.
- Borrello R, Bettio E, Bacci C, Valente M, Sivolel S, et al. A conservative approach to a peripheral ameloblastoma. Case Rep Dent.
2016; 2016: 8254571.
- Yanamoto S, Yamabe S, Kawasaki G, Mizuno A. et al. Peripheral
ameloblastoma in the maxillary canine region. Asian J Oral Maxillofac Surg. 2005; 17: 195-198.
- Buchner A, Sciubba JJ. Peripheral epithelial odontogenic tumors: a
review. Oral Surg Oral Med Oral Pathol. 1987; 63: 688-697.
- Baden E, Doyle JL, Petriella V. Malignant transformation of peripheral ameloblastoma. Oral Surg Oral Med Oral Pathol. 1993; 75:
214- 219.
- Lin SC, Lieu CM, Hahn LJ, Kwan HW. Peripheral ameloblastoma
with metastasis. Int J Oral Maxillofac Surg. 1987; 16: 202-204.
- Wettan HL, Patella PA, Freedman PD. Peripheral ameloblastoma:
review of the literature and report of recurrence as severe dysplasia. J Oral Maxillofac Surg. 2001; 59: 811-815.