Introduction
Studies show that hip fracture is a global problem and is common among the elderly. A study stated that the incidence rate of
hip fracture is as high as 171/100000 [1]. The study also stated
that the risk of hip fracture increases with increasing lifespan. As
a result, the elderly patients tend to have worse prognoses and
longer recovery time than the younger ones [2]. The estimated
12-month mortality among elderly patients with hip fractures is
about 27% to 30% [3]. In addition to the high mortality rate, taking care of patients with hip fractures is an expensive endeavor. It
places a substantial burden on social healthcare resources [4,5].
Therefore, several scholars are concerned with improving the
prognosis of patients with hip fractures.
After studying many factors, researchers have since turned
their attention to the timing of surgery and concluded that early
surgery has no effect on the outcomes of hip fracture patients [6].
For instance, Gökhan Karademir said that there is no significant
difference in mortality between patients who undergo surgery
within five days and those who undergo surgery after five days
[7]. Nonetheless, other researchers like Paul Welford concluded
that performing surgery on patients within 24 hours can reduce
the mortality rate [8]. A study conducted by Zachary Tran showed
that delayed operation (time to surgery ≥48 h) increases the likelihood of mortality [9]. Notably, even among researchers who support early surgery, the relationship between time to surgery and
the exact prognosis is controversial.
Materials & methods
To review the literature on waiting time before surgery for patients with hip fractures, a comprehensive search was performed
in PubMed and Web of Science between the 19 December, 2011
and the 19 December, 2021. The search strategy included the following terms: (Hip fracture) OR (Trochanteric Fractures) OR (Fractures, Trochanteric) OR (Fractures, Hip) OR (Intertrochanteric
Fractures) OR (Subtrochanteric Fractures) OR (Fractures, Intertrochanteric) OR (Fractures, Subtrochanteric)) AND (Early Operation)
OR (Delayed Surgery) OR (Delayed Operation) OR (Early Surgery))
AND (Rehabilitation) OR (Habilitation).
A total of 834 articles were found, and 241 duplicate articles
were excluded from the study. Additional 558 unrelated articles
were excluded from the study after reading the title and abstract.
Furthermore, seven articles were excluded from the study for several reasons. First, we excluded articles that mentioned the concept of a delayed or early operation but did not study it. Second,
we excluded articles that lacked the time boundary between early
and delayed operation and those with multivariable interaction.
After all the exclusions, 15 articles were included in this study.
Results
In a retrospective cohort study published by Daniel Pincus [10],
in 2017, 42230 patients who underwent hip fracture surgery from
2009 to 2014 were included. The patients were assigned into two
groups. One group comprised patients whose waiting time before
surgery was less than 24 hours and the other group comprised
patients whose waiting time before surgery was more than 24
hours. After matching the baseline characteristics of the patients
in the two groups, the average age was 80.1. In the analyses of
outcomes, mortality (30 days, P=0.006; 90 days, P<0.001; 12 months, P<0.001), pneumonia (P=0.002), pulmonary embolism
(P<0.001), myocardial infarction (P<0.001) showed significant differences and deep venous thrombosis (P=0.86) showed no significant differences. In another article, Daniel Pincus, MD, states
that when the waiting time for surgery is more than 24 hours, it
significantly increases the length of stay (P=0.006) and the medical expenses (P<0.001).
In a randomized controlled trial published by Flavia K Borges
in 2020, 2970 patients who underwent hip fracture surgery from
2014 to 2019 were included [11]. The patients were assigned into
two groups. One group comprised patients whose waiting time
before surgery was about 6 hours and the other group comprised
patients whose waiting time before surgery was about 24 hours.
All patients in this study were above 45 years. In the analyses of
outcomes, stroke (P=0.047), delirium (P=0.009), urinary tract infection, moderate to severe pain on day 4-7 showed significant
differences and mortality (90 days, P=0.40), myocardial infarction
(P=0.77), pressure ulcer (P=0.46), infection (P=0.08) showed no
significant differences. In conclusion, advancing the operation to
about 6 hours will be better than 24 hours.
In a retrospective cohort study published by Alejandro L in
2018, 1234 patients who underwent hip fracture surgery from
2011 to 2016 were included [12]. The patients were assigned into
three groups. Group one comprised patients whose waiting time
before surgery was less than two days. Group two comprise patients whose waiting time before surgery was more than two days
with medical reasons and group three comprised patients whose
waiting time was also more than two days but with organizational reasons. The average age of the three groups was 83.5, 83.3
and 82.4, respectively. In the analyses of group 1 and group 3,
mortality (6 months, P=0.027; 12 months, P=0.002), pneumonia
(P=0.042), urinary infection (P=0.017), pulmonary exacerbation
(P=0.001) showed significant differences and 30-day mortality,
deep venous thrombosis, renal insufficiency, wound infection,
dementia, cardiac arrhythmia, myocardial infarction, thromboembolism, stroke, gastrointestinal bleeding showed no significant
differences. However, in the analyses of group 1 and group 2,
mortality and complications didn’t have significant differences. In
conclusion, the prognosis of surgical patients who are delayed for
organizational reasons will be worse.
In a retrospective cohort study published by Boris Sobolev
Ph.D. in 2018, 139119 patients who underwent hip fracture surgery from 2004 to 2012 were included[13]. All the patients in
this study were above 65 years. The patients were assigned into
four groups. The patients who underwent surgery on admission
day were assigned group 1; patients operated on the second day
were assigned group 2; patients operated on the third day were
assigned group 3; and patients operated after the third day were
assigned group 4. In the analyses of outcomes, compared with
patients operated on admission day, 30-day mortality of those
operated on the third or after the third day showed significant
differences. But those operated on the second day showed no
significant differences. In conclusion, surgery within 48 hours can
decrease the 30-day mortality.
In a prospective cohort study published by Chris A. Anthony
in 2017, 8254 patients who underwent hip fracture surgery from
2005 to 2010 were included[14]. The study placed the subjects into two cohorts. One cohort is operation ≤2 days undergoing all
surgery and operation >2 days undergoing all surgery. The other
cohort is operation ≤2 days except for total hip arthroplasty and
operation >2 days except for total hip arthroplasty. All the patients in this study are above 60 years. In the analyses of cohorts,
two cohorts reached a similar conclusion. Pneumonia (in cohort
1, P=0.009; in cohort 2, P=0.010), myocardial infarction (in cohort
1, P=0.015; in cohort 2, P=0.025), stroke (in cohort 1, P=0.018; in
cohort 2, P=0.031), cardiac arrest (in cohort 1, P=0.043; in cohort
2, P=0.039), sepsis (in cohort 1, P=0.010; in cohort 2, P=0.008),
septic shock (in cohort 1, P=0.010; in cohort 2, P=0.007) showed
significant differences and mortality (30 days), pulmonary embolism, deep venous thrombosis, infection, renal insufficiency, deep
wound infection, organ space infection, superficial infection,
wound dehiscence, unplanned intubation, urinary tract infection,
acute renal failure, coma >24 hours, bleeding transfusions, peripheral nerve injury showed no significant differences. In conclusion, surgery within 24 hours improves the prognosis.
In a retrospective cohort study published by Giulio Piol in 2019,
939 patients who underwent hip fracture surgery from 2012 to
2015 were included [15]. All patients in this study were above 75
years. Patients were assigned into three groups. Group one comprised patients who underwent surgery within one day. The second group comprised patients who underwent surgery within two
days and the third group comprised patients who underwent surgery after more than three days. In the disturbance of consciousness group before the operation, delayed operation showed no
significant differences. In the mild disturbance of consciousness
group before operation, delayed operation (≤2 days, P=0.009; >2
days, P=0.002) showed significant differences. In conclusion, surgery within 2 days can improve the prognosis.
A prospective cohort study by Defei Meng in 2021, included
480 patients who underwent hip fracture surgery from 2016 to
2017 [16]. The average age of the patients in this study was 65
years. The researcher divided the patients into three groups. Patients operated within 2 days were assigned group one, patients
operated within 7 days were assigned group two and patients
operated after seven days were assigned group. There was no
significant difference in the 12-month mortality and mobility between groups one and two. However, the analysis of group one
and group three showed a significant difference in the12-month
mortality (P=0.020) and mobility (P=0.027). This study concluded
that performing surgery within 7 days can improve the prognosis
of hip fracture.
A retrospective cohort study published by Takahisa Ogawa in
2019, included 175 patients who underwent hip fracture surgery
from 2013 to 2015 [17]. The researcher assigned patients into two
groups. One group comprised patients whose waiting time before
surgery was less than 24 hours and the other group comprised
patients whose waiting time is more than 24 hours. The average
age of the two groups was 86.7 and 85.4, respectively. The study
showed that patients whose waiting time before surgery was less
than 24 hours had better mobility than those whose waiting time
was more than 24 hours. The study concluded that shorter waiting time before surgery for patients with hip fracture promotes
mobility rehabilitation and reduces mortality.
In 2021, Obada Hasan conducted a case-cohort study that included 911 patients who had undergone hip fracture surgery between 2010 and 2018 [18]. The average age of the patients in this
study was 50 years. The patients were assigned into four groups
based on the waiting time before surgery and whether they were
transferred to ICU after the operation. In the analyses of outcomes, postoperative ICU (P=0.37) showed no significant differences. In conclusion, surgery within 48 hours has no relationship
with postoperative ICU.
A study conducted by Nathalie Declarador in 2018 included
450 patients who had undergone hip fracture surgery between
2011 and 2012 [19]. The patients were assigned into two groups.
Group one comprised patients whose waiting time before surgery
was less than 48 hours and group two comprised patients whose
waiting time was more than 48 hours. The average age for the
two groups was 79.3 and 80.6, respectively. In the analyses of
outcomes, 12-month mortality (P=0.03), primary complications
(urinary tract infection and pneumonia, P<0.01), length of stay
(P<0.01), mobility (P=0.030) showed significant differences but
in-hospital mortality (P=0.16) showed no significant differences.
In conclusion, surgery within 48 hours can improve the prognosis.
A retrospective cohort study by Luigi de Palma in 2014 comprised 1169 patients who had undergone hip fracture surgery between 1995 and 2008 [20]. All the patients in this study were above
65 years. The researcher placed the patients into two groups. The
first group comprised patients whose waiting time was less than
48 hours and the second group comprised patients whose waiting time was more than 48 hours. In the analyses of outcomes,
30-day mortality (P<0.001) showed significant differences. In
conclusion, surgery within 48 hours improves the prognosis.
In 2017, Natasha Morrissey conducted a study that comprised
1880 patients who had undergone hip fracture surgery between
2011 and 2015 [21]. The average age of patients in this study was
83.9. The study showed that there is no significant difference in
the 30-day mortality and length of stay when patients are divided
into groups depending on the 12 or 18 hour waiting time before
surgery. However, the study showed that there is a significant difference in the 30-day mortality when patients are divided into
groups based on longer waiting times of more than 24 hours or
36 hours. The study concluded that performing surgery within 24
hours positively impacts the mortality rate of patients with hip
fracture after the operation.
In 2016, Andre M Samuel conducted a study that involved 1361
patients who had undergone hip fracture surgery between 2011
and 2012 [22]. Unlike most of the studies, Andre selected patients
that were less than 50 years. The patients were assigned into two
groups. The first group comprised patients whose waiting time
was less than 24 hours and the second group comprised patients
whose waiting time was more than 24 hours. In the analyses of
outcomes, adverse events (serious adverse events: thromboembolic event, acute respiratory distress syndrome, unplanned return to the operating room, cardiac arrest (requiring CPR), severe
sepsis, cerebrovascular accident, death, myocardial infarction;
minor adverse events: pneumonia, urinary tract infection, drug/
ethanol withdrawal, unplanned intubation, acute kidney injury,
surgical site infection, decubitus ulcer, compartment syndrome,
unplanned return to ICU line-associated bloodstream infection, osteomyelitis) showed significant differences. In conclusion, surgery within 24 hours can improve the prognosis.
In 2019, Gurger conducted a retrospective study that comprised 324 patients who had undergone hip fracture surgery between 2015 and 2016 [23]. The patients were assigned into three
groups. Two groups comprised of patients whose waiting time
was are less than 72 hours and the third group comprised of patients whose waiting time was more than 72 hours. The average
age of the three groups was 79.3. In the analyses of outcomes,
1-year mortality showed significant differences. In conclusion,
surgery within 72 hours decreases the mortality rate.
Discussion
This study included 15 studies: nine retrospective studies, one
randomized controlled trial, one case-control study, and 4 four
prospective studies. The paper used these collected articles to assess the impact of waiting time before surgery for patients with
hip fracture. The goal of the paper was to improve prognosis of
hip fracture. The specific characteristics are as shown in Table 1.
In all the papers included in this study, the researchers divided
the patients into two or more groups depending on their waiting
time before surgery. After assigning the patients into groups, the
researchers then performed a prognosis analysis to determine
whether there is a significant difference between the groups with
different waiting time before surgery. Except for Obada Hasan’s
research, all the other articles concluded that the waiting time
before surgery impacts the prognosis of hip fracture. The studies
stated that patients with delayed surgery have higher mortality,
more complications, higher costs and longer hospital stay than
patients with shorter waiting time before surgery. Moreover, the
studies stated that patients whose waiting time before surgery
is longer are less likely to recover to preoperative mobility. Unlike all the other studies, Obada Hasan’s research concluded that
several factors aside from the timing of the surgery influence the
occurrence of critical postoperative illness in patients with hip
fractures. Based on the literature reviewed, this paper concludes
that the waiting time before surgery does not determine whether a patient will be taken to ICU after the surgery, but it influences
the patient’s mortality rate and the occurrence of complications.
Nonetheless, studies have shown that early surgery is beneficial
to patients with hip fractures. This study found that performing
hip fracture surgery within 24 hours had no effect on most prognostic indicators. However, it still influenced the occurrence of
delirium, stroke, infection without sepsis, urinary tract infection,
4-7-day moderate-to-severe pain. Additionally, the study found
that 30-day mortality, 90-day mortality, 12-month mortality,
pneumonia, myocardial infarction, pulmonary embolism, length
of hospital stay, delirium and mobility are affected when the operation is postponed to more than 24 hours. Nonetheless, the
events that occur when the surgery is delayed for more than 48
hours to those that occur when the surgery is delayed by 24 hours.
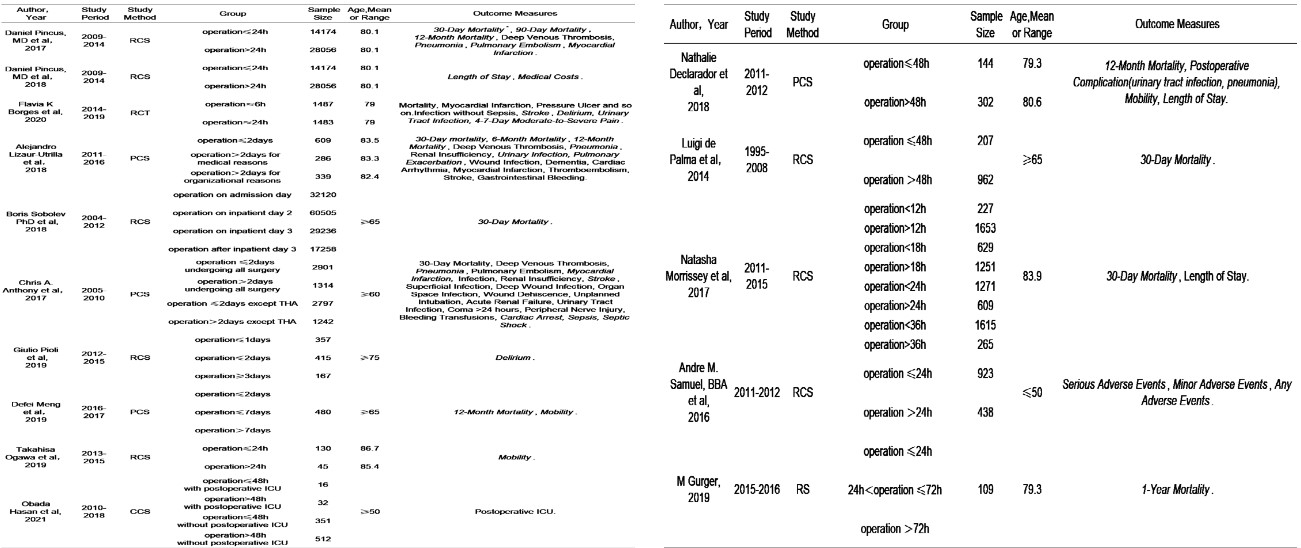
Table 1: Characteristic of individual study.
RCS; Retrospective Cohort Study; RS; Retrospective Study; PCS; Prospective Cohort Study; CCS; Case Cohort Study; RCT; Randomized Controlled
Trial; THA; Total Hip Arthroplasty; ICU; Intensive Care Unit. *Italic means that the index is statistically significant and the others mean that they are
no statistically significant.
Finally, the study found that the most critical surgery time for
hip fracture patients should be within 24 hours. The patients undergoing surgery during this period should be closely monitored
for the development of delirium, stroke, non-septic infection and
moderate to severe pain in 4-7 days after surgery. Moreover, patients who postpone the operation by 24 hours for various reasons, more attention should be monitored for the development
of pneumonia, pulmonary embolism, myocardial infarction. Furthermore, patients who delay the operation by 48 hours should
be monitored not only for pneumonia, pulmonary embolism and
myocardial infarction but also for sepsis and arrhythmia.
The advantage of this article is that it treats the problem from a
new perspective and accurately predicts the complications which
promotes recovery. This study also has some limitations. First,
the articles in this study were retrieved from only two databases;
PubMed and Web of Science. As a result, there are still some studies about the waiting time for hip fracture surgery that have not
been included. For this reason, therefore, the information included in this paper might be incomplete. The other limitation for this
study is that it included articles that are not more than 10 years.
This limitation affects the inclusion of articles which also limits the
information and conclusion derived from the studies.
Conclusions
The time within which patients with hip fracture undergo surgery is critical. According to studies conducted by various scholars, patients with hip fractures must undergo surgery within 24
hours to prevent the occurrence of postoperative complications
such as pneumonia and myocardial infections. Delaying the surgery of patients with hip fractures increases the risk of developing
postoperative complication and increases the patient’s mortality
rate. Nonetheless, the occurrence of postoperative complications
is influenced by the waiting time. For instance, patients who take
less than 48 hours to undergo surgery experience less severe
postoperative complications than those that delay the surgery by
more than 48 hours.
Declarations
Conflict of interest: The authors declare that there are no conflicts of interest.
Funding: This work was supported by Health Commission of
Zhejiang Province (Grant No. 2021RC128).
Acknowledgements: We thank our colleagues from Huzhou
Central Hospital for their support in conducting this review.
References
- Adeyemi A, Delhougne g. Incidence and Economic Burden of Intertrochanteric Fracture: A Medicare Claims Database Analysis. JB JS
Open Access. 2019; 4: e0045
- Ortiz-Alonso FJ, Vidán-Astiz M, Alonso-Armesto M, Toledano-Iglesias, Alvarez-Nebreda L. The pattern of recovery of ambulation
after hip fracture differs with age in elderly patients. J Gerontol A
Biol Sci Med Sci. 2012; 67: 690-697
- Zhang R, Yang Z, Lei T, Ping Z, Bai G. Effects of aminocaproic acid
on perioperative hidden blood loss in elderly patients with femoral
intertrochanteric fracture treated with proximal femoral nail anti-rotation. J Int Med Res. 2019; 47: 5010-5018.
- Marques A, Lourenço O, da Silva JAP. The burden of osteoporotic
hip fractures in Portugal: costs, health related quality of life and
mortality. Osteoporos Int. 2015; 26: 2623-30
- Hartholt KA, van Beeck EdF, Polinder S, van der Velde N, van
Lieshout EMM. Societal consequences of falls in the older population: injuries, healthcare costs, and long-term reduced quality of
life. J Trauma. 2011; 71: 748-753
- Mirbolook A, Siavashi B, Jafarinezhad AE, Jahromi SK, Farahmand
M. Subtrochanteric Fractures: Comparison of Proximal Femur
Locking Plate and Intramedullary Locking Nail Fixation Outcome.
Indian J Surg. 2015; 77: 795-798
- Karademir G, Bilgin Y, Erşen A, Polat G, Buget MI. Hip fractures in
patients older than 75 years old: Retrospective analysis for prognostic factors. Int J Surg, 2015; 24: 101-104
- Welford P, Jones CS, Davies G, Kunutsor SK, Costa ML. The association between surgical fixation of hip fractures within 24 hours and
mortality : a systematic review and meta-analysis. Bone Joint J.
2021; 103: 1176-1186.
- Tran Z, Hsiue PP, Pan C, Verma A, Rahimtoola R. Impact of delayed
intervention on clinical outcomes following traumatic hip fracture
in the elderly: A national analysis. J Orthop. 2021; 27: 74-78.
- Pincus D, Wasserstein D, Ravi B, Huang A, Paterson JM. Medical
Costs of Delayed Hip Fracture Surgery. J Bone Joint Surg Am. 2018;
100: 1387-1396.
- HIP ATTACK Investigators. Accelerated surgery versus standard
care in hip fracture (HIP ATTACK): an international, randomised,
controlled trial. Lancet, 2020; 395: 698-708.
- Lizaur-Utrilla A, Gonzalez-Navarro B, Vizcaya-Moreno MF, Miralles
Muñoz FA, Gonzalez-Parreño S. Reasons for delaying surgery following hip fractures and its impact on one year mortality. Int Orthop. 2019; 43: 441-448.
- Sobolev B, Guy P, Sheehan KJ, Kuramoto L, Sutherland JM. Mortality effects of timing alternatives for hip fracture surgery. Cmaj,
2018; 190: E923-e932
- Anthony CA, Duchman KR, Bedard NA, Gholson JJ, Gao Y. Hip Fractures: Appropriate Timing to Operative Intervention. 2017; 32:
3314-3318.
- Pioli G, Bendini C, Giusti A, Pignedoli P, Cappa M. Surgical delay is a
risk factor of delirium in hip fracture patients with mild-moderate
cognitive impairment. Sabetta. Aging Clin Exp Res. 2019; 31: 41-47.
- Meng D, Bai X, Wu H, Yao S, Ren P. Patient and Perioperative Factors Influencing the Functional Outcomes and Mortality in Elderly
Hip Fractures. J Invest Surg. 2021; 34: 262-269.
- Ogawa T, Aoki T, Shirasawa S. Effect of hip fracture surgery within
24 hours on short-term mobility. J Orthop Sci. 2019; 24: 469-473.
- Hasan O, Mazhar L, Rabbani U, Rabbani A, Mahmood F. Does early
surgery prevent Postoperative ICU admission after surgery for the
fracture of the hip. Nested case control study of 911 patients. Ann
Med Surg (Lond), 2021; 61: 35-40.
- Declarador N, Ramason R, Tay L, Lim William Chan W, Kwek EBK. Beyond comanaged inpatient care to community integration: Factors
leading to surgical delay in hip fractures and their associated outcomes. J Orthop Surg (Hong Kong). 2018; 26: 2309499018783909.
- de Palma L, Torcianti M, Meco L, Catalani A, Marinelli M . Operative delay and mortality in elderly patients with hip fracture: an
observational study . Eur J Orthop Surg Traumatol, 2014; 24: 783-8.
- Morrissey N, Iliopoulos E, Wais Osmani A, Newman K. Neck of femur fractures in the elderly: Does every hour to surgery count?
Injury. 2017; 48: 1155-1158.
- Samuel AM, Russo GS, Lukasiewicz AM, Webb ML, Bohl DD. Surgical Treatment of Femoral Neck Fractures After 24 Hours in Patients
Between the Ages of 18 and 49 Is Associated With Poor Inpatient
Outcomes: An Analysis of 1361 Patients in the National Trauma
Data Bank. J Orthop Trauma. 2016; 30: 89-94.
- Gurger M. Factors impacting 1-year mortality after hip fractures in
elderly patients: A retrospective clinical study. Niger J Clin Pract.
2019; 22: 648-651.