Introduction
Uveitis-glaucoma-hyphema (UGH) syndrome is a triad characterized by recurrent episodes of elevated intraocular pressure
(IOP), anterior chamber (AC) hemorrhages, AC inflammation, and
blurred vision. UGH syndrome or Ellingson’s syndrome was first
described in 1978, and it is generally associated with contact between a malpositioned AC intraocular lens (IOL) and the iris or
ciliary body, leading to mechanical tissue trauma [1,2]. UGH syndrome is a severe complication of cataract extraction and a cause
for blurry vision weeks to months after surgery. Currently, with
the upgrades in lens design, surgical techniques, and the IOL is implanted into the capsular bag, minimizing the possibility of the IOL
contacting the uvea and reducing the incidence of UGH syndrome
(from 2.2-3 to 0.4-1.2%) [3-5].
In the report, we present an application of aqueous humor
(AH) cytokines and AC cells analysis in a case of an UGH. Ethical
approval for this study was provided by the Ethics Committee of
affiliated eye hospital of Shandong University of Traditional Chinese Medicine and written informed consent was obtained from
the patient. The study and data collection conformed with the
principles of the Declaration of Helsinki. Informed consent was
obtained from the patient for the publication of this study.
Case presentation
Participants
A 51-year-old male was presented to the affiliated ophthalmic
hospital of Shandong university of Traditional Chinese Medicine,
Jinan, China in June 2021 due to right reduced visual acuity, eye
redness and pain that had repeatedly appeared in the past 8
years, and the symptoms were aggravated for 2 days. The patient
reported that he had undergone uneventful phacoemulsification with implantation of a posterior chamber in-the-bag ReSTOR
multifocal lenses (model SN6AD1, Alcon Laboratories, Inc., Fort
Worth, TX, USA) in his right eye in 2013 at his local hospital, 8
years before presentation. The patient repeatedly presented with
decrease of visual acuity, eye redness in the right eye after surgery.
He was diagnosed as uveitis at other hospitals and the symptoms
improved slightly after hormone treatment. Six years later (2019
year), a cataract surgery was performed on his left eye. A history
of head injury caused by tricycle for 19 years was reported.
Ocular examinations
After careful review of his medical history, a series of detailed ophthalmic examinations were conducted. The visual acuity of 40/100 and the best corrected visual acuity was 60/100
(-0.25/1.25×7) in the right eye. The visual acuity of the left eye
was 20/20. Intraocular pressure (IOP) was 39.7 mmHg OD and 13
mmHg OS.
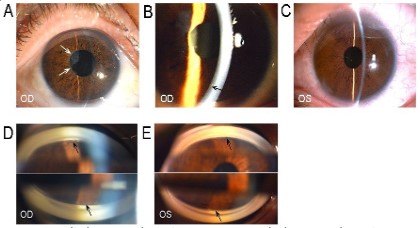
Slit lamp examination in the right eye showed a clear cornea,
diffuse pigmented keratic precipitates, flare in AC (++) and under
natural pupils, the IOL remained centered. The pupils were round
of about 3.5 mm in diameter and pupillary margin organized
membrane. He was found to have 2+ AC cells and his AC showed
no evidence of hypopyon or hyphema on OD (Figure 1A, B). Slit
lamp did not detect any abnormality in the left eye (Figure 1C).
Gonioscopy further revealed all the AC angles were open and pigmentation in the trabecular meshwork of the two eyes, with OD
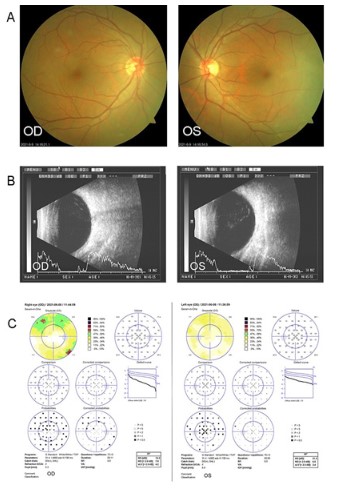
and II OS (Figure 1D, E). Funduscopic examination revealed a vertical cup disc ratio of 0.5 in the right eye. There was no abnormality
in the left eye (Figure 2A). B-scan ultrasound showed an inhomogeneous weak dough like echoes throughout the vitreous cavity
of the right eye (Figure 2B). Automated visual field examination
showed the arcuate scotomas in the superior quadrant in right
eye. Left eye was approximately normal (Figure 2C). Considering
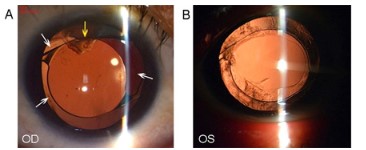
that the patient has undergone IOL implantation, a possible diagnosis of UGH syndrome was proposed. After dilation of the pupil,
we double checked the eyes by slit lamp (Figure 3). The superior
temporal haptic of the right IOL was located outside the anterior
capsule bag, and the inferior nasal haptic of the IOL was located
in-the-bag.
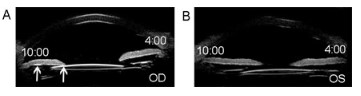
Ultrasound biomicroscopy (UBM) showed the chafing between
the IOL and the posterior surface of the iris at 10-o’clock position
(Figure 4A). Chafing of the posterior iris by the IOL haptic almost
confirmed the diagnosis of UGH syndrome. It was also necessary
to confirm that the AC cells seen under slit lamp were red blood
cells (RBCs).
Surgery and AH Analysis
Considering that the patient was implanted with multifocal IOL
and most of the lens capsule was complete. The optimal treatment modality is to rotate the existing IOL and adjust it into the
capsule bag to remove the chafing between IOL and iris. AH samples (100 to 150 μl) were collected at the beginning of the surgery. Before making the incision, a paracentesis was carried out
at the limbal region using a 1 ml graduated syringe. No bleeding
and contact with peripheral tissue during puncture. AC cells were
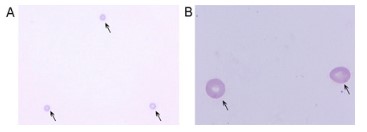
detected by AH smear (Giemsa stain). The specific operation is as Kalogeropoulos CD’s description [6]. The RBCs in the AH were
identified (Figure 5). Cytokines were detected by flow cytometry
cell-based assay. Our findings showed a significantly elevated
concentrations of interleukins 6, 8 (IL-6, IL-8), adhesion molecules
(vascular cell adhesion molecule, VCAM), and basic fibroblast
growth factors (BFGF) (Table 1). The AC RBCs, AH cytokines, high
IOP, and dynamic interactions between IOL and iris determine a
diagnosis of UGH syndrome.
Table 1: The levels of different cytokines in the aqueous humor.
| Cytokine |
Result |
Unit |
Reference range |
| BFGF |
10.1↑ |
pg/ml |
<1.0 |
| VCAM |
1923.9↑ |
pg/ml |
200-1000 |
| IL-8 |
47.9↑ |
pg/ml |
0-20.0 |
#BFGF: basic fibroblast growth factors; VCAM: vascular cell adhesion
molecule; IL-6: interleukins 6; IL-8: interleukins 6.
Follow-up
The patient had resolution of AC inflammation after surgery
(Figure 6A, B). UCVA was 20/20 OD. The IOL was described as centered in-the-bag and UBM showed there was no contact between
IOL and the posterior surface of the iris (Figure 6C). The IOP was
16mmHg OD without IOP lowering medications.
Discussion and conclusions
UGH syndrome is usually an iatrogenic disease. It was initially
described in 1978 as a complication of intraocular friction caused
by first generation AC IOL [7]. It has also been found more recently in subjects submitted to cataract surgery and IOL implantation
(either in the sulcus or in-the-bag) [8]. It is noteworthy that a UGH
syndrome could occur even the IOL remained centered without
dislocation in the state of small pupil. Generally, the clinical signs
and symptoms of these patients were frequently mild in this situation. In this case report, under natural pupils, slit lamp shows that
the IOL remained centered. After full mydriasis, the dislocation of
the haptic of the IOL can be seen. The cause of UGH syndrome in-the-bag IOL is due to large capsulorhexis, the haptics were not in
the capsular bag. The persistent mechanical chaffing between IOL
and iris leads to the spread of iris pigment and the disruption of
blood-aqueous barrier, resulting in the triad of intraocular inflammatory reaction, elevated IOP and AC hemorrhages. Cytokines
trigger and boosts the inflammatory responses in which complement and fibrin enter the eye and are activated by the surface of
the IOL [9]. In our case study, this was evidenced by the organized
membrane of the pupil margin. Elevated IOP can be caused by direct mechanical injury, with clogging of the trabecular meshwork
by pigment or scarring, or by the inflammatory reaction itself.
For ocular lesions with inflammatory compound, the analysis
of cytokines in AH has become extremely attractive for research
[10-13]. However, the expression of inflammatory cytokines in
UGH syndrome has not been reported previously. In this case
report, IL-6, IL-8, VCAM and BFGF concentrations were significantly elevated. BFGF is a member of a family of heparin-bind-
ing growth factors. It is found in normal tissue associated with
heparan sulfate on the cell surface or extracellular matrix. It has
been shown that BFGF accelerates the rate of wound closure by
increasing cell proliferation, promoting tissue angiogenesis, and
inhibiting myofibroblast differentiation [14]. Gallego-Muñoz et
al [15].showed that upon adding TGF-β1 and BFGF to the culture
medium of human corneal fibroblasts, the cellular proliferation
process is strengthened and the myofibroblast differentiation and
cellular migration are remarkably reduced, with TGF-β1 treatment
alone comparison. In addition, at sites of inflammation, BFGF is
released and upregulated by the action of proteases and hepa-
rinases [16]. The increased levels of BFGF are directly related to
the formation of pupillary margin organized membrane, and the
increased levels of BFGF also indicates the presence of inflammatory reaction. VCAM an endothelial receptor belonging to the
immunoglobulin superfamily is associated with the disruption of
the blood-ocular barrier [17]. IL-6 is an interleukin that acts as a
proinflammatory cytokine. It is secreted by macrophages, monocytes and T and B cells to stimulate an immune response during
tissue damage. Previous investigations suggested that IL-6 mediates the inflammatory processes and immune responses in many
eye diseases such as, Behcet’s disease [18], and pseudoexfoliation glaucoma [19]. IL-6 is involved in vascular hyperpermeability
and endothelial barrier dysfunction [20,21]. This suggests a possible involvement of elevated IL-6 levels in the active intraocular
inflammation and break down of the blood–aqueous barrier. IL8 is
an important neutrophil chemotactic factor, which plays a key role
in the defense mechanism through its effects on neutrophil activities [19,22]. Previous studies of inflammatory eye disease [23,24]
have showed that increased levels of IL-6 and IL-8 were associated
with intraocular inflammation. We found similar changes among
these cytokines in the samples from current UGH patients in the
present study. The increased levels of the IL-6, 8 and BFGF suggested active intraocular inflammation.
The treatment of UGH syndrome depends on the clinical signs,
symptoms, and disease severity, and to a lesser extent on the type
and position of IOL. In the mild-to-moderate cases, treatment
with a combination of anti-inflammatory and anti-glaucoma medications might be sufficient. However, for recurrent patients, the fundamental treatment is to eliminate the persistent mechanical
chaffing between IOL and iris and/or ciliary body. For advanced
cases, surgical intervention may be the only option, usually with
a complete IOL repositioning or exchange [25-27]. The technologies of IOL repositioning depends strongly on the severity of ad-
hesion formation between the IOL and the capsular bag. In future
cataract surgery, it is very important to implant IOL in the capsular bag, not ciliary sulcus, with circumferential overlapping of the
appropriately-sized anterior capsule over the optic edges of IOL
to reduce UGH morbidity [28]. In conclusion, medical history, a
necessary UBM, along with a proper assessment of the IOL position were necessary for early diagnosis of UGH. AH cytokines and
AC cells analysis, may offer more useful information for correct
diagnosis of UGH and provide the corresponding laboratory basis
[29-31].
Declarations
Ethics approval and consent to participate: This study complied with the tenets of the Declaration of Helsinki. Ethics approval was not required for the reason that this was a single case
report.
Consent for publication: The written consent obtained from
the patient for any personal or clinical details along with any identifying images to publish in this report. The copy of the written
consent form is available for review by the journal Editor.
Availability of data and materials All data generated or analyzed during this study are included in this published article.
Competing Interest: All authors declare that they have no conflicts of interest.
Funding: This study was supported by the Shandong Tradition-
al Chinese Medicine Science and Technology Development Plan
Project (2021Q096, 2019-0251), Shandong Medical and Health
Development Plan Project (2019ws566) and National Key Research and Development Project (2019YFC1710200).
Authors’ contributions: Xiujuan Du and Xiuyan Zhang were the
major contributors to the drafting of the manuscript. Fang Sha
and Haifeng Ji collected the ophthalmological data. Dongmei Liu
and Yan Liu interpreted the ophthalmological data. The correspondence authors reviewed and approved the final manuscript.
Acknowledgments: Not Applicable.
References
- A YAK, A F Charles J Pavlin, B RC, A F David S Rootman. Uveitis-glaucoma-hyphema syndrome after handmade, anterior chamber
lens implantation. Journal of Cataract & Refractive Surgery. 1997;
23(9): 1414-7
- Ellingson, Thomas F. The uveitis-glaucoma-hyphema syndrome associated with the Mark VIII anterior chamber lens implant. American Intra-Ocular Implant Society Journal. 1978; 4(2): 50-3.
- Badakere SV, Senthil S, Turaga K, Garg P. Uveitis-glaucoma-hyphaema syndrome with in-thebag placement of intraocular lens. BMJ
Case Reports. 2016; 2016: bcr2015213745.
- Foroozan R, Tabas JG, Moster ML. Recurrent microhyphema despite intracapsular fixation of a posterior chamber intraocular lens.
Journal of Cataract & Refractive Surgery. 2003; 29(8): 1632.
- Apple DJ, Mamalis N, Loftfield K, Googe JM, Olson RJ. Complications of intraocular lenses. A historical and histopathological review. Survey of Ophthalmology. 1984; 29(1): 1–54.
- Kalogeropoulos C, Malamou-Mitsi V, Asproudis I, Psilas K. The contribution of aqueous humor cytology in the differential diagnosis
of anterior uvea inflammations. Ocular Immunology & Inflammation. 2004; 12(3): 215–25
- Zvi G, Erez T, Asaf A. Uveitis-Glaucoma-hyphema Syndrome. Nepalese journal of ophthalmology: A biannual peer-reviewed academic
journal of the Nepal Ophthalmic Society: NEPJOPH. 2016; 8(1): 99.
- Hou A, Hasbrook M, Crandall D. A Case of Uveitis-Hyphema-Glaucoma Syndrome Due to EX-PRESS Glaucoma Filtration Device Implantation. Journal of Glaucoma. 2019; 28(10): e159–61.
- Chu AJ. Tissue factor mediates inflammation. Archives of Biochemistry & Biophysics. 2005; 440(2): 123–32.
- Chua J, Vania M, Cheung C, Ang M, Wong TT. Expression profile of
inflammatory cytokines in aqueous from glaucomatous eyes. Molecular Vision. 2012; 18(45–47): 431.
- Borkenstein A, Faschinger C, Maier R, Weger M, Theisl A, et al.
Measurement of tumor necrosis factor-alpha, interleukin-6, Fas
ligand, interleukin-1α, and interleukin-1β in the aqueous humor of
patients with open angle glaucoma using multiplex bead analysis.
Molecular Vision. 2013; 19: 2306–11.
- Hautala N, Glumoff V, Hautala T, Vainio O. IL-2 may possess neuroprotective properties in glaucomatous optic neuropathy. Acta
Ophthalmologica. 2012; 90(3): e246–7.
- Gramlich OW, Beck S, von Thun Und Hohenstein-Blaul N, Boehm
N, Ziegler A, et al. Enhanced Insight into the Autoimmune Component of Glaucoma: IgG Autoantibody Accumulation and Pro-Inflammatory Conditions in Human Glaucomatous Retina. Plos One.
2013; 8(2): e57557.
- Song QH, Klepeis VE, Nugent MA, Trinkausrandall V. TGF-beta1
regulates TGF-beta1 and FGF-2 mRNA expression during fibroblast
wound healing. Mol Pathol. 2002; 55(3): 164-76.
- Gallego-Muñoz P, Ibares-Frías L, Garrote JA, Valsero-Blanco M.
C, CantalapiedraRodríguez R., et al. uman corneal fibroblast migration and extracellular matrix synthesis during stromal repair:
Role played by platelet-derived growth factor-BB, basic fibroblast
growth factor, and transforming growth factor-1. Journal of Tissue
Engineering and Regenerative Medicine. 2018; 12(2): e737-e746.
- Bikfalvi A, Klein S, Pintucci G, Rifkin DB. Biological roles of fibroblast growth factor-2. Endocrine Reviews. 1997; 18(1): 26.
- Mestre L, Iñigo PM, Mecha M, Correa FG, Guaza C. Anandamide
inhibits Theiler’s virus induced VCAM-1 in brain endothelial cells
and reduces leukocyte transmigration in a model of blood brain
barrier by activation of CB1 receptors. Journal of Neuroinflammation. 2011; 8(1): 102.
- Shunsei, Hirohata, Hirotoshi, Kikuchi. Changes in Biomarkers Focused on Differences in Disease Course or Treatment in Patients
with Neuro-Behcet’s Disease. Internal Medicine. 2012; 51(24):
3359-65.
- Zenkel M, Lewczuk P, Jünemann A, Kruse FE, Naumann G,
Schl?Tzer-Schrehardt U. Proinflammatory cytokines are involved
in the initiation of the abnormal matrix process in pseudoexfoliation syndrome/glaucoma. American Journal of Pathology. 2010;
176(6): 2868–79.
- Campbell IL, Abraham CR, Masliah E, Kemper P, Inglis JD, Oldstone
MB, Mucke L. Neurologic disease induced in transgenic mice by cerebral overexpression of interleukin 6. Proceedings of the National
Academy of ences of the United States of America. 1993; 90(21):
10061-5.
- Maruo N, Morita I, Shirao M, Murota S. IL-6 increases endothelial
permeability in vitro. Endocrinology. 1992; 131(2): 710–4.
- Ghasemi H, Ghazanfari T, Yaraee R, Faghihzadeh S, Hassan ZM.
Roles of IL-8 in ocular inflammations: a review. Ocular Immunology & Inflammation. 2011; 19(6): 401–12.
- Curnow SJ, Falciani F, Durrani OM, Cheung C, Murray PI. Multiplex
Bead Immunoassay Analysis of Aqueous Humor Reveals Distinct
Cytokine Profiles In Uveitis. Investigative Ophthalmology & Visual
Science. 2005; 46(11): 4251–9.
- Li J, Ang M, Cheung C, Vania M, Chee SP. Aqueous Cytokine Changes Associated with Posner-Schlossman Syndrome with and without Human Cytomegalovirus. Plos One. 2012; 7(9): e44453.
- Singh H, Modabber M, Safran SG, Ahmed II. Laser iridotomy to
treat uveitis-glaucomahyphema syndrome secondary to reverse
pupillary block in sulcus-placed intraocular lenses: Case series.
Journal of cataract and refractive surgery. 2015; 41(10): 2215-23.
- Sousa DC, Leal I, Faria MY, Pinto LA. A Rare Manifestation of Uveitis-glaucoma-hyphema Syndrome. Journal of current glaucoma
practice. 2016; 10(2): 76–8.
- Zhang L, Hood CT, Vrabec JP, Cullen AL, Parrish EA, Moroi SE. Mechanisms for in-the-bag uveitis-glaucoma-hyphema syndrome. Journal of Cataract and Refractive Surgery. 2014; 40(3): 490–2.
- Wintle R, Austin M. Pigment dispersion with elevated intraocular
pressure after AcrySof intraocular lens implantation in the ciliary
sulcus. Journal of Cataract & Refractive Surgery. 2001; 27(4): 642–4.
- Piette S, Canlas O, Tran HV, Ishikawa H, Liebmann JM, Ritch R. Ultrasound biomicroscopy in uveitis-glaucoma- hyphema syndrome.
American Journal of Ophthalmology. 2002; 133(6): 839-41.
- Lima BR, Pichi F, Hayden BC, Lowder CY. Ultrasound Biomicroscopy
in Chronic Pseudophakic Ocular Inflammation Associated With
Misplaced Intraocular Lens Haptics. American Journal of Ophthalmology. 2014; 157(4): 813-817.e1.
- Wu N, Zhang H, Chen B, Ding W. A novel application of B-ultrasonography at various head positions in the diagnosis of untypical uveitis-glaucoma-hyphema (UGH) syndrome. Medicine (Baltimore). 2019; 98(2): e13891.