Introduction
The early diagnosis of lung cancer is becoming prevalent. Lung
segmentectomy has become a common surgical procedure in thoracic surgery, which is increasingly being used for the treatment
of early small-sized lung cancers [1-3]. However, anatomical segmentectomy is a much more complex procedure than lobectomy,
and it’s challenging and technique demanding, especially when
performed under total thoracoscopic visualization. The main
reason lies in the difficulty in dissecting the frequently variable
segmental structures (vein, artery, and bronchus) and identifying
the accurate intersegmental planes [4,5]. Furthermore, segmentectomy for S9 is one of the most challenging anatomical segmentectomy [6,7]. It is difficult to expose and correctly identify the
target vessels and bronchus because they are commonly variable
and deeply located in the lung parenchyma. Moreover, tailoring
the intersegmental plane is also challenging in video-assisted thoracoscopic surgery (VATS) S9 segmentectomy [8]. 3D reconstruction images have the advantage of providing a clear identification
of the pulmonary vessel branches even at the subsegmental and
more peripheral levels, thus making this complicated surgery easier and more practical [9,10].
Patients and methods
Patients
All surgeries were performed by the same thoracic surgeon
(Dr. Yun Liu) with assistant surgeons, who at least completed 200
cases of thoracoscopic anatomic lung resection per year. Between
February 2018 and December 2020, 17 patients who underwent
thoracoscopic S9 segmentectomy or S9b subsegmentectomy, all
procedures were performed using 3D interactive quantitative surgical planning through inferior pulmonary ligament approach. All
enrolled patients provided informed consent. The patients provided Informed Written Consent for the publication of their study
data. The patients’ preoperative characteristics and clinical outcomes were reviewed using a database of our institute. The study
was conducted in accordance with the Declaration of Helsinki (as
revised in 2013). The protocol of this study was approved by the
institutional review board of Yichang Central People’s Hospital
(NO. HEC-KYJJ-2018-601-01) (2018-01-09).
Selection criteria
The inclusion criterion for VATS segmentectomy in the present
study was computed tomography (CT) indicating a single lesion
around the lung (considered 1/3 outside the lung parenchyma)
with a diameter of ≤2 cm and with at least one of the following:
pathologically confirmed AIS, nodule with ≥50% ground-glass
opacity (GGO) on high-resolution CT, and imaging-confirmed tumor doubling time of ≥400 days. Patients who are not suitable
for lobectomy due to compromised cardiopulmonary function are
also appropriate candidates.
Preoperative planning
The preoperative workup of all patients included clinical history, physical examination, thin-slice CT of the chest, lung function
test, heart function test, blood gas analysis, and basic examinations as usual. Brain magnetic resonance imaging, bone scintigraphy, or positron emission tomography/CT was also performed if
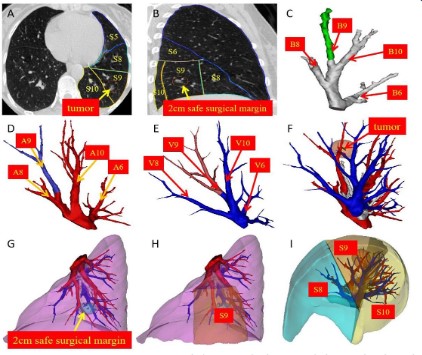
necessary. Prior to the operation, the lesion location and anatomy of the branches of the bronchus, arteries, and veins were identified using 3D reconstruction images. 3D reconstruction images
were generated for all patients using the Materialise 3-Matic software (developed by Materialise Nv Co., Materialise’s interactive
medical image control system, Kingdom of Belgium. Serial number: A51D56D6-C3XE-0011-1F7605D216DF39D5). The distance
from the lesion to the intersegmental plane was measured using
3D reconstruction images before the operation to ensure that
the lesion was at least 2 cm away from the resection margin, and
thus, the cut line was determined. The anatomic variations and
positional relations of the basal segmental vessels and bronchi
were analyzed. The location and radiological features of the target
nodule was identified. Furthermore, the anatomic relationship
between the nodule and the neighboring structures was collected
to design an appropriate surgical excision (Figure 1).
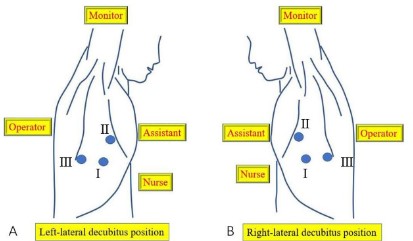
Positioning, anesthesia and port placement
The patient was placed in the contralateral lateral decubitus
position. General anesthesia was administered, and intubation
was achieved through a double-lumen endobronchial tube, surgery was performed with the lung collapsed on the operating side.
The surgeon stood at the dorsal side of the patient, and the assistant stood at the ventral side of the patient. The thoracoscope
port (approximately 1.5 cm long) was placed at the midaxillary
line of the 7th intercostal space. The main utility incision (approximately 3 cm long) was made in the 5th intercostal space at the
anterior axillary line, whereas the assistant incision was located
in the 8th intercostal space at the posterior axillary line (approximately 1.5 cm long). The incisions were protected with a silicone
rubber wound protector (Figure 2).
Surgical techniques
All procedures of segmentectomy were performed starting
with an inferior pulmonary ligament approach and proceeding in
a single-direction strategy without turnover of the lung repeatedly. The detailed procedures of RS9 and LS9 segmentectomy was
similar, we took a LS9 segmentectomy as example to depict the
detailed techniques in this study (Video 1).
Video 1: The detailed procedures of three-dimensional inter-
active quantitative surgical planning with complete thoracoscopic
left lateral basal segmentectomy.
B9, bronchus of the lateral basal segment; A9, artery of the
lateral basal segment; V9, vein of the lateral basal segment; S9,
lateral basal segment; S10, posterior basal segment; S8, anterior
basal segment; S6, superior segment.
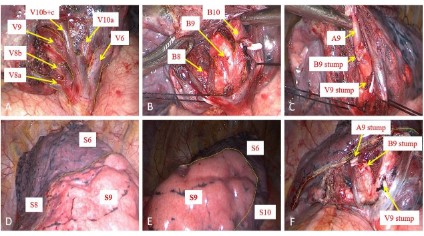
The dissection was initiated from the inferior pulmonary ligament. The inferior pulmonary vein was cleared from the surrounding tissues, and its basal branches were dissected [8]. After a careful dissection, the branches of the inferior pulmonary
vein to the target segment were skeletonized, this is the crux of
the ensuing dissection. For the segmental veins, we should follow the principles of preserving uncertain veins, particularly the
intersegmental veins. Corresponding to the 3D image, the name
of each vein branch was determined and the internal segment
vein V9a was divided. Sometimes, in order to ensure the safety
of the margin, the intersegmental vein (V9b) between S9 and S10
should also be separated. After the V9 was severed, we dissected
the lower lobe bronchus. The stem of the basal segmental bronchus was dissected. The bronchial branches were further dissected along the stems from proximal to distal [8]. B9 consists of B9a
and B9b, B9 itself is usually very short before bifurcation into B9a
and B9b, and the angle between these two subsegment bronchi is
often estimated to be close to 90 degrees, the stem and branches
of B9 were usually dissected from proximal to distal along the
stems. B9b was more comfortable to take since it was located in the shallow and more accessible hilar structures from this approach, B9a was less accessible as it location was much deep.
Therefore, it is sometimes difficult to isolate the B9 trunk. We
have to deal with B9a and B9b respectively, B9b was severed first
and B9a was severed later, the stem and branches of the common
basal segmental bronchus were usually dissected from proximal
to distal along the stems, at the same time peri-bronchial lymph
nodes were retrieved. Sometimes, if B9a was very close to B9b,
we just need to deal with B9, corresponding to the 3D image, the
B9 was confirmed and severed. After the bronchial branch was
severed, the target segmental feeding artery always came into
sight directly because it was always running along the bronchus.
The last step was managing the intersegmental plane and dividing the lung parenchyma. A modified inflation-deflation method
was used to identify the intersegmental plane [11]. After the targeted segment structures were dissected, the collapsed lung was
initiated to fully re-expand with controlled airway pressure under
20 cm H2O, followed by single lung ventilation. After an interval
of approximately 15 min, an irregularly curved demarcation was
identified naturally between the deflated preserving segments
and the inflated target segment. Furthermore, the contour of
the target segment was displayed. Thereafter, staple-based 3D
tailoring was performed. For the management of the intersegmental plane, we started from the relatively thin part of the lung
tissue and gradually reached the segmental gate and the thick
part of the lung. The specific steps were as follows: the first step
was opening the boundary between S8 and S9, the second step
was opening the boundary between S8 and S9 along the straight
line where the lower lung ligament is located, the third step was
opening the boundary between S9 and S10, and the last step was
opening the boundary between S6 and S9. The use of a stapler for
cutting the intersegmental plane does not affect the expansion of
the residual lung and does not cause atelectasis (Figure 3).
Pathological examination of the frozen section confirmed the
presence of a minimally invasive adenocarcinoma. The hilar and
mediastinal lymph nodes were obtained and sampled. The view
of the hilum following LS9 removal showed the stumps of the
targeted bronchi and vessels. The surgical margin width was >20
mm. Finally, the lung was dilated and air leakage was tested from
the stump of the bronchus and the resection margin of the lung.
An 8F thoracic catheter connected to a negative pressure drainage bottle was placed in the observation hole. The operative time
was 102 minutes, with an estimated blood loss of 35 ml. Early mobilization out of bed was started 12h postoperatively. The chest
tube was removed on postoperative day 3, the postoperative hospitalization time was 4 days, and the final pathology revealed the
presence of a pTmi1N0M0 minimally invasive adenocarcinoma.
At 3 months after the operation, the patient underwent chest CT
examination, revealing the presence of a well inflated lung (Figure 4).
The aforementioned techniques were used for most cases of
single or combined basal segmentectomy without considering
the interlobar fissure was complete or not. Margins were an important consideration for segmentectomy, the specimen must be
examined after resection, surgical margin was checked immediately. The surgical margin was sent for intraoperative frozen section pathological examinations, if the surgical margin was insufficient, an additional wedge resection would be performed. The
chest tube was removed if there was no air leak, well inflated lung
on chest X-ray, and less than 150 ml of drainage during the latest 24 hours. In cases with pulmonary adenocarcinoma, the new
proposed histologic classification system18 and the eighth edition
of TNM staging system 19 were adopted for histologic typing and
surgical-pathologic staging, respectively.
Statistical analysis
The data were analyzed using SPSS, version 22.0 (SPSS Inc.,
Chicago, IL, USA). Quantitative variables were expressed as median and range.
Results
Patients’ characteristics are shown in (Table 1). The study group
included 5 (29.4%) men and 12 (70.6%) women, ranging in age
from 26 to 71 years (median, 57 y). Among these, 2 cases were
active smokers. Regarding all patients, body mass index ranged
from 20.2 to 25.1 (median, 22.7) and lesion diameter ranged from
8 to 17 mm (median, 13.7 mm), with 7 (41.2%) lesions having
pure GGO, the consolidation ratio of 10 (58.8%) lesions was <50%,
surgical resection margin ranged from 20.0 to 27.7 mm (median, 21.7 mm). Eight patients underwent right segmentectomy (five
RS9 segmentectomy and three RS9b subsegmentectomy) while
nine patients underwent left segmentectomy (seven LS9 segmentectomy and two LS9b subsegmentectomy). 3D reconstruction
was successful in all patients, facilitating determination of the
operation plan according to simulation results; adequate resection margin distance was found for all patients. All procedures
were successfully performed under thoracoscopic visualization,
with no conversion to thoracotomy or lobectomy. In this group
of patients, pathological examination showed that curative resections were achieved with free surgical margins in all patients. All
patients had an R0 complete cancer resection on histology. The
histological subtypes of the segmental lesions included 7 of adenocarcinoma, 7 cases of MIA, 2 cases of AIS, and 1 case of AAH.
Among patients with AIS or MIA, systemic hilar and mediastinal
lymph node sampling was performed in 9 patients. Systemic hilar and mediastinal lymph node dissection were performed in 7
patients among those with adenocarcinoma. No patients were
identified with postoperative lymph node involvement. The pathological examination characteristics of the patients are shown in
Table 2. The median operation time of thoracoscopic left S9 (LS9)
segmentectomy was 122 min (range, 67-171 min), the median
operation time of thoracoscopic right S9 (RS9) segmentectomy
was 156 min (range, 75-217 min), the operation time of RS9 segmentectomy was significantly longer than that of LS9 segmentectomy (P<0.01). The median operation time of thoracoscopic S9b
subsegmentectomy was 101 min (range, 67-131 min), the median
operation time of thoracoscopic S9 segmentectomy was 167 min
(range, 79-217 min), the operation time of S9 segmentectomy
was significantly longer than that of S9b subsegmentectomy (P
<0.01). The median intraoperative blood loss was 50 ml (range,
35–230 ml). The median duration of chest tube insertion was 2
days (range, 1–4 days) and median length of postoperative hospital stay was 4 days (range, 3–7 days). No postoperative morbidity
was identified. No perioperative death was identified. No recurrence or mortality was observed during the median follow-up period of 13 months (range, 1–34 months). The operative results of
the patients are shown in (Table 2).
Table 1: Baseline characteristics of the patients
| Characteristic |
|
|
| Age, years |
Range |
26-71 |
|
Median |
57 |
| Male/female, n |
|
5/12 |
| Active smokers, n |
|
2 |
| BMI, kg/m2 |
Range |
20.2-25.1 |
|
Median |
22.7 |
| Image characteristics |
|
|
| Size, mm |
Range |
8-17 |
|
Median |
13.7 |
| Pure GGO, n |
|
7 |
| GGO with <50% solid part, n |
|
10 |
| Surgical resection margin, mm |
Range |
20.0-27.7 |
|
Median |
21.7 |
Table 2: Surgical types and perioperative outcomes.
| Variables |
n |
| Surgical types |
| Right |
8 |
| RS9 segmentectomy |
5 |
| RS9b subsegmentectomy |
3 |
| Left |
9 |
| LS9 segmentectomy |
7 |
| LS9b subsegmentectomy |
2 |
| Operative time, min RS9 segmentectomy |
| Range |
75-217 |
| Median |
156 |
| LS9 segmentectomy |
| Range |
67-171 |
| Median |
122 |
| S9 segmentectomy |
| Range |
79-217 |
| Median |
167 |
| S9b subsegmentectomy |
| Range |
67-131 |
| Median |
101 |
| Bleeding, ml |
| Range |
35-230 |
| Median |
50 |
| Chest tube duration, d |
| Range |
1-4 |
| Median |
2 |
| Postoperative hospital stay, d |
| Range |
3-7 |
| Median |
4 |
| Conversion to thoracotomy |
0 |
| Conversion to lobectomy |
0 |
| Postoperative complications |
0 |
| Histologic subtypes |
| Invasive AC |
7 |
| MIA |
7 |
| AIS |
2 |
| AAH |
1 |
| Pathological TNM stage of lung cancer (16 cases) |
| 0 |
2 |
| IA1 |
8 |
| IA2 |
6 |
| IA3 |
0 |
Ac: Adenocarcinoma; Mia: Minimally Invasive Adenocarcinoma; Ais: Adenocarcinoma In Situ; Aah: Atypical Adenomatous Hyperplasia. The operation time of left and right S9 segmentectomy was compared (P <0.01).
The operation time of S9 segmentectomy and S9b subsegmentectomy
was compared (P<0.01).
Discussion
The bronchovascular pattern of the basal segments is the most
complex [12]. The branching patterns of the left basal segmental
bronchus are B8 and B9+10 at a frequency of 80%; B8+9 and B10
at 4%; and B8, B9, and B10 at 16%. When S* is present (4% in
frequency), care should be taken when distinguishing A10 and A*
from B10a and B*. While the pulmonary artery usually branches
into A8 and A9+10 at a frequency of 74%; into A8+9 and A10 at a
frequency of 16%; and into A8, A9, and A10 at a frequency of 10%.
The branching patterns of the left basal vein are V8+9 and V9+10
at a frequency of 30%; V8+9+10 and V10 at 6%; V8 and V8+9+10
at 4%; V8+9 and V10 at 28%; V8 and V9+10 at 24%; and V8, V9,
and V10 at 8% [13]. The bronchovascular pattern of the right basal
segments (S7, S8, S9, and S10) was more complex, the branching
patterns of segmental bronchus are B8 and B9+10 at frequency
of 86%, B8+9 and B10 at 8%, and B8, B9, and B10 at 6%. While
the pulmonary artery usually branches into the A8 and A9+10 at
a frequency of 90%, into A8+9 and A10 at a frequency of 8%, and
into A8, A9, and A10 at a frequency of 2%. The branching patterns
of right basal vein are V8+9 and V9+10 at a frequency of 30%,
V8+9+10 and V10 at 14%, V8 and V8+9+10 at 2%, V8+9 and V10 at
26%, V8 and V9+10 at 18%, and V8, V9, and V10 at 10% [13]. Thoracoscopic segmentectomy for every basal segment is a technically challenging anatomical segmentectomy, with S9 segmentectomy being one of the most complex [9]. There are three methods
that can be used. First is the interlobar fissure approach using an
intersegmental tunneling to separate the superior segment (S6)
and basal segments, wherein we can first expose the segmental
hilum, thus exposing the pulmonary artery and bronchus branches and then resect the lateral part of the basal segment [14]. However, dividing the lung parenchyma and creating the tunnel were
technique-demanding procedures, especially when the interlobar fissures were not complete. There is also concern regarding
the possible torsion of S6 after complete separation from other
segments. Second is the inferior lung ligament approach used to
track the intersegmental plane following the inferior pulmonary
ligament, which is considered a landmark for intersegmental division. This approach is reasonable, however, such a unidirectional
dissection sometimes leads the surgeon to misunderstanding the
anatomy if the surgeon does not have sufficient experience. Zhu
and colleagues have reported a case of RS9 segmentectomy via
inferior lung ligament approach [15], this surgical method was
suitable for both left S9 segmental resection and right S9 segmental resection. To make the operation easier, we performed a 3D
reconstruction to identify the branches of the pulmonary vessels
of the patient [14,16]. Our results showed that the operation time
of RS9 segmentectomy was significantly longer than that of LS9
segmentectomy (P<0.01), which may be related to the difference
of bilateral anatomical structure, the bronchovascular pattern of
the right basal segments was more complex. S9 consists of S9a
and S9b. S9a is closer to the oblique fissure, while S9b is deeper.
According to our experience, some S9 extends to oblique fissure,
and some S9 does not extend to oblique fissure. B9b and A9b is
more comfortable to take since they are located in the shallow
and more accessible hilar structures from this approach. B9a and
A9a are less accessible as their location are much deep. So, the
operation time of S9 segmentectomy was significantly longer than
that of S9b subsegmentectomy (P<0.01). Third is the bidirectional
approach, which regards the pulmonary artery as the primary landmark [6]. If the fissure is incomplete or inflammatory, this
step can be tedious. Opening the fissure can lead to pulmonary
tears and troublesome oozing. We prefer the inferior lung ligament approach, with the aid of 3D reconstruction, it is possible
to accomplish all cases of S9 segmentectomy through an inferior
pulmonary ligament approach, which is the preferred approach in
our practice, without worrying about the fissures [8], the minimal
range of surgical resection can be determined by setting the safe
margin through three-dimensional reconstruction, and the operation mode (S9 segmentectomy or S9b subsegmentectomy) can
be determined before operation. Tracking the target segmental
branches by 3D reconstruction images during a single-direction
thoracoscopic S9 segmentectomy starting from the inferior pulmonary ligament. In this approach, dissection proceeds from the
pulmonary ligament to the hilum using the intersegmental septum as a landmark. We first encountered the inferior pulmonary
vein, which has the most variations and combinations. From this
point of view, the lack of a reference and insufficient surgical experience and anatomical knowledge may lead to miscalculation
in identifying the vein branches. The accurate establishment of
the target vein is challenging and should be overcome in S9 resection through the inferior lung ligament approach. In this situation,
we have to expose pulmonary vein from proximal to distal side as
possible by cutting lung parenchyma along intersegmental plane.
Here we suggest that three-dimensional reconstruction should be
introduced into the operation, given that it is a good tool to confirm the target segment vein and the intersegmental vein. Similarly, 3D reconstruction can help in tracking the target bronchi and
reducing unnecessary exploration. We do not need to expose all
the branches of the artery because it does not affect the accurate identification of the target artery. The artery generally corresponds to the bronchus one by one and slightly deviates from the
spine. Of course, we can confirm A9 through 3D reconstruction.
Tailoring the intersegmental plane is another challenge encountered in VATS S9 segmentectomy. The anatomical characteristics of this segment make it difficult to imagine how multiple
staplers tailor the segment. It starts from a relatively thin part of
the lung tissue and gradually reaches the segmental hilum and
the thick part of the lung, from the periphery to the center with
“step-by-step” stapling [18]. The guidance of 3D reconstructed
images not only enables to achieve a safe surgical margin but also
minimizes the anatomic resection of lung tissues [19].
Conclusions
The optimal surgical techniques and approach of thoracoscopic S9 segmentectomy remains the subject of debate, based on 3D
interactive quantitative surgical planning, thoracoscopic S9 segmentectomy can be successfully performed using an inferior pulmonary ligament approach. 3D reconstruction is helpful for the
surgeon to decide which segment should be resected and to know
the anatomic features of the target segmental structures and its
neighbors. We believe that even an inexperienced surgeon using
3D reconstruction can perform thoracoscopic S9 segmentectomy
with acceptable safety and complications.
Limitations
This study is a retrospective one without comparisons of techniques. However, because the experience with thoracoscopic S9
segmentectomy is still lacking worldwide, we believe that it is still of importance to provide an additional option for thoracic surgeons to consider. The follow-up period of patients with lung can-
cer was short and long-term outcomes were expected.
Declarations
Author contributions: Conception, study design and protocol:
Y Liu, SL Zhang, CB Liu. Identification of studies: Y Liu, SL Zhang.
Data analysis and interpretation: Y Liu; Manuscript writing: Y Liu.
Project oversight and supervision: SL Zhang, CB Liu. Critical revisions for important intellectual content: All authors. All authors
read and approved the final manuscript.
Funding: This work was supported by the Medical and Health
Research Program (A20-2-015), Science & Technology Bureau of
Yichang.
Conflict of interest: None declared.
References
- Handa Y, Tsutani Y, Mimae T, Miyata Y, Okada M. Complex segmentectomy in the treatment of stage IA non-small-cell lung cancer.
Eur J Cardiothorac Surg 2020; 57: 114-21.
- Wisnivesky JP, Henschke CI, Swanson S, Yankelevitz DF, Zulueta
J, Marcus S. Limited resection for the treatment of patients with
stage IA lung cancer. Ann Surg 2010; 251:550-4.
- Shapiro M, Weiser TS, Wisnivesky JP, Chin C, Arustamyan M, Swanson SJ et al. Thoracoscopic segmentectomy compares favorably
with thoracoscopic lobectomy for patients with small stage I lung
cancer J Thorac Cardiovasc Surg. 2009; 137: 1388-93.
- Yan TD. Surgical atlas of thoracoscopic lobectomy and segmentectomy. Annals of Cardiothoracic Surgery 2014; 3: 183-91
- Liu C, Liao H, Guo C, Pu Q, Mei J, Liu L. Single-direction thoracoscopic basal segmentectomy. J Thorac Cardiovasc Surg 2020; 160:
1586-94.
- Sato M, Murayama T, Nakajima J. Thoracoscopic stapler-based
‘‘bidirectional’’ segmentectomy for posterior basal segment (S10)
and its variants. J Thorac Dis 2018; 10: 1179-86.
- Endoh M, Oizumi H, Kato H, Suzuki J, Watarai H, Masaoka T et al.
Posterior approach to thoracoscopic pulmonary segmentectomy
of the dorsal basal segment: a single-institute retrospective review. J ThoracCardiovasc Surg 2017; 154: 1432-9.
- Pu Q, Liu C, Guo C, Mei J, Liu L. Stem-Branch: a novel method for
tracking the anatomy during thoracoscopic S9-10 segmentectomy.
Ann Thorac Surg 2019; 108: 333-5.
- Oizumi H, Endoh M, Takeda SI, Suzuki J, Fukaya K, Sadahiro M et
al. Anatomical lung segmentectomy simulated by computed tomographic angiography. Ann Thorac Surg 2010; 90: 1382-3.
- Nakamoto K, Omori K, Nezu K. Superselective segmentectomy for
deep and small pulmonary nodule under the guidance of three-dimensional reconstructed computed tomographic angiography
Ann Thorac Surg. 2010; 89: 877-84.
- Wang J, Xu X, Wen W, Wu W, Zhu Q, Chen L et al. Modified method
for distinguishing the intersegmental border for lung segmentectomy. J Thorac Cancer 2018; 9: 330-3.
- Nagashima T, Shimizu K, Ohtaki Y, Obayashi K, Nakazawa S, Mogi A
et al. Analysis of variation in bronchovascular pattern of the right
middle and lower lobes of the lung using three-dimensional CT angiography and bronchography. Gen Thorac Cardiovasc Surg 2017;
65: 343-9
- Nomori H, Okada M. Illustrated anatomical segmentectomy for
lung cancer. Heidelberg: Springer Science & Business Media; 2012.
- Igai H, Kamiyoshihara M, Kawatani N, Ibe T. Thoracoscopic lateral
and posterior basal (S9 + 10) segmentectomy using intersegmental
tunnelling. Eur J Cardiothorac Surg 2017; 51: 790-1.
- Zhu Y, Pu Q, Liu L. Trans-inferior-pulmonary-ligament single direction thoracoscopic RS9 segmentectomy: application of stem-branch method for tracking anatomy. Ann Surg Oncol 2020; 27:
3092-3.
- Kikkawa T, Kanzaki M, Isaka T, Onuki T. Complete thoracoscopic S9
or S10 segmentectomy through a pulmonary ligament approach. J
Thorac Cardiovasc Surg 2015; 149: 937-9.
- Oizumi H, Kanauchi N, Kato H, Tndoh M, Suzuki J, Fukaya K et al.
Anatomic thoracoscopic pulmonary segmentectomy under 3-dimensional multidetector computed tomography simulation: a report of 52 consecutive cases. J Thorac Cardiovasc Surg 2011; 141:
678-82./li>
- Zhu Y, Pu Q, Liu L. Trans-inferior pulmonary-ligament VATS basal
segmentectomy: application of single-direction strategy in segmentectomy of left S9+10. J Thorac Dis 2018; 10: 6266-8.
- Wu WB, Xu XF, Wen W, Xu J, Zhu Q, Pan XL et al. Three-dimensional computed tomography bronchography and angiography in
the preoperative evaluation of thoracoscopic segmentectomy and
subsegmentectomy. J Thorac Dis 2016; 8: 710-5.