Case description
A 35-year-old male patient was admitted to the Department
of otorhinolaryngology of our hospital on August 1, 2022 due to
“bilateral nasal congestion with headache for more than 6 years”.
Patients with no obvious incentives in bilateral nasal congestion
six years ago, I have a side of the heavier, lay down at night and
a change in the weather congestion is aggravating, usually have
a sneeze, the symptom such as flow cleaning stuff, no flow pus,
hyposmia, no facial pressure and swelling of the nasal cavity, out-patient doctor after checking with the nasal septum deviation,
bubble on the right side one” She was admitted to the hospital, in
good health, with no history of meningitis and no special family
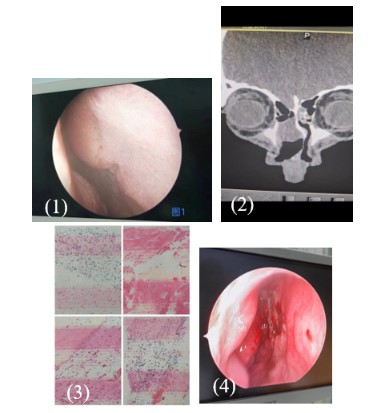
history. Hospital physical examination: nasal appearance is good,
see: under nasal endoscope (Figure 1) double nasal mucosa is
ruddy, nasal septum front-end clearly to the left deviation, block
the left nostril, before the left nasal cavity structure is not seen,
on the right side of the nasal visible light pink neoplasm growth,
qualitative soft, smooth surface without damage, middle turbinate partial properties, and the mass roots part on the septum.
CT of paranasal sinus in our hospital on June 29, 2022 (Figure 2)
showed: 1. Soft tissue shadow in ethmoid sinus cavity, obvious left
deviation of nasal septum, inflammation 2. Chronic inflammation
of the right maxillary sinus and ethmoid sinus. After the relevant
examinations were completed before surgery, the patient underwent the operation of “septum correction, right septum mass
extraction + right maxillary sinus and ethmoid sinus opening”
under general anesthesia on August 3, 2022. During the operation, the tumor was found to be closely connected with the right
lateral mucosa of the nasal septum, without adhesion to the right
middle and inferior turbinates, and the base of the tumor was derived from the right lateral mucosa of the nasal septum. The basal
area was about 1.5 cm x 1.0 cm in size, and the tissue was slightly
tough and not easy to bleed. A small amount of clear fluid was
found to flow out of some of the tumor tissues after biting lead,
and no obvious bleeding was observed. After the tumor specimen was collected for examination, the nasal septum mass was
completely removed with the power cutting system. It was found
that the inner surface of the tumor had cystic membrane, and the
boundary between the tumor and the nasal septum mucosa was clear. The nasal cavity was filled with absorbable naxi sponge after
operation. Postoperative pathology showed ectopic brain tissue
(glial ectopic) and inflammatory polyps (Figure 3). Symptomatic
supportive treatment such as anti-inflammation and hemostatic
treatment was given after the operation. The patient improved
and was discharged from hospital one week after the operation.
Reexamination one week after the operation showed satisfactory
correction of the nasal septum, a small amount of dry scab attached to the right nasal septum operation area, and nasal cavity
was cleaned, and the nasal septum mucosa was intact, and the
tumor did not relapse (Figure 4). The patient felt nasal congestion
disappeared, still slightly felt forehead pain, a small amount of
clear liquid flowed out when the right nasal cavity bowed its head,
after the operation, the headache disappeared, nasal cavity still
flowed clear nose, and other complaints of special discomfort.
Discussion
Heterotopia of nasal neuroglia-nGH, also known as nasal glioma, is a rare congenital midline benign tumor. A disease in which
nerve tissue grows outside the central nervous system and ectopic glial tissue is deposited extracranial during embryonic development due to abnormal closure of the nasal and frontal bones
[1]. This disease was first reported by Reid in 1852, and the concept of glial ectopia was elaborated by Schmidt in 1900. Since it
occurs most often in the nose, this disease is called nasal NGH [2].
Nasal glial ectopia is often diagnosed in neonates but rarely found
in adults. There is no family history of the disease, the incidence is
very low, the male to female ratio is about 3:2, and it is usually not
accompanied by other congenital malformations [3].
NGH is not a true tumor, but a congenital malformation. Its etiology and pathogenesis are still unclear. At present, the accepted
pathogenesis is "meningoencephalocele" theory [4]. At 8 weeks
of embryo, there is an anterior nasal space between the nasal and
frontal bones and their deep square nasal cartilage sac. Through
this, the dura meets the skin of the outer nose, forming a dural
diverticulum. With the development of the frontal osteonasal
process, the dural diverticulum gradually separated from the outer nasal skin and retracted into the skull, the blind foramen was
filled with fibrous tissue, and the dura was completely enclosed
in the skull. At the same time, the nasal cartilage sac gradually
developed into the nasal septum cartilage, the vertical plate of
ethmoid bone and the comb, until the nasal space disappeared.
During the retraction of the dural diverticulum into the skull, congenital nasal NGH is formed its part of the neural tissue remains
in its retraction path.
Glial heterotopia (NGH) can occur in several sites, including
the scalp, orbit, nasal cavity, middle ear and mastoid process, soft
palate, tongue base and neck, and other sites. The incidence of
ectopic sites ranges from 1 in 20,000 to 1 in 40,000. However, it
mainly occurs around the nasal root, leading to ectopic nasal glial
cells [2]. NGH can be divided into three types according to the site
of occurrence, namely, intranasal type (about 30%), nasal appearance type (about 60%) and mixed type (about 10%) [3-5]. Extrasal
nasal glial Ectopia IS MOSTLY FOUND AT BIRTH, AND as the child
grows, the tumor gradually increases in size, resulting in a widening of the nasal root and a widening of the pupil spacing. This
results in facial deformities and frequent tears, but when crying,
the tumor does not grow or harden; Intranasal tumors are usually
located near or connected to the nasal septum by connective tissue. The clinical manifestations were dyspnea, nasal congestion,
runny nose, mouth opening breathing, snoring, choking during
feeding, and feeding difficulties. The diagnosis of intranasal type
is generally later than that of extranasal type [2]. This case is an
adult patient, who had no related symptoms in childhood after
questioning the history. This time, he sought medical treatment
because of nasal obstruction and headache, which was caused by
nasal obstruction considering ectopic nasal stenosis caused by nasal neuroglia and nasal septum deviation blocking nostrils.
The symptoms and laboratory findings of nasal NGH in adults
are nonspecific. The diagnosis mainly depends on preoperative
computed tomography (CT) and MRI imaging. CT helps to observe
the bone defect of the anterior skull base, while MRI provides
supplementary information about the fluid or soft tissue characteristics of the mass. MRI also provides a three-dimensional view
and can determine intracranial invasion [9]; Some authors proposed MRI as the first choice for ectopic glioma after summarizing
the cases in the past 40 years. If bone defect was considered, CT
control was performed [6].
Macroscopic, intranasal HNG is nodular or polypoid, without
capsule, smooth surface, medium hardness, gray powder or grayish brown, cut surface grayish white grayish red, cystic cavity may
form, cystic containing cerebrospinal fluid like clear fluid; The outer nasal type has skin on the surface, and the inner nasal type is
covered with nasal mucosa [2], which does not radiate or expand
with the Valsalva maneuver or crying. The ipsilateral internal jugular vein should be compressed, and the Furstenberg test should be
negative to observe whether the mass is dilated or pulsatile [6,7].
Histologically, nasal NGH consists of an unencapsulated collection of astrocytes, eosinophilic glial cells in the connective tissue
matrix, and the internal neural tissue is nonfunctional, as no surgical excision resulting in any neurological deficits has been reported. The possible intracranial connections are usually fibrous and
do not disrupt the dura [8,9]. According to the study of 10 cases
of nasal NGH in foreign countries, it was found that all cases were composed of neurons and glia in different proportions. There was
no obvious ependyma, choroid plexus or light membrane, and the
complex epithelium (skin, respiratory or metaplastic squamous
epithelium) was intact, although sometimes weakened and atrophic. The glial component is often difficult to identify, especially
when there are associated inflammatory complexes, or fibrosis is
evident. All cases had chronic inflammatory cells, including lymphocytes and macrophages, and reactive gliosis. In adult patients,
fibrosis or sclerosis is significantly more severe and almost completely masks the background glial tissue [8], making it difficult for
pathologists to diagnosis nasal NGH.
A strict and comprehensive differential diagnosis of nasal mass
must be performed before treatment. The external nasal lesions
should be differentiated from common nasal root masses such
as hemangioma, dermoid cyst, meningoencephalocele, etc. [8]:
hemangioma is soft and multiple. some skin temperature increases, and the pressure can be reduced. Dermoid cysts showed cystic
structures by CT and MRI examination. In addition to the imaging
features of meningoencephalocele, the mass is usually translucent and can beat with pulse or breathing. The mass can increase
with crying force, and the tension can increase. Furstenber sign is
positive. Intranasal NGH should be distinguished from nasal polyps and meningocele. Intranasal NGH is easy to be misdiagnosed
as nasal polyps, the latter is soft, often accompanied by asthma,
nasal itching, nasal congestion, runny nose and other symptoms
of sinusitis, patients often have a history of allergic rhinitis, the
former contrary; Meningocele is the herniation of brain and/or
meningeal tissue through a bone defect in the skull. The herniated tissue remains connected to the intracranial nervous system
and subarachnoid space, and the meninges or brain tissue usually
enters the upper nasal passage through the lamina cribriae. Or
they may enter the sinuses and nasopharynx through bone defects in the sphenoid or ethmoid sinuses. In addition, pathological examination of nasal meningoencephalocele usually indicates
that the lesion is composed of brain and meningeal tissue, with
neuronal cells and ependyma, elements rarely observed in nasal
glial ectopia; Although meningocele and nasal glial ectopia have
similar clinical manifestations and pathologies, they require different treatment approaches. Therefore, meningocele must be
ruled out by clinical and radiographic examination to prevent CSF
leakage and meningitis before any form of surgical intervention
is performed in patients with suspected congenital nasal glia heterotopia. In such cases, CT and MRI of the nasal cavity are usually
performed to determine whether the nasal lesion shows intracranial communication. Although the distinction between nasal NGH
and encephalocele depends on the presence of a connection between the mass and the intracranial tissue. However, studies have
shown that even with CT and MRI, this connection may be very
small or insignificant. In addition, given the developmental abnormalities, bone defects may also be associated with nasal NGH but
still show no connection to the brain parenchyma, distinguished
by the presence or absence of meningitis and/or CSF rhinorrhea
before and after surgery.
For the patients, patients with adult due to congestion in hospital, preoperative examination from the septum pure sense,
vesicular sense, nasal polyps, etc to consider is one-sided, most
doctors in adult patients, the consultation will not NGH and meningeal encephalocele as the primary differential diagnosis of nasal
septum neoplasm, then if blind lines of preoperative biopsy or surgical removal of the endoscopic surgery. This may lead to serious consequences such as meningitis, brain abscess, or cerebrospinal fluid rhinorrhea [9], so it also reminds us physicians that
when nasal mass is encountered, comprehensive preoperative
evaluation must be performed, and preoperative biopsy or surgery should not be performed blindly.
Conclusion
Nasal glial heterotopia is a rare benign congenital disease. In
our case, ectopic presentation of glial tissue over the nasal septum was extremely rare. Evaluation should include preoperative
imaging with thin-cut coronal and axial CT scans and multiplanar
MRI scans to rule out any intracranial connections before invasive surgery. In the case of nasal NGH, endoscopic resection is
required. Postoperative recurrence and malignant potential are
rare. These patients may develop cerebrospinal fluid rhinorrhea
and infection after surgery, so close follow-up is important.
References
- Iacob D, Fufezan O, Popa-Stănilă R, Topoe M. Frontonasal gliomadiagnostic difficulties. Med Pharm Rep. 2021; 94(1): S33-S35.
- Yy Yan, Zy Zhou, J Bi, Y Fu. Nasal glial heterotopia in children: Two
case reports and literature review. International Journal of Pediatric Otorhinolaryngology.
- Ling Nana, Wu Jingjing, Duan Shihong. Nasal glial endometriosis in
1 [J]. Chinese otolaryngology head and neck surgery. 2022; 29(5):
337338.
- Yang Xiaojian, Tang Lixing, Wang Pengpeng, Zhang Nan, Sun Jihang, Zhang Wei, Ge Wentong Yang Xiaojian, Tang Lixing, Wang
Pengpeng, Zhang Nan, Sun Jihang, Zhang Wei, Ge Wentong ectopia of nasal glia in children: a clinical analysis of 13 cases. Chinese
Journal of Otorhinolaryngology Head and Neck Surgery 2021; 56.
- Patterson K, Kapur S, Chandra RS. “Nasal gliomas” and related
brain heterotopias: a pathologist′s perspective[J]. Pediatr Pathol.
1986; 5(3-4): 353-362.
- Jiang Chenyan, Lin Nana, Peng Lijing, Shi Runjie. Congenital intranasal meningoencephalocele complicated with ectopic glioma: a
case report and literature review [J]. Chin j otorhinolaryngology
skull base surgery,2018; 24(04): 336-340.
- A MAJITHIA, S H LIYANAGE, R HEWITT, W E GRANT.Adult nasal
glioma presenting with visual loss[J].The Journal of Laryngology &
Otology, 2010; 124: 1309–1313.
- Carla R. Penner, DDS, and Lester D.R. Thompson, MD .Nasal Glial
Heterotopia: A Clinicopathologic and Immunophenotypic Analysis
of 10 Cases With a Review of the Literature[J].Annals of Diagnostic
Pathology, 2003; 7(6): 354-359.
- Wei WZ, Wang XL, Huang SY. Evaluation of CT and MI in diaagnosis
of intranasal encephalomeningocele. J Journal of Clinical Otorhinolaryngology. 2004; 18: 84-85.
- Bykova VP, Bakhtin AA, Polyakov DP, Yunusov AS, Daikhes NA.
Kliniko-morfologicheskaia kharakteristika nazal’noĭ glial’noĭ geterotopii [Nasal glial heterotopia: Clinical and morphological characteristics]. Arkh Patol. 2017; 79(5): 38-42.