Introduction
Most pediatric ophthalmic tumors are benign. However, they
may have a significant impact on vision and may result in significant morbidity and mortality [1,2]. The wide varieties of rare intraocular and orbital neoplasms differ in presentation in the pediatric population in comparison to same entities in adults [1,2].
Rhabdomyosarcoma is a rare childhood cancer but the most
common primary orbital malignancy occurring in this age group
with estimated incidence of 4.5 cases per million with 50% occurring in the first decade of life [1-3]. Generally, rhabdomyosarcoma
is classified into four major subtypes; including embryonal, alveolar, botryoid and pleomorphic (57%, 19%, 6% and 1% respectively)
[2]. The most common presenting clinical features were unilateral proptosis (30%), eyelid edema (21%), and blepharoptosis
[2,3]. Other manifestations are Nasal congestion and epistaxis [2].
Orbital apex syndrome, manifested by complete ophthalmoplegia, ptosis, decreased corneal sensation, and vision loss, was reported by Machleder et al. as a result of RMO [4,5].
Rhabdomyosarcoma of the orbit (RMO) is managed through
a multidisciplinary approach including surgery, chemotherapy
and irradiation [6]. Little evidence is available regarding details of
the management and the choice of intervention in RMO [7]. Current treatment guidelines use a staging system by the Intergroup
Rhabdomyosarcoma Study Group dividing the patients into four
stages and four groups to allocate each to a certain combination
of treatment modalities [7].
Stages are categorized based on universal TNM staging [8]. In
short, Groups are divided into: localized disease and completely
resected is considered group I, microscopic remnants after biopsy
as group II, gross residual disease detected after biopsy as group
III while presence of distant metastasis onset as group IV [7].
In Saudi Arabia, only one large scale study was conducted targeting pediatric patient regarding orbital lesions [9]. Alkatan et al
reported only 11 cases of RMO in the largest specialized tertiary
ophthalmology center in Saudi Arabia over a period extending
from 2000 to 2013 [9]. Here, we report a case of RMO, outlining the clinical presentation, histopathological features and treatment outcomes.
Case report
Clinical presentation: 8-year-old girl who is medically free,
presented with diffuse swelling of the right eye for one month
followed by sudden dystopia, pain and proptosis in the same eye
two days prior to emergency department visit. There was no history of trauma and significant family history of similar condition.
Upon initial assessment of the right eye, visual acuity was severely
impaired 20/100, Intraocular pressure was 25 mmhg with dystopic globe inferiorly and palpable mass, restricted supraduction.
Disc swelling was also noted. The left eye was normal on examination (Figure 1).
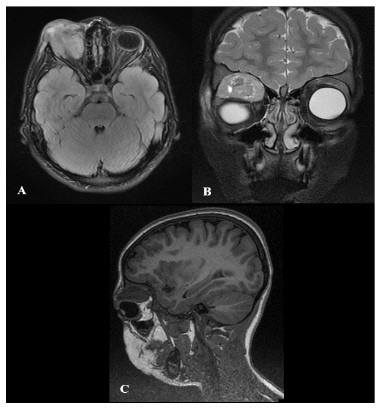
Radiological imaging: Computed Tomography (CT) brain
showed Hyper-enhancing heterogeneous mass in the right superior extraconal compartment, loss of interface with superior rectus and a small superior orbital wall erosion. Contrasted Magnetic
resonance Image (MRI) brain showed an extraconal mass with
heterogeneous enhancement and faint diffusion restriction, invasive of right orbicularis oculi muscle and no intracranial extension
(Figure 2A-C).
Surgical intervention: The patient was planned for gross total
resection but due to the high vascularity and loss of clear surgical plan, small biopsy was obtained and sent to histopathology.
Unfortunately, pathology came inconclusive. The patient was
planned for excisional biopsy through pterion-orbital craniotomy
in which tumor was resected as one piece successfully (Figure 3).
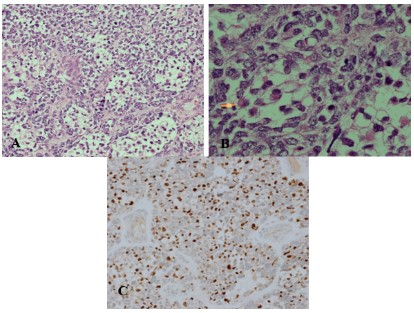
Histopathological features: The excisional biopsy suggested
Rhabdomyosarcoma, most probably alveolar type (Figure 4A,B).
The tumor cells were positive for desmin and myogenin immunostains (Figure 4C). The Myo-D1 stain is non-contributory. CD99,
SMA, Chromogranin and Cytokeratin cocktail staining are negative.
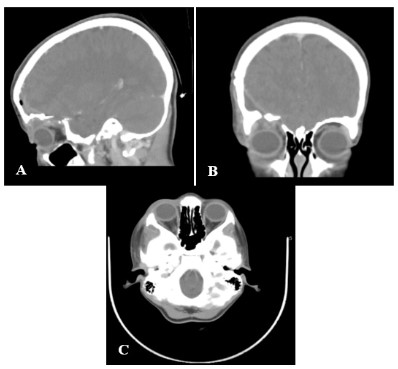
Outcome and follow-up: contrasted CT brain post-operatively
showed no enhancing tissue to suggest residual tumor (Figure
5A-C). On the basis of the histopathological-confirmed diagnosis
of RMO, a complete workup was done by oncology team which
all came negative. The patient was assigned as stage I grade II
rhabdomyosarcoma. Patient was started on chemotherapy protocol ARST0531 on week 1 and radiotherapy protocol ARST0531
on week 4. During the 8th week of chemotherapy, ophthalmology
examination showed: right eye eyelid ptosis, redness, tenderness, blepharitis, eyelid skin abrasion in the medial and lateral canthus,
conjunctiva showed mild follicular reaction and the lens showed
early post subcapsular cataract. The rest of the examination was
normal. Initial management included antibiotics, antiviral and
heavy lubrication. Later-on, patient developed more radiotherapy-related ophthalmic complications like blepharoconjunctivitis,
pre-septal cellulitis, cataract and exposure keratopathy and had
multiple ophthalmology surgeries and progressive rapid visual
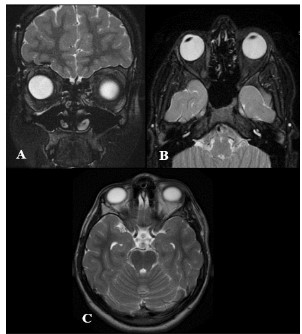
acuity deterioration over the course of five years. Four years post-surgery follow up brain MRI showed stable postsurgical changes
in the right orbit with no signs of tumor recurrence (Figure 6A-C).
In the last follow up, five years after the surgery, she was only able
to count fingers 4ft in the right eye.
Table 1: Summary of the reported cases of orbital rhabdomyosarcoma in the literature.
| Author |
Study type |
Year |
Age |
Gender |
presentation |
Histology |
Grade |
Intervention |
Outcome |
| Machleder et al [4] |
Case report |
2004 |
12y |
female |
progressive visual
loss + difficulty in eye
movements + mild
headache |
alveolar |
IV |
radiation therapy + systemic chemotherapy |
complete return of extra-ocular movement, visual
acuity remained impaired
with persistence of a left afferent defect. |
| Yazici et al [15] |
Case report |
2014 |
15y |
Male |
progressive painful
proptosis+ loss of vision |
embryonal |
NA |
radiation therapy + chemotherapy |
orbital symptoms were
improved and visual acuity
increased to 20/20 |
| Elomrani et al [16] |
Case report |
2014 |
20y |
Male |
NA |
embryonal |
NA |
chemotherapy |
local recurrence and cutaneous Metastasis |
| Sarkar et al [17] |
Case report |
2012 |
18y |
male |
pain in the right hip +
inability to fully extend
the joint, followed by
proptosis of the right
eye + blurred vision +
photophobia |
alveolar |
IV |
chemotherapy + radiation therapy |
patient died 3 weeks after
initiation of treatment |
| Amato et al [18] |
Case report |
2002 |
29y |
male |
nasal obstruction +
epistaxis + headache +
subacute visual loss in
the left eye |
Inconclusive
biopsy |
NA |
Chemotherapy + radiation therapy |
The patient died 2 years
after the initial diagnosis of
disseminated disease. |
| Kaliaperumal et al [19] |
Case series |
2007 |
10y |
female |
proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy |
No recurrence in 3 years |
| Kaliaperumal et al [19] |
Case series |
2007 |
4y |
male |
Proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy + surgery |
No recurrence in 2 years |
| Kaliaperumal et al [19] |
Case series |
2007 |
29y |
Female |
Proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy + surgery |
Loss of follow up |
| Kaliaperumal et al [19] |
Case series |
2007 |
10y |
female |
Proptosis |
embryonal |
NA |
Chemotherapy |
No recurrence in 1 year |
| Kaliaperumal et al [19] |
Case series |
2007 |
9y |
Female |
Proptosis |
alveolar |
NA |
Chemotherapy + radiotherapy + surgery |
No recurrence in 2 years |
| Kaliaperumal et al [19] |
Case series |
2007 |
7y |
male |
Proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy |
No recurrence in years |
| Wang et al [20] |
Case report |
2019 |
6 m |
Female |
congenital skin lesion
involving the left glabella and orbit |
embryonal |
NA |
proton therapy +
chemotherapy |
No recurrence in 1 year |
| Dziedzic et al [21] |
Case report |
2015 |
4y |
Female |
swelling + proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy + surgery after recurrence |
local recurrence treated
by Endonasal endoscopic
surgery with gross-total
resection |
| Rustemeyer et al [22] |
Case report |
2011 |
7y |
male |
Proptosis |
embryonal |
NA |
Chemotherapy + radiotherapy + surgery
after recurrence |
local recurrence 3 times
after the third time no recurrence |
| Li et al [23] |
Case report |
2018 |
6y |
Female |
Proptosis |
embryonal |
III |
Chemotherapy +
radiotherapy + excisional biopsy |
regression of the residual
orbital mass |
| Kim et al [24] |
Case report |
2019 |
6y |
Female |
Mild injection + eyelid
swelling |
NA |
NA |
Chemotherapy + radiotherapy |
NA |
| Chitsike et al [25] |
Case report |
2012 |
4m |
Female |
Swelling + proptosis |
embryonal |
NA |
Chemotherapy |
Didn’t respond to chemotherapy and offered palliative care |
| Othmane et al [26] |
Case report |
1999 |
34y |
male |
Painless mass of the
eyelid |
embryonal |
NA |
Chemotherapy +
radiotherapy + exci-
sional biopsy |
No recurrence |
| Van den bogaert et
al [27] |
Case report |
1992 |
6y |
male |
Mass |
embryonal |
NA |
Chemotherapy +
radiotherapy |
Multiple local recurrence
then intracranial extension |
| Maurya et al [28] |
Case report |
1990 |
4y |
male |
Painless proptosis |
embryonal |
NA |
Surgery + radiotherapy |
NA |
| Sanz-marco et al [29] |
Case report |
2014 |
25y |
Female |
headache and discomfort in the right eye |
alveolar |
III |
Chemotherapy +
radiotherapy |
remission and resolution of
the proptosis and ophthalmoplegia |
NA: Not Available. Chemotherapy: deferent regimens used. Radiotherapy: deferent regimens used. Y: years. M: months.
Discussion
Radiologically, rhabdomyosarcoma could show different features based on the type and location [10]. On CT, these lesions
tend to show moderate to highly enhanced homogenously well
circumscribed masses [11]. Calcification could be also seen in case
of bony destruction which is another common feature of these
lesions [11]. In the present case, CT showed hyper-enhancing heterogeneous mass in the right superior extraconal compartment
having loss of interface with superior rectus and a small superior
orbital wall erosion. Such lesions appear isointense to muscles on
T1 and hyperintense to muscles on T2 on Magnetic Resonance
Images (MRI) [11]. Post-contrast, these lesions usually exhibit
moderate to substantial enhancement [11]. MRI findings in the
present case were similar to the previous description.
Histopathological-confirmation of the diagnosis and staging of
orbital RMS, which was done by evaluating imaging (MRI of primary tumor, chest-CT and bone scan), and subsequent workup for
metastases, are used to make therapy decisions [6,7,12].
Management strategies include surgery, radiotherapy and chemotherapy [6,7,12]. Patients allocated to stage 1 group II, like in
the presented case, can receive different choices of treatment
based on which protocol is being followed [12]. North American
Intergroup Rhabdomyosarcoma Study Group (IRSG) suggest treatment with a combination of chemotherapy (vincristine and actinomycin and cyclophosphamide; VAC) and radiotherapy (36 Gy)
for group II patients [12]. The European pediatric Soft tissue sarcoma Study Group (EpSSG) protocol (EpSSG-RMS-2005) propose
chemotherapy VA and in the first four courses Ifosfamide is added; if complete remission is achieved after three chemotherapy
courses radiotherapy (36 Gy) is added which can be replaced with
addition of more ifosfamide [12] if remission is not achieved following chemotherapy radiotherapy (45 Gy) is added without further ifosfamide [12].
Long term ophthalmic sequalae after chemotherapy and radiotherapy could be devastating [1,13]. The most common complication is cataract [1,13]. Other complications including keratopathy,
ptosis, lacrimal duct stenosis, keratoconjunctivitis and retinopathy could also be seen [1,13]. In the present case, patient developed multiple complication secondary to radiotherapy including:
blepharoconjunctivitis, conjunctival abrasion, cataract, severe
dryness, inflammation, and decrease in the visual acuity.
In this type of lesions, the long-term visual acuity outcome is
a crucial aspect to consider [1]. Eade et al, reported in their study
which included 18 cases that 29% of the patients attained vison
better than 6/12 and 43% had vision worse than 6/60 [1]. In the
present case, the visual acuity declined over the course of four
years as result of multiple complications after the radiotherapy
until she is only able to count fingers 4ft. Patient survival is related to a number of factors but the most important of which is
whether the main tumor is T3 or above according to the AJCC TNM staging system for Orbital Sarcoma [14].
Conclusion
RMO is the most common pediatric orbital tumor. Treatment
modalities includes: surgery, chemotherapy and radiation therapy. Radiation-related ophthalmic sequalae is devastating and it is
important to have regular ophthalmic follow-up. With excellent
survival in patients with RMO, the continued efforts are encouraged to reduce the post treatment morbidity by reducing the intensity of treatment or adopting newer treatment techniques.
Declarations
Conflict of interest: The authors declare that the article content was composed in the absence of any commercial or financial
relationship that could be constructed as a potential conflict of
interest.
Funding sources: None
Acknowledgment: None.
References
- Eade E, Tumuluri K, Do H, Rowe N, Smith J. Visual outcomes and
late complications in paediatric orbital rhabdomyosarcoma: Late
outcomes of orbital rhabdomyosarcoma. Clin Experiment Ophthalmol. 2017; 45(2): 168–73
- Indelicato DJ, Rotondo RL, Mailhot Vega RB, Uezono H, Bradfield S,
Agarwal V, et al. 45 GyRBE for group III orbital embryonal rhabdomyosarcoma. Acta Oncol. 2019 Oct 3;58(10):1404–9.
- Ermoian RP, Breneman J, Walterhouse DO, Chi Y-Y, Meza J, Anderson J, et al. 45 Gy is not sufficient radiotherapy dose for Group III
orbital embryonal rhabdomyosarcoma after less than complete response to 12 weeks of ARST0331 chemotherapy: A report from the
Soft Tissue Sarcoma Committee of the Children’s Oncology Group.
Pediatr Blood Cancer. 2017; 64(9): e26540.
- Machleder DJ, Banik R, Rosenberg RB, Parikh SR. An unusual case
of rhabdomyosarcoma presenting as orbital apex syndrome. Int J
Pediatr Otorhinolaryngol. 2005; 69(2): 249–54
- Badakere A, Patil- Chhablani P. Orbital Apex Syndrome: A Review.
Eye Brain. 2019; 11: 63–72.
- Blank LECM, Koedooder K, van der Grient HNB, Wolffs NAW, van
de Kar M, Merks JHM, et al. Brachytherapy as Part of the Multidisciplinary Treatment of Childhood Rhabdomyosarcomas of the
Orbit. Int J Radiat Oncol. 2010; 77(5): 1463–9.
- Shields JA, Shields CL. Rhabdomyosarcoma. Surv Ophthalmol.
2003;48(1): 39–57.
- James D. Brierley, Mary K. Gospodarowicz, Christian Wittekind.
TNM Classification of Malignant Tumours. 8th ed. 2017; 241.
- Alkatan HM, Al Marek F, Elkhamary S. Demographics of Pediatric
Orbital Lesions: A Tertiary Eye Center Experience in Saudi Arabia. J Epidemiol Glob Health. 2019; 9(1): 3.
- Inarejos Clemente EJ, Navallas M, Barber Martínez de la Torre I,
Suñol M, Munuera del Cerro J, Torner F, et al. MRI of Rhabdomyosarcoma and Other Soft-Tissue Sarcomas in Children. RadioGraphics. 2020; 40(3): 791–814.
- Rao AA, Naheedy JH, Chen JY-Y, Robbins SL, Ramkumar HL. A Clinical Update and Radiologic Review of Pediatric Orbital and Ocular
Tumors. J Oncol. 2013; 2013: 1–22.
- Jurdy L, Merks JHM, Pieters BR, Mourits MP, Kloos RJHM, Strackee
SD, et al. Orbital rhabdomyosarcomas: A review. Saudi J Ophthalmol. 2013; 27(3): 167–75.
- Boutroux H, Levy C, Mosseri V, Desjardins L, Plancher C, Helfre S, et
al. Long-term evaluation of orbital rhabdomyosarcoma in children:
Orbital rhabdomyosarcoma in children. Clin Experiment Ophthalmol. 2015; 43(1): 12–9.
- Sa H-S, Rubin ML, Ning J, Li W, Tetzlaff MT, McGovern SL, et al. Association of T and N Categories of the American Joint Commission
on Cancer, 8th Edition, With Metastasis and Survival in Patients
With Orbital Sarcoma. JAMA Ophthalmol. 2020; 138(4): 374.
- Yazıcı B, Sabur H, Yazıcı Z. Orbital cavitary rhabdomyosarcoma:
case report and literature review. Ophthalmic Plast Reconstr Surg.
2014; 30(1): e20-2.
- Elomrani F, Touri S, Ouziane I, Berrada N, Boutayeb S, Mrabti H,
Elkhannoussi B, Errihani H. Orbital rhabdomyosarcoma with skin
metastasis: a case report. BMC Res Notes. 2014; 7: 670.
- Sarkar D, Ray S, Saha M, Chakrabarti P. Alveolar rhabdomyosarcoma with multiple distal metastases. A case report and review of
literature. BMJ Case Rep. 2012 Sep 3;2012:bcr2012006523. doi:
10.1136/bcr-2012-006523. Erratum in: BMJ Case Rep. 2012; 2012.
- Amato MM, Esmaeli B, Shore JW. Orbital rhabdomyosarcoma metastatic to the contralateral orbit: a case report. Ophthalmology.
2002; 109(4): 753-6.
- Kaliaperumal S, Tiroumal S, Rao V. Orbital rhabdomyosarcoma: a
case series. Indian J Cancer. 2007; 44(3): 104-7.
- Wang S, Li P, Li J, Liu J, Jiang X, Zeng W. A case of congenital rhabdomyosarcoma. Pediatr Dermatol. 2019; 36(5): 747-749.
- Dziedzic TA, Anand VK, Schwartz TH. Endoscopic endonasal approach to the lateral orbital apex: case report. J Neurosurg Pediatr.
2015; 16(3): 305-8.
- Rustemeyer J, Günther L, Junker K. Limits and chances in an unfortunate course of recurrent orbital rhabdomyosarcoma. Nepal J
Ophthalmol. 2011c; 3(2): 202-5.
- Li A, Blandford A, Chundury RV, Traboulsi EI, Anderson P, Murphy E,
Parikh S, Perry J. Orbital rhabdomyosarcoma in a child with Leigh
syndrome. J AAPOS. 2018; 22(2): 150-152.e1
- Kim J, Ussher JG. Orbital rhabdomyosarcoma: a rare ophthalmic
condition. Med J Aust. 2019; 211(9): 398-399.e1.
- Chitsike I, Masanganise R, Sibanda D, Kuona P. Rhabdomyosarcoma of the orbit in a four months old infant in Zimbabwe: A case
report. Cent Afr J Med. 2012; 58(5-6): 26-9.
- Othmane IS, Shields CL, Shields JA, Eagle RC Jr, Gunduz K, Fitch S.
Primary orbital rhabdomyosarcoma in an adult. Orbit. 1999; 18(3):
183-189.
- Van den Bogaert W, Van Limbergen E, Dralands G, Drochmans A.
Curative irradiation of the entire orbit in rhabdomyosarcoma: a
case report. Head Neck. 1992; 14(5): 392-4.
- Maurya OP, Patel R, Thakur V, Singh R, Kumar M. Embryonal rhabdomyosarcoma of orbit--a case report. Indian J Ophthalmol. 1990;
38(4): 202-4.
- Sanz-Marco E, España E, Alamar A, Pérez-Rojas J, López-Prats MJ,
Díaz-Llopis M. Rabdomiosarcoma alveolar orbitario enmascarado
por sinusitis etmoidal en un adulto de 25 años [Orbital alveolar
rhabdomyosarcoma masked by ethmoid sinusitis in a 25-year-old].
Arch Soc Esp Oftalmol. 2014; 89(5): 182-5