Introduction
In the last 10 years, the merge of technology and healthcare
has seen tremendous growth. From automatic craniotomy systems that prevent penetration of dura mater or elegant tissue
of the brain, to robotic systems that help with pedicle screw
placements and augmented reality that guides surgeons in safe
tumor resections. All these advancements have significantly improved patient safety outcomes and more reliable approaches to
the narrow neurosurgical corridors. Upon reviewing the current
literature about technological advancements in surgical fields,
many of them mention trials and successes in the developing or developed world. There are only a few published materials that
widely discuss the application of these technologies in low and
middle-income settings. We hypothesized that authors of many
technologically advanced papers are simply overlooking the potential applicability and availability of these medical technologies
there. However, the feasibility of the novel surgical technologies,
especially in the LMIC (low and middle-income countries) regions
might be a total success in achievement, since these geographical
regions usually don’t have the strict restrictions that many developed countries impose.
Distance and feasibility
One of the successes of the application of advanced technology in LMIC settings was demonstrated by Tejas M Patel, Sanjay
C Shah, and Samir B Pancholy In the paper “Long Distance TeleRobotic-Assisted Percutaneous Coronary Intervention: A Report
of First-in Human Experience” published on September 3, 2019
- Dr. Patel and his colleagues demonstrated tremendous success
in treating cardiac patients remotely. While interventional cardiology and neurosurgery are different fields, endovascular access
to many procedures is relevantly similar. Many neuroendovascular and cardio endovascular procedures access major vessels
via femoral or radial arteries, therefore, allowing a comparison
to neurosurgery directly. This exact scenario of remote neuroendovascular work might be the actual answer to bridging the gap
between specialists in remote areas.
Availability and price
In another study, published by Sheth et al “Assessment of Brain
Injury Using Portable, Low-Field Magnetic Resonance Imaging at
the Bedside of Critically Ill Patients” we saw how portable MRI
could be accessed on-demand in critical neuro patients. What
piqued our interest in researching more about this machine is its
uniqueness in mobility, price sensitivity, and accessibility of results
on demand. These 3 elements are extremely important in underserved and rural areas of LMIC regions. One of the most devastating outcomes of the neurosurgery of LMIC is the unavailability of
the right technology and specialists themselves. While our focus
is not on the lack of specialists, but rather on technological feasibility and price points, it must be noted that the lack of specialist
care is a huge burden and must be further investigated as well.
When we thoroughly assessed the paper by Sheth et al. it was
clear how the portability of Hyperfine’s MRI machine in 50 patients was a tremendous success in neurological Intensive Care
Units (ICU) at Yale-New Haven Hospital in New Haven. The feasibility of rolling in the machine right at the bedside of a patient’s
head - is an ideal scenario for many underserved regions, as many
hospitals are sometimes lacking a good interior foundation in the
developing world.
Another very important concept of this modern technology
is the price point of under $100,000 and the rapid availability of
scanned results. This on-demand infrastructure of the hyperfine
machine allows underserved and rural regions to get the right information on time, and potentially save a life of a critical neurosurgical patient.
Savings and the latest computer technology
While reviewing modern medical technologies, we couldn’t
mention augmented and virtual reality. Healthcare as a field essentially wants to be as organized and as safe as the aviation industry. The aviation industry implements numerous safety checks
before deploying any protocols or scenarios, including the case-based Augmented Reality (AR) flight practice for pilots. Finally,
the medical field started widely adopting the same scenarios for
medical student education and surgical treatments. Neurosurgery
particularly has been implementing numerous AR-based scenarios for resident-physician education, pre-and intra-operative
scenarios, and more. Currently, the same Augmented Reality is
utilized in modern operating rooms to visualize arteriovenous malformations (AVMs), tumors, and even the safe placement of
pedicle screws in the spine. In the publication by Mascitelli J et
al “Navigation-Linked Heads-Up Display in Intracranial Surgery:
Early Experience,” it described how heads-up display was utilized
in 79 patients with 84 combined pathologies. The paper showcased how this technology helped neurosurgeons treat a very
wide range of cranial pathologies safely during multiple stages
of operation. This principle of safety and efficacy plus affordability might be the answer to many costly devices associated with
neurosurgical operating rooms. While operating in tight surgical corridors such as the skull or spine, a neurosurgeon needs to
know the position where he or she operates in. Therefore, neuro-navigation constantly must be utilized in order not to damage the
critical parts of the brain tissue. For the sake of this paper, it was
very essential for us to find a solution that might be affordable
and feasible in resource-limited settings. The augmented reality
technology might be used exactly in this case, as was discussed
in our previous published paper titled “Current and future use of
virtual and augmented reality in neurosurgery: a literature review
by Zhalmukhamedov, E., Urakov, T.M.
The adoption of technology and an open mind to try new
things in surgical settings remains the challenge in many LMIC and
developed countries. Therefore, we have a unique opportunity
right now to showcase how these new technologies could majorly
improve patient care and save money in resource-limited settings.
Methods
In this publication, we performed review research on highly effective neurosurgical technologies that have drastically improved
neurosurgeons’ experience in the operating room. The literature
on the most significant technological advancements in neurosurgery and its application in low and-middle-income countries are
reviewed and discussed. The applicability of technology ranged
from the years of 2009 to 2022. Our findings showcased the average price spent on traditional imaging and interventional technology and compared it to the cost of acquiring the latest/new
technological advancements. The availability and calculation of
pricing were based on widely available price tags in scientific publications or original equipment manufacturers (OEM). The novelty
of chosen technologies was based on scientific search queries
from PubMed, Neurosurgical Meetings, and its proven applicability in the hospital settings of the developed world. Additionally,
we surveyed 2 active neurosurgeons in the United States, who are
pioneering the fields of spine augmented reality and advanced
technology in endovascular neurosurgery.
To quantify the quality of this paper we narrowed down our
search to the years 2009-2022. The criteria for inclusion of researched papers were based on novelty, applicability, feasibility,
and active usage in surgical fields. The literature search conducted
in March 2022 yielded in total of 303 results for “augmented reality in neurosurgery” and 448 results for “modern technology in
neurosurgery”. The sum of (n=751) search queries was screened.
Out of these results, we narrowed down 70 papers that fit our
criteria.
Since the socioeconomic status of the geographical region is
also one of the central themes of this paper - a cost comparison
was included as well. We collectively identified 30 available price
tags from scientific papers and widely available prices on the World Wide Web. Although our research focused on neurosurgery, a cross-disciplinary application of technology from medical
specializations such as neurology, radiology, and surgery was included in this paper.
The era of robots and computer-powered technology
The days when neurosurgeons had to go to the dark radiology
room to see the film scans of CT or MRI have been long gone from
our lives in the developed world. Now many operating rooms are
equipped with digital screens and the latest navigation systems to
guide surgeons in the right region of the brain or spine. Not only
does neurosurgery as a field embrace the technology, but it also
pushed the boundary to improve operating techniques and patient outcomes. Many computer-related technological advancements have directly impacted the field of medicine at large. One
of the most exciting things that many neurosurgeons embraced is
virtual and augmented reality [1]. This haptic technology allows
neurosurgeons to visualize patient-specific anatomy for preoperative and intraoperative care. One of the major adoptions in
augmented reality is taking place in the skull base, followed by
the spine and endovascular neurosurgery. In all three areas - a
heads-up display is utilized to visualize the anatomy, pathological structures, and areas to avoid intraoperatively. The traditional
microscope and navigation use - create an attention distractor for
the surgeon while operating in the tight corridors of the surgical
exposure. However, the use of a heads-up display mounted on
the head or glasses of the surgeon - allows distractions flow of
surgery and is less prone to errors [2]. This technology was a tremendous help and improvement in the workflow of the operator,
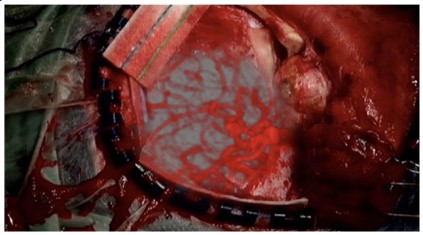
from planning a skin incision, craniotomy, tissue differentiation, etc. More than 84 cranial-based pathologies such as aneurysms,
Arteriovenous Malformations (AVMs), meningiomas, osteoblastoma, Cerebrospinal Fluid (CSF) leaks, and more are accurately
addressed with the help of this technology (figure 1) [2-4]. The
application and benefits of spine surgery could be observed in figure 2, where T. Urakov MD from the University of Miami utilizes
augmented reality for pedicle screw placements.
When it comes to robotics, spine and endovascular fields have
shown massive progress, especially in the United States and Europe, among which the Mazor and Rosa family robots were prevalent the most in spine cases [4]. Even though according to the
survey of neurosurgeons practicing in the global regions, it was
stated as a positive surgical outcome for the patients, the cost of
acquiring and maintaining this technology has proven significantly
high [5].
In an example of the spine, endovascular and cerebrovascular
fields - a remote video robot, robotic-assisted angiography, guided microscopes, clipping, and coil insertion devices have been
pioneered in this arena [6]. The successful treatments of saccular
sidewall aneurysms of the basilar artery and carotid artery angioplasty were successfully treated by utilizing CorPath GRX Vascular
Robotic System in Toronto and Philadelphia University hospitals
[7,8]. Another significant breakthrough in the endovascular and
cerebrovascular field was telemedicine application, especially in
the areas where stroke unit teams are scarce or non-existent. The
significant time management in TPA administration of Cerebrovascular Accident (CVA) patients and door-to needle times for endovascular procedures were significantly reduced - thanks to Tele-
stroke systems. The current tele-stroke application improved the
treatment rate from 19% to 78% in Southeast Bavaria, Germany
[9]. These are so far the most successfully diverse cases reported
in neurosurgery around the world.
While technology greatly contributed to the advancement of
neurosurgical care intraoperatively; perioperative care technologies remain the golden standard for identifying pathological lesions in the central or peripheral nervous systems. Particularly CT
and MRI machines are still one of the oldest and most reliable
methods to identify pathology promptly. While these machines
remain bulk and financially significant for the hospitals, there
were some advancements in this area. In 2020 one of the pioneers of portable MRI machines was born, Hyperfine Research
inc. received full clearance for the usage of the first fully functional portable MRI. This machine has significant advantages for
patient care and financial incentives [10]. The machine provides
significant mobility within the patient’s location due to its size and
it costs around $50,000 in comparison to the traditional high-field
MRI machine which costs from $1 to USD 3 million.
The next significant step in a potential application in neurosurgery is Metaverse. According to a broad definition, a Metaverse is
a 3D virtual reality world powered by real users’ input and interaction. Generally speaking, it’s a virtual world where people can socialize and actively participate in various activities, including work,
education, play, and general participation for leisure time [11]. Dr.
Koo from Seoul National University, Bonding Hospital, Korea - performed one of the first educational lung cancer surgery through
Metaverse. Essentially, this operating room had significant investments to become “smart” also known as a technologically savvy operating room. The operating room was equipped with 360-8K-
3D cameras and XR immersive sound system for seamless surround sound. All participants had an option either to have a 3D
headset (figure 3) for a more immersive experience or simply a
computer screen to attend this surgery LIVE. As a main theme of
Metaverse, each participant was asked to create an avatar or gamified persona to enter the metaverse hall where the surgery was
broadcasted. With the help of 3D cameras and smart technologies
in the operating room, each participant was able to observe surgery virtually from any corner. This exact application of Metaverse
has significant advantages over in-person surgery attendance.
Many academic surgeons who actively teach medical students,
residents, and fellows – understand that overcrowding and low
visibility of the operating field is a huge issues for in-training doctors. As neurosurgery requires a delicate technique in executing
various procedures, observation of an operating physician’s hand
movements is critical for proper education. Additionally, some
ergonomics of an operating room could be observed as well, it
helps physicians-in-training understand the role of each person
in the operating room and how they strategically move around
[12]. This exact technology might have a significant improvement
in operating techniques for surgeons who work in remote locations or lack knowledge in advanced neurosurgical procedures.
Another positive outcome of utilizing Metaverse’s virtual reality
is COVID-19 precautions in crowded places. Metaverse could be
deployed anywhere in the world, which allows participants to
be in their comfort zone and eliminate the social distancing concerns while observing surgery LIVE. In addition to the metaverse,
there are some exciting developments in haptic technology, such
as Meta’s haptic feedback glove that allows participants to feel
the object, which is essential for any surgeon’s experience [13].
However, haptic technology remains in the developmental phase
of Metaverse or Augmented/Virtual Reality for surgery and the
public at large.
Current challenges of low-and middle income countries
Critical imaging
While modern technology continues to improve, some traditional modalities of obtaining critical neuroimaging are still lacking
in LMICs. One of the main resource limitations in LMIC is Computed
Tomography (CT) and Magnetic Resonance Imaging (MRI). These
two critical machines that help identify critical intracranial pathologies such as bleeding or hematomas in emergency settings, significantly reduce morbidity and mortality in the mentioned above
geographical areas. A survey conducted from 2015 to 2016 in Sub-Saharan Africa revealed a sum of 84 MRI machines for a popula-
tion of 372, 551, 411 people [14]. These statistics are very disappointing, knowing the high significance of motor vehicle-related
accidents due to poor road Infrastructure in the LMICs [15,16].
Lack of specialists in the field
Many rural and resource-limited geographical locations of
healthcare systems usually lack many specialized surgeons. This
lack of specialist surgeons is especially felt in the neurological surgery arena [17]. There are significant barriers such as lack of training in the reachable area for physicians to specialize, inadequately
trained operative personnel, and lack of equipment.
Additionally, it’s worth noting that neurosurgery is considered
one of the most expensive specialties to train in. The average cost
to train a fully competent neurosurgeon in the United States is
approximately $341,978.00 plus $27,876.36 for annual expenses
[18]. This amount is truly astronomical for the developing and
LMIC regions, as spending per physician education in Colombia
for example, costs $80,971.80 for a privately held university and
$54,971.79 for a public educational institution [19].
One can see the huge gap in spending on physician education,
therefore many LMIC doctors are unfortunately at a big disadvantage for specialized education [20]. While neurosurgery is considered one of the technically and academically challenging specialties, not many countries can afford nor have the luxury to train
one. One of these LMICs are Caribbean islands, in St. Lucia for
example, there are only 2 neurosurgeons who take care of a population of 180,287 people [21]. This proportion seems extremely
unreasonable and impossible at the same time, to address urgent
neurosurgical procedures that can save a life. It’s worth noticing,
that both neurosurgeons on this island have received their neurosurgical education overseas to help locals address their neurosurgical challenges.
Even though neurosurgery is one of the most expensive specialties out there, one of the scientific studies proved to have an
economic benefit to the country. Hubbard et al. calculated Disability Adjusted Life Years (DALY) per neurosurgical intervention
in Haiti. The total benefit to the country’s economy due to neurosurgical interventions was from $2.5 to $5.5 million [22]. These
significant numbers, upon proper presentation, could pave the
way for the funding of neurosurgical care and education in LMICs.
The potential technology that could be applied to LMICs
Earlier in this paper, we discussed some of the latest technological advancements in neurosurgery and how they benefit patients. While many of these technologies will require a substantial
investment, some options could be affordable for many LMICs.
In table 1 we present an example of a comparison between traditional cost versus investment in the latest imaging technology.
The average cost of traditional technologies was calculated based
on the popularity of the products within hospital systems in the
developed world. Malham et al. provided an excellent overview
of major pricing points, which guided us in calculating the average
price point in table 1 [23]. The prices provided in table 1 have been
closely approximated, as fluctuations of the exact prices could be
changed by manufacturers or distributors daily. We calculated the
difference between traditional technology and modern technology and captured total savings.
The following price range models were identified:
1. Fluoroscopy imaging: $250,000 - $500,000
2. Intraoperative CT: $600,000 – $1.2 million
3. Neuronavigation system: $250,000 - $700,000
4. MRI Scanners: $200,000 - $3 million
5. AR Navigation System (P.e HoloLens 2) + a set of 4 digital
cameras: $7,000 - $10,000
The cost of a portable Hyperfine MRI unit and complete AR
System with needed cameras for augmentation & 3D imaging -
was based on the original equipment manufacturer’s (OEM) price
and a widely available price tag on the internet.
Table 1: Imaging technology cost comparison for traditional vs. new technology.
| Total Savings |
MRI Machine |
Neuronavigtion |
| Average Traditional Cost |
Hyperfine Portable MRI Cost |
AR Navigation System Cost |
Traditional Neuronavigation Cost |
| ≈ $1 million |
≈ $50,000 |
≈ $10,000 |
≈ $483,000 |
| $950,000 |
$473,000 |
Another critical point of price sensitivity is associated with
maintaining the actual equipment. The cost of maintenance of
traditional MRI and Neuronavigation is very significant and should
be considered thoroughly. The average cost of repairing a traditional imaging system is between 4 to 14 percent of the actual
acquisition cost [24]; additionally, there should be personnel that
is adequately trained in repairing these machines. All these costs
should be adequately calculated and/or negotiated before the
final acquisition. The newer systems on another hand might be
more complex in terms of technological hardware, however, the
maintenance cost is significantly lower in comparison to traditional systems.
While considering a wide range of neurosurgical procedures
for this research, we narrowed it down to only essential neurosurgical procedures that are critical for a patient’s survival and quality of life. Therefore, for the quality of this paper, we are considering critical care/trauma neurosurgery, spine, and endovascular
neurosurgery. Upon reviewing multiple published papers, these
exact fields of neurosurgery are tended to be frequent in terms
of the scope of LMIC cases [25]. However, the largest contributor
to neurological diseases in terms of DALY is found to be a cerebrovascular accident (CVA). If we look at Nigeria as an example
of a developing world, the highest mean direct cost of stroke was
$8424 USD [26], while the highest average annual salary in the
country was $1243.56. Even though Nigeria as a country participates in Universal Healthcare Coverage (UNC) the difference of
$7180.44 per single stroke accident is a significant amount for the
country and patients alike. Additionally, the quality of treatment
is not always guaranteed, as the scarcity of neurosurgeons in Nigeria is massive 97 neurosurgeons for a population of 200 million
[27]. This statistic doesn’t even include super-specialized training
in the field.
Therefore, we propose an investment in telerobotic and robotic endovascular robots, that could be operated either remotely or
in the hospitals themselves. While endovascular robots are still
in the pre-approval stages, it has already shown some great potential to change stroke treatment forever, especially in remote
areas.
The first-ever long-distance remote endovascular procedure
was successfully implemented in India. The group of intervention
cardiologists successfully deployed CorPath GRX®, (Corindus Vascular Robotics, USA) at a 32 km distance between operating medical centers. What was essential for this procedure is the availabil-
ity of a catheterization staff and unit, an obvious technology of
the CorPath robot, and reliable connectivity infrastructure [28].
Even though this Indian success has proven a breakthrough success, there are still more investigations and trials that need to be
deployed to prove the efficacy worldwide. The success of Patel
et.al has proven, that rural medicine might finally bridge the gap
of specialist doctor shortages in rural areas.
However, telerobotic interventions, on the other hand, are
already actively utilized in remote areas of the developed world
and have proven a better outcome in those regions [29]. These
robots will help local non-specialized neurosurgeons receive guidance from physicians who are specifically trained in this area in
the developing or developed world. The average cost to implement a telestroke unit in a hospital is $46,000 [30]. Even though,
this seems like a large investment especially for LMIC regions, the
long-term benefit outweighs the burden of investment, as we
showcased in an example of Nigeria’s DALY. As everyone knows
that time is of the essence, especially in the stroke scenario, therefore, it’s important to provide a needed or guided intervention on
time. The therapeutic window for the application of thrombolytic
therapy or immediate lifesaving neurosurgical intervention could
be drastically decreased, once a telestroke unit is operational.
While investing in this telerobot might be a big one-time cost, the
total burden of CVA outcomes in LMIC might be easier financially
on the government. For the reference of the reader, we provided a visual cost representation of the cerebrovascular robot and
telerobot in table 2.
Table 2: Representation of prices for robotic technology in vascular neurology/neurosurgery.
| Average cost of Telerobot |
Average cost of CorPath GRX Robot |
| ≈ $46,000 |
≈ $650,000 [31] |
Results
In this paper, we demonstrated how the latest technological advancements in neurosurgery could play a vital role in the
improvement of patient care in LMICs. Our findings have shown
how the latest imaging technology of portable MRI, AR Neuronavigation, Telerobot, and Endovascular Robots have a tremendous
advancement in improving care and could save money for local
government and healthcare systems. The comparison of acquiring new technology versus the cost of traditional treatment has shown favorable towards technology. An investment in modern
technology will allow any LMIC region to become more progressive in its approach to healthcare needs, especially in times of the
COVID-19 pandemic.
The significant cost reduction of DALYs spending due to the
implementation of technology, will further improve not only
the population’s health but also economic output, and bring up
healthier nations.
Conclusion
The advantages of modern technology in the neurosurgical
specialty play a vital role in patient survival. Technology that has
proven a positive outcome for neurosurgical patients, must be seriously considered for implementation in LMIC hospital systems.
The only logical setback of the mentioned technologies - is the
financial upfront cost to the facility or government. However, the
evidence provided on the financial benefits of long-term outcomes might be a win-win situation for providers and policymakers alike. This literature review research should provide a foundational groundwork for an open dialogue within LMIC regions
to adapt the novel technological advancements in neurosurgery.
Further investigation and feasibility of the proposed technology
must be carried out to solidify a purchase decision per country of
origin and their needs.
Acknowledgments
I would like to thank my academic mentors Timur Urakov MD-Associate professor of neurosurgery at the University of Miami,
Jabbour Pascal MD - Professor, Neurological Surgery, The Angela
and Richard T. Clark, Distinguished Professor and Division Chief,
Neurovascular Surgery & Endovascular Neurosurgery, and Parham Yashar MD-President of Yashar Neurosurgery.
References
- Pelargos P, Nagasawa D, Lagman C, Tenn S, Demos J, et al. Utilizing virtual and augmented reality for educational and clinical enhancements in neurosurgery. Journal of Clinical Neuroscience.
2017; 35:1-4.
- Mascitelli J, Schlachter L, Chartrain A, Oemke H, Gilligan J, et al.
Navigation-Linked Heads-Up Display in Intracranial Surgery: Early
Experience. Operative Neurosurgery. 2017; 15: 184-193.
- Zhalmukhamedov E, Urakov TM. Current and future use of virtual
and augmented reality in neurosurgery: a literature review. Indonesian Journal of Neurosurgery. 2019; 2: 50-54.
- Drouin S, Kochanowska A, Kersten-Oertel M, Gerard I, Zelmann
R, et alIBIS: an OR ready open-source platform for image-guided
neurosurgery. International Journal of Computer Assisted Radiology and Surgery. 2016; 12: 363-378.
- Stumpo V, Staartjes V, Klukowska A, Golahmadi A, Gadjradj P, et al.
Global adoption of robotic technology into neurosurgical practice
and research.Neurosurgical Review. 2020; 44: 2675-2687.
- Menaker S, Shah S, Snelling B, Sur S, Starke R, et al. Current ap-
plications and future perspectives of robotics in cerebrovascular
and endovascular neurosurgery. Journal of NeuroInterventional
Surgery. 2017; 10: 78-82.
- Mendes Pereira V, Cancelliere N, Nicholson P, Radovanovic I, Drake
K, et al. First-in-human, robotic-assisted neuroendovascular intervention. Journal of NeuroInterventional Surgery. 2020; 12: 338-
340.
- Sajja K, Sweid A, Al Saiegh F, Chalouhi N, Avery M, et al. Endovascular robotic: feasibility and proof of principle for diagnostic cerebral
angiography and carotid artery stenting. Journal of Neuro Interventional Surgery. 2020; 12: 345-349.
- Müller-Barna P, Hubert G, Boy S, Bogdahn U, Wiedmann S, Heuschmann P et al. TeleStroke Units Serving as a Model of Care in
Rural Areas. Stroke. 2014; 45: 2739-2744.
- Sheth K, Mazurek M, Yuen M, Cahn B, Shah J, Ward A et al.: Assessment of Brain Injury Using Portable, Low-Field Magnetic Resonance Imaging at the Bedside of Critically Ill Patients. JAMA Neurology. 2021; 78: 41.
- Kye B, Han N, Kim E, Park Y, Jo S. Educational applications of metaverse: possibilities and limitations. Journal of Educational Evaluation for Health Professions. 2021; 18: 32.
- Koo H. Training of lung cancer surgery through metaverse including extended reality in the smart surgical room in Seoul National
University Bundang Hospital, Korea. Journal of Educational Evaluation for Health Professions. 2021; 18: 33.
- “Inside Reality Labs Research: Meet the Team That’s Working to
Bring Touch to the Digital World.” Facebook Technology, 2021.
- Ogbole G, Adeyomoye A, Badu-Peprah A, Mensah Y, Nzeh D. Survey of magnetic resonance imaging availability in West Africa. Pan
African Medical Journal. 2018; 30.
- De Silva M, Roberts I, Perel P, Edwards P, Kenward M, et al. Patient
outcome after traumatic brain injury in high-, middle- and low-income countries: analysis of data on 8927 patients in 46 countries. International Journal of Epidemiology. 2008; 38: 452-458.
- Zhalmukhamedov E, Magloire C, Maidyrov E, Soans A, Elijio L, et al.
Overview of neurosurgical capacity in St. Lucia. Romanian Neurosurgery. 2019; 329-331.
- Punchak M, Mukhopadhyay S, Sachdev S, Hung Y, Peeters S, et al.
Neurosurgical Care: Availability and Access in Low-Income and
Middle-Income Countries. World Neurosurgery. 2018; 112: e240-e254.
- Gasco J, Holbrook T, Patel A, Smith A, Paulson D, Muns A et al. Neurosurgery Simulation in Residency Training. Neurosurgery. 2013; 73: S39-S45.
- Gil-Rojas Y, Gil-Tamayo S, Mosos J, Hernandez F, Castañeda-Cardona C, et al. PMU54 - HOW MUCH DOES IT COST TO TRAIN A PHYSICIAN IN COLOMBIA?. Value in Health. 2018; 21: S317.
- Avila-Guerra M. Simulation in Developing Countries. Neurosurgery. 2014; 74: E343.
- About Cananeurocom. 2022.
- Hubbard Z, Shah A, Ragheb M, Wang S, Jernigan S, et al. Economic
benefit of neurosurgical intervention for infant hydrocephalus in
Haiti. Journal of Neurosurgery Pediatrics. 2019; 24: 306-314.
- Malham G, Wells-Quinn T. What should my hospital buy next?
Guidelines for the acquisition and application of imaging, navigation, and robotics for spine surgery. Journal of Spine Surgery. 2019; 5: 155-165.
- Sferrella S. Radiology business 2022.
- Feigin V, Nichols E, Alam T, Bannick M, Beghi E, et al. Global, regional, and national burden of neurological disorders, 1990-2016:
a systematic analysis for the Global Burden of Disease Study 2016.
The Lancet Neurology. 2019; 18: 459-480.
- Nigeria Living Wage Individual - 2021 Data - 2022 Forecast - 2015-
2020 Historical: Trading economics com: 2022.
- Morgan E, Nwatuzor C: Starting a neurosurgical service in a Southern Nigeria rural community. Prospect, challenges, and future-the
Irrua experience. Egyptian Journal of Neurosurgery. 2020; 35.
- Patel T, Shah S, Pancholy S. Long Distance Tele-Robotic-Assisted
Percutaneous Coronary Intervention: A Report of First-in-Human
Experience. E Clinical Medicine. 2019; 14: 53-58.
- Moylan D, Joffe D, Morse C, Knapp M, Sweid A, et al. Evaluating the
Efficacy of Telestroke Intervention in a Large Community Hospital
Network. Jefferson Digital Commons. 2022.
Miley M, Demaerschalk B, Olmstead N, Kiernan T, Corday D, et al.
- The State of Emergency Stroke Resources and Care in Rural Arizona: A Platform for Telemedicine. Telemedicine and e-Health. 2009;
15: 691-699.
- Cover Story The Robot Will See You Now... Robotics in the Cath Lab
Have Staff Breathing a Sigh of Relief - American College of Cardiology: American College of Cardiology: 2022.