Introduction
The COVID-19 pandemic has created unprecedented challenges to health service delivery around the world, with an adverse
impact on doctors-in-training. In the UK alone it is estimated that
1.5 million elective procedures were cancelled or postponed, resulting in a 33.6% drop-in surgical activity in 2020 [1]. As well as a
burden on patients, this has had a huge impact on trainees, with
each of these procedures representing a lost teaching opportunity. 41% of surgical trainees were redeployed to help with staff
shortage, with 74% of those for longer than four weeks, in addition there was complete loss of procedural training in over 65% of
trainees. Worryingly, only 9% reported that they would meet all
required competencies expected that year [2]. A survey by Choi
et. Al [3] of 440 students from 32 UK medical schools revealed
that 38.4% had their final OSCE cancelled, and 43% had their student assistantships postponed, which had a significant effect on
their confidence in entering first year placements.
The pandemic has created an opportunity to utilise and apply
digital tools to replace most, if not all, face-to-face teaching. Due
to the nature of restrictions, many educational resources including lectures and final examinations had to go online [4,5]. Remote
learning has subsequently shown benefits such as reduced costs
in travel and resources [6], flexibility, and better accessibility[7]
allowing students to continue receiving medical training despite
social distancing. Studies have found that the utilisation of online
resources in place of previously classroom-based teaching has
been well received by trainees and faculty alike [8-10] and could
therefore become essential to medical curricula.
There is limited evidence showing the application of virtual
training to practical tasks such as basic surgical skills, although
students reported positive responses [11-14]. Of these, three
studies have objectively evaluated a virtual teaching programme
of surgical skills by formally assessing performance, but there
have been no reports further evaluating skill retention [12-14].
However, whether virtual training is as effective in teaching surgical skills when compared to traditional face-to-face methods is an
important question to consider.
The aim of this study was to ascertain the feasibility and effectiveness of virtual training of basic surgical skills using the Kirkpatrick model of curriculum evaluation [15].
Methodology
This was a prospective observational cohort study recruiting
medical students, without prior suturing experience, who participated in a series of training sessions on basic suturing techniques
over a total of 6 hours.
The virtual (intervention) group were recruited through the
British Indian Surgical & Medical Associations (BISA/BIMA) for
undergraduate medical students. A Basic Surgical Skills Teaching
Series was advertised through the social media accounts of BISA/
BIMA and was open to all undergraduates across the UK. Students
were asked to complete an application form online, with places
being allocated on a first come first serve basis. The first 24 out
of 150 students to register for the virtual teaching series were
selected for the course. Complete data were obtained from 17
participants in the virtual group as 7 failed to return assessments
to the research team.
Sessions were delivered online through Zoom Video Communications, Inc., where participants received a total of 6 hours of
teaching. Prior to the first session suturing kits funded by ©2022
Sigma Lance and provided by BISA (Supplementary Material)
were sent out including a silicon suturing pad, 3-0 silk sutures, a
needle driver, a pair of toothed and non-toothed forceps, suture
scissors, and a sharps pad for disposal. Industry was not involved
in designing the curriculum, running the teaching or analysing the
results. Sessions were taught by specialist trainees and consultants, with a ratio of three to four participants per tutor in break
out rooms. The structure of the session was as follows; the lead
tutor described the instruments and their use, followed by a demonstration of the suture and knot tie with commentary, then repeated without. Participants were then split into their breakout
rooms and given time to practice along with live feedback from
their tutor. Assessments were performed by the tutors at the end
of the sessions on week one and two, using a validated Objective
Structured Assessment of Technical Skill (OSATS) tool which combined a task-specific checklist and a Likert format Global Rating
Scale (GRS) [16] (Appendix 1), to give a final score out of 21.
The in-person (control) group were recruited from the cohort
of intercalating medical students from University College London, attended conventional face-to-face surgical skills training
sessions. These participants underwent two half day workshops
(total of 6 hours training) on basic suturing skills with the same
equipment and structure of training sessions as the virtual group.
The Kirkpatrick model of evaluation was applied for this curriculum consisting of four levels described below.
Appendix 1
1. OSATS tool
Objective Structured Assessment of Technical Skills (OSTS):
Suturing
Candidate name: Self-assessment: yes/no
(select appropriate): Tutor: Date:
| Checklist |
Yes |
No |
| Selects appropriate instruments |
|
|
| Needle loaded ½ to 2/3 from tip |
|
|
| Bite depth and distance from wound edge appropriate 0.5cm-1cmm |
|
|
| Needle enters tissue perpendicular (90 degree) |
|
|
| Single attempt taking bites |
|
|
| Forceps used to hold skin |
|
|
| Supinates wrist |
|
|
| Approximates wound edges (appropriate eversion) |
|
|
| Secures square knot with hand or instrument tie - surgeons knot first
throw |
|
|
| Appropriate number of throws i.e. 3-4 braided, 6-7 monofilament |
|
|
| Sutures placed appropriate distance apart/equal bites each side |
|
|
| Cuts suture tail correct length |
|
|
| Avoids handling needle with fingers |
|
|
| Avoids torqueing skin i.e. sutures placed incorrectly |
|
|
| Avoids grasping needle tip |
|
|
| Avoids multiple forceps grasps on tissue/damaging tissue or foam
pad |
|
|
Score /16 |
Global rating scale (Please mark/highlight) /5
1- Poor technique, poor manual dexterity/instrument handling
and unacceptable knot/closure
2- In between 1 and 3
3- Moderately good technique, moderate manual dexterity/instrument handling, acceptable knot
4- In between 3 and 5
5- Excellent Technique, excellent manual dexterity, and
excellent knot
Total score: Checklist + global rating scale ( /21)
2. Example Session Feedback Form – In-person group
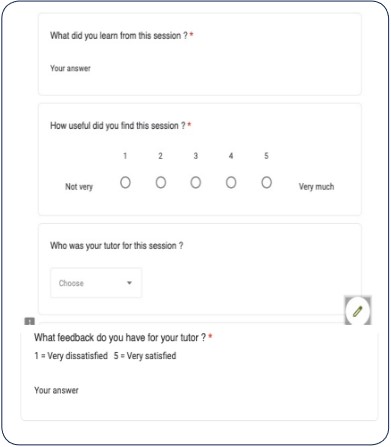
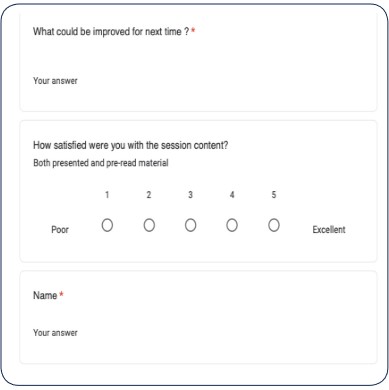
3. Example Session Feedback form - Virtual group
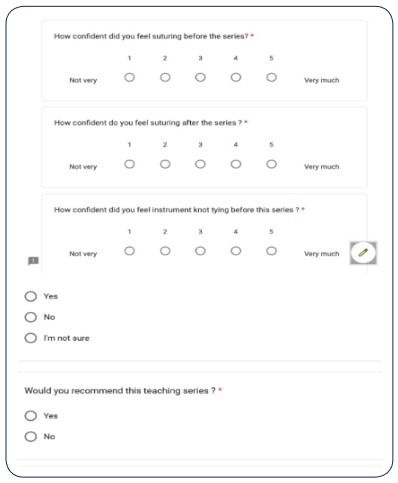
4. Overall feedback form – Virtual and in-person groups
Supplementary material
Sigma Lance © EDGE MK IV - Pre-Cut, Great Value System used
for the virtual group
Level 1 – Participant reaction
Level 1 evaluates reaction towards the learning experience
through standard course evaluation forms assessing how participants perceive the quality and value of training. Feedback questionnaires were completed at the end of each session for both
groups, via Google Forms for virtual and paper handouts for inperson participants (Appendix 1). Questions covered expectations
of the course, usefulness of the sessions, satisfaction with the tutors’ teaching, as well as areas for improvement.
Level 2 – Skill acquisition
Level 2 measures the degree to which training improves participant knowledge and skills. In both groups, the OSATS tool was
used to objectively by the trainers to assess participants’ ability to
perform basic suturing skills at weeks one and two of the course.
Level 3 and 4: Evaluation of skill retention and impact
Change in behaviour was assessed through Google Forms
feedback [Appendix 1] at the end of each training period for both
groups. Questions evaluated confidence in suturing before and
after the teaching series, whether they were more likely to pursue a career in surgery or organise theatre experience, and if they
would recommend the course.
In addition to this, we objectively measured skill retention in
both groups at four months after completion of their respective
courses. The virtual group was requested to submit self-recorded
videos of basic suturing tasks, whilst the in-person group were invited back to a face-to-face session for reassessment of the same
tasks. The skill retention assessments were done by a single specialist level assessor using the same OSATS tool; weeks one and
two mean scores were then compared to this.
Data collection and statistical analysis
We collected demographic information of all participants
which included year of university course, and previous surgical
experience. Mean OSATS scores were calculated for weeks one,
two and skill retention sessions in both groups. An independent
sample t-test was used to compare the mean scores of virtual versus in-person groups at each stage. Each groups’ progression from
week one to two, was measured by calculating the mean scores
and compared using a paired samples t-test. Finally, skill retention in each group was evaluated using paired samples t-test to compare mean scores of weeks one and two. Two tailed p values were
considered significant if under 0.05. Analysis was performed using
IBM SPSS statistics version 28.0.1.1.
Results
Demography
In total 48 participants underwent the training, with 13 (54.2%)
females in the virtual group, ranging from year one to four medical students from ten different universities across the UK. The
in-person group were all intercalated medical students after their
third year and consisted of 10 (41.7%) females. No participants
had any prior exposure or formal training of surgical skills.
Evaluation of Curriculum
Complete evaluation data were received from 17 (70.8%) virtual participants at week one and 16 (66.7%) after week two while
course feedback was collected from 24 (100%) participants from
the in-person group.
Level 1 – Participant reaction
Participant reaction from both groups was highly positive (Figures 1 and 2), with feedback from virtual sessions showing comparable favourable opinions to that of face-to-face sessions. Overall, virtual participants found their sessions to be highly useful,
with an average score of 4.68/5, in comparison to 5/5 for the inperson group. The virtual group were overall thoroughly satisfied
with the contents of the session, giving an average satisfaction
score of 4.79/5.
Points praised in virtual teaching were the interactivity of
the sessions, clarity of demonstrations, and quality of teaching
from the tutors. Participants highlighted the individual feedback provided, and described the tutors as “helpful", “engaging”
and “friendly”. Similarly, the in-person group complimented the
equipment and tutors providing “really helpful advice” with “well
taught” sessions.
Issues highlighted in the virtual training were that of time
restrictions and technical limitations. This included issues with
camera focus and angle, with screen limitations sometimes preventing a clear view of demonstrations. Problems with internet
connectivity were also noted by some participants, causing interruption to the session.
Level 2 - Skill acquisition: Objective evaluation
Both virtual and in-person groups showed progression (Figure
3), with the mean week one and two scores of the virtual participants (n=16) being 15.94 (SD 2.05) and 18.97 (SD 2.00) respectively (mean difference 3.03, t=4.07, SD 2.98, 95% CI 1.44-4.62,
p=0.001), whilst for the in-person group (n=24) mean scores were
17.67 (SD 1.59) and 18.44 (SD 1.36) respectively (mean difference
0.77, t=2.47, SD 1.52, 95% CI 0.13-1.41, p=0.02).
Comparing group performance at each week demonstrated
that the virtual group was out performed by the in-person in
week one, with mean scores of 15.71 (SD 2.20) (n=17) and 17.67
(SD 1.59) (n=24) respectively (mean difference 1.96, t= 3.31, SE
0.59, p=0.002). However, by week two, both groups had comparable scores with virtual and in-person scoring 18.97 (SD 1.94)
and 18.44 (SD 1.36) respectively (mean difference 0.53, t=1.04, SE
0.52, 95% CI -0.51-1.57, p=0.31).
Level 2 - Skill acquisition: Self-evaluation
From 10 (41.7%) virtual group responses to the final feedback
survey, participants clearly felt that they had improved in specific
skills set out by the course, with their confidence in instrument tying improving from an average score of 1.6/5 before the course to
4.4/5 after (corresponding to a 175% improvement in self-rated
score), and suturing (1.4 to 4.2/5 i.e. a 200% improvement). From
9 (37.5%) in-person responses, confidence in instrument tying improved from 2.56/5 before the course to 4.56/5 after the course
(78% increase) and 2.44 to 4.44/5 (82% increase) for suturing.
Level 3 and 4 evaluation of skill retention and impact: Objective evaluation
Upon completion of the training, self-recorded skill retention videos were submitted at four months by a total of 13 (76.5%),
out of the 17 who returned assessments, from the virtual group,
whilst 8 (33.3%) from the in-person group returned for reassessment. Skill retention was analysed for these participants, within
and between groups. Comparison between groups revealed that
the virtual group had a significantly lower mean score of 17.88
(SD 1.92) than the in-person group with 19.50 (SD 0.75) (mean
difference 1.62, t=2.26, SE 0.72, 95% CI 0.12-3.11, p=0.04).
However, when looking independently at each group’s scores,
both were able to maintain or improve their performance at 4
months. From the virtual group, week one to skill retention mean
scores (n=13) of 16.08 (SD 2.18) and 17.88 (SD 1.92) respectively,
showed a significant improvement of 1.80 (t=2.23, SD=2.93, 95%
CI 0.04-3.58, p=0.046). Their week two and skill retention mean
scores (n=13), 19.27 (SD 1.67) and 17.88 (SD 1.92) respectively,
had a mean difference of 1.39 (t=1.62, SD 3.09, 95% CI -0.48-3.25,
p=0.132), although statistically this was not significant.
The in-person group from week one to skill retention (n=8) also
showed an improvement with respective mean scores of 18.75
(SD 1.41) and 19.50 (SD 0.75) (mean difference 0.75, t=1.60, SD
1.60, 95% CI -2.09-0.59, p=0.23). Similarly, their mean scores in
week two of 18.88 (SD 1.06) (mean difference 0.62, t=1.53, SD
1.53, 95% CI -1.90-0.65, p =0.29) showed improvement, which
again was not significant, likely due to a small comparative sample
size.
Level 3 and 4 evaluation of skill retention and impact: Self-evaluation
Further ‘Overall Feedback’ responses were submitted by 10
virtual and 9 in-person participants, assessing the course’s impact
on participant’s behaviour. 100% of participants in both groups
would recommend their respective teaching series and were
more likely to organise theatre experience following their course.
100% of virtual participants responded they were more likely to
pursue a career in surgery after their course, in contrast to 88.9%
of in-person participants.
Discussion
Our study aimed to establish whether virtual teaching is a
feasible and effective means of providing basic suturing training
when compared to the traditional face-to-face approach. This
curriculum was pragmatically applied to medical students and
evaluated comprehensively by applying the Kirkpatrick model,
using objective assessments. Our results have demonstrated that
participants were able to achieve similar progression in basic
suturing skills after two weeks of virtual teaching, compared to
traditional training. Furthermore, participants were able to retain skills learnt remotely, and apply them after four months to a
similar level of competency as achieved by the end of their training. Lastly, feedback from the participants was equally positive in
both groups and enthused many to potentially pursue a career in
surgery.
Recent years have seen a rapid development in online technological advances, and the effects of the pandemic has accelerated
the transition to remote working and learning. This is particularly
pertinent now given the significant disruption to surgical training
caused by the pandemic, highlighted by the annual GMC report in
202117. This revealed that 40% of trainees felt they were not on course to undertake the expected number of operative and practical procedures due to a reduction in opportunities to gain the
required curriculum competencies. Furthermore, 40% of trainees
felt that they were not provided with alternatives to compensate
for these lost opportunities. As medical education has shifted towards distance learning, it is important that surgical training can
also adopt effective virtual practices so that technical skills can
continue to be taught at the same frequency and to the same
standard.
The application of virtual teaching for basic surgical skills is
also considered an appropriate method to test and evaluate the
impact of teaching on those skills. Basic surgical skills have been
highlighted by the General Medical Council (GMC) as a technical
procedure competency in newly qualified doctors [18], yet despite this, basic suturing is only present in a minority of medical
school curricula [19]. This combined with the challenges posed
to medical education by the pandemic will undoubtedly lead to
reduced student exposure to surgical training. In attempts to address this there have been innovative examples of teaching methods employed [14,20].
In this study we applied a robust evaluation methodology
through Kirkpatrick’s model. Firstly, we demonstrated positive
participant reaction that correlated to the existing literature
[9,11], with overall high satisfaction with the course, including
positive feedback on the level of interaction with the faculty. This
however, required a high faculty to participant ratio, which can be
afforded virtually, with training sessions easily attended by surgical tutors without impacting on their clinical work.
Secondly, we applied OSATS, a validated and reliable tool to
objectively evaluate suturing skills [21-23]. The OSATS tool used
consists of two components; a task-specific checklist, which
breaks down the surgical task into discrete segments, and a GRS,
which gives a generic Likert scale scoring of overall technical ability. A modified version of this tool specific to basic surgical suturing was applied as a formative and summative assessment in
our study, allowing us to track participant progression from weeks
one to two as well as providing valuable feedback.
Interestingly, performance was evidently weaker in virtual delegates after the first teaching session than those taught face-to-face, suggesting that skill acquisition may be slower for virtually
teaching basic suturing skills. Potential explanations may be that
visuospatial concepts, such as knot-tying, may be more difficult to
grasp through a two-dimensional screen, and technical glitches
such as Wi-fi interruptions may cause lagging of video demonstrations. As such, issues noted in the feedback evaluation highlighted the necessity of ensuring good internet connection, camera
resolution and view, which should be taken into account to improve future courses. Additional limitations exist within a virtual
classroom which impede the flow of the teaching, such as the tutor having to switch from screen-to-screen to assess and provide
feedback to participants individually.
Our study showed that at four months after the end of training both groups exhibited skill retention with higher mean OSATS
scores when compared to the first week, and comparable mean
scores at week two when they had had the most teaching and
practice. The in-person group had a higher but non-significant
mean score at the skill retention session compared to the virtual group, however, we were only able to assess a small sample of
the control group at four months, which may have led to an involuntary selection bias towards more committed participants who
continued to practice and potentially skewing the true results. On
the other hand, this subset in-person group did not have the kit
at home to practice yet still demonstrated their best scores at skill
retention. Final feedback responses also indicated behavioural
change in participants, whereby students felt more encouraged to
involve themselves in theatre opportunities, as well as potentially
pursue a career in the surgical field.
Limitations
This study has some limitations including a small sample size
and lack of randomisation of both groups. Additionally, there
was an incomplete collection of data, which was evident in both
groups for different reasons. The virtual assessments relied on tutors and participants to email forms back to the researchers, and
as there were multiple tutors in each session it was difficult to
retrieve a full data set. This led to missing data which necessitated
the exclusion of those participants from analysis. Meanwhile, the
in-person group had mandatory attendance for face-to-face training as part of their iBSc intercalated year, therefore, there was
full attendance to both training sessions with complete collection
of data. However, when evaluating skill retention, fewer students
returned for the face-to-face reassessment session. This lack of
attendance was due to conflicting medical school commitments
as they entered their clinical years. In contrast, the majority of virtual students submitted skill retention videos after four months,
highlighting the convenience of virtual teaching and assessment,
as these participants were able to submit videos from their own
home at a time of their convenience. Additionally, this was easier
for the tutor who could assess videos at a time of their choosing.
Taking this into consideration for reassessment methods in future
training curricula, if feasible financially, suturing kits could be provided for students taught face-to-face, allowing not only at-home
practice but also easier reassessments for both tutor and student.
Conclusion
This study demonstrated that virtual teaching of basic surgical
skills can be a feasible and useful adjunct to traditional surgical
teaching. Future curricula should consider the use of digital plat-
forms, perhaps in a hybrid approach, to ensure that missed train-
ing opportunities can be compensated.
Declarations
Funding: ©2022 Sigma Lance sponsored the use of suturing
kits for BISA tutors and provided BISA students with a discount
code for suturing kits on their site.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Dobbs TD, Gibson JAG, Fowler AJ, Abbott TE, Shahid T, et al. Surgical activity in England and Wales during the COVID-19 pandemic:
a nationwide observational cohort study. Br J Anaesth. 2021; 127:
196-204.
- COVID-STAR Collaborative Study Group. COVID-19 impact on Surgical Training and Recovery Planning (COVID-STAR) - A cross-sectional observational study. Int J Surg. 2021; 88: 105903.
- Choi B, Jegatheeswaran L, Minocha A, Alhilani M, Nakhoul M, et al.
The impact of the COVID-19 pandemic on final year medical students in the United Kingdom: A national survey. BMC Med Educ.
2020; 20: 1-11.
- Papapanou M, Routsi E, Tsamakis K, et al. Education and learning
Medical education challenges and innovations during COVID-19
pandemic. Postgrad Med J. 2022; 98: 321-327.
- The Guardian. Medical students take final exams online for first
time, despite student concern. 2020.
- Mukhtar K, Javed K, Arooj M, Sethi A. Advantages, Limitations and
Recommendations for online learning during COVID-19 pandemic
era. Pak J Med Sci. 2020; 36: S27.
- Papapanou M, Routsi E, Tsamakis K, et al. Medical education challenges and innovations during COVID-19 pandemic. Postgrad Med
J. 2022; 98: 321-327.
- Brown R, Humphreys A, Bamford R, Mutimer J, Coulston J. Mapping out a virtual surgical curriculum: opinions on a core surgical
training programme with technology-enhanced learning.
- Figueroa F, Figueroa D, Calvo-Mena R, Narvaez F, Medina N, et al.
Orthopedic surgery residents’ perception of online education in
their programs during the COVID-19 pandemic: should it be maintained after the crisis? Acta Orthop. 2020; 91: 543-546.
- Kam CT, Rait J, Brooke-Ball H, Ojofeitimi O. Virtual surgical education for foundation doctors in the United Kingdom during COVID-19 pandemic: A qualitative study. Annals of Medicine and Surgery. 2022; 80: 104192
- Co M, Chu KM, Kent-Man Chu C. Distant surgical teaching during
COVID-19-A pilot study on final year medical students. 2020.
- McGann KC, Melnyk R, Saba P, Joseph J, Glocker RJ, et al. Implementation of an E-Learning Academic Elective for Hands-On Basic
Surgical Skills to Supplement Medical School Surgical Education. J
Surg Educ. 2021; 78: 1164-1174.
- Zaghal A, Marley C, Rahhal S, Hassanieh J, Saadeh R, et al. Face-to-face versus distance learning of basic suturing skills in novice
learners: a quantitative prospective randomized trial. BMC Med
Educ. 2022; 22.
- Co M, Chung PHY, Chu KM. Online teaching of basic surgical skills
to medical students during the COVID-19 pandemic: a case–control study. Surg Today. 2021; 51: 1404-1409
- Kirkpatrick DL. The Four Levels of Evaluation. Evaluating Corporate
Training: Models and Issues. 1998; 95-112.
- Asif H, McInnis C, Dang F, Ajzenberg H, Wang PL, et al. Objective
Structured Assessment of technical skill (OSATS) in the Surgical
Skills and Technology Elective Program (SSTEP): Comparison of
peer and expert raters. Am J Surg. 2022; 223: 276-279.
- General Medical Council (GMC). A State of Medical Education and
Practice in the UK 2021 - Annual Report. 2021.
- General Medical Council (GMC). Practical Skills and Procedures.
2019.
- Davis CR, Toll EC, Bates AS, Cole MD, Smith FCT. Surgical and procedural skills training at medical school -a national review. International Journal of Surgery. 2014; 12: 877-882.
- Kang CM. Non-face-to-face basic surgical skill education in the
novel coronavirus disease 2019 (COVID-19) outbreak: obstacle vs.
opportunity? Ann Surg Treat Res. 2020; 99: 247.
- Reznick R, Regehr G, MacRae H, Martin J, McCulloch W. Testing
technical skill via an innovative “bench station” examination. Am J
Surg. 1997; 173: 226-230
- Martin JA, Regehr G, Reznick R, MacRae H, Murnaghan J, et al. Objective structured assessment of technical skill (OSATS) for surgical
residents. British Journal of Surgery. 1997; 84: 273-278
- Vaidya A, Aydin A, Ridgley J, Raison N, Dasgupta P, et al. Current
Status of Technical Skills Assessment Tools in Surgery: A Systematic
Review. Journal of Surgical Research. 2020; 246: 342-378.