Introduction
The introduction of two new fully cementless acetabular im-
plants in 2008 has revolutionized total hip arthroplasty (THA) as
well as THA acetabular revision surgery in the past decade. The
use of Trabecular Metal (TM) implants has shown satisfactory re-
sults since their introduction in the late twentieth century [1,2].
Despite the development of several different designs and operat-
ing techniques, elimination of the most common cause of pros-
thesis failure, and subsequently revision acetabular surgery, has
not yet been achieved. Risk of a revision significantly increases
in the second decade following primary THA and is mostly due
to loosening of the acetabular component [3,4]. With the grow-
ing demand for THA as well as acetabular revision surgery, use
of Trabecular Titanium (TT) has increased significantly [5]. Pure
Trabecular Titanium (Delta Trabecular Titanium, Limacorporate,
Udine, Italy) is designed as a honeycomb-like structure, with
highly porous material consisting of multi-planar hexagonal inter-
connected cells [6,7]. In vivo studies have shown that Trabecular
Titanium is capable of inducing complete and quick osseo integra-
tion by means of its porous, hexagonal cell structure [8,9]. Use
of the Electron Beam Melting (EBM) technique produces the mi-
crostructure Trabecular Titanium, which provides continuity be-
tween the solid part of the acetabular cup cavity and the exter-
nal honeycomb-like structure. This one-step production process
makes the Trabecular Titanium less susceptible for common risks
in coated implants, such as detachment [9,10]. The Delta One TT
THA is designed to have a reduced caudal size in order to be ap-
plicable in challenging conditions such as hip dysplasia or revision
surgery. The Delta Revision TT THA has a cage construct with a
hook and three arms to provide the implant with sufficient stabil-
ity. In order to further enhance stability, it is possible to insert
screws through the holes of the arms, fixating them to the pelvis
[1,7]. This makes the Delta One TT and Delta revision TT systems
promising implants, especially for complex primary surgery (due
to osteonecrosis, dysplasia or otherwise poor bone quality) or
challenging revision surgery [11].
Orthopedic surgeons will often opt for placement of a Dual
Mobility Cup (DMC) in patients with higher preoperative risk of
instability and possible dislocation after THA. A DMC consists of
a small prosthetic head inside a larger polyethylene liner. Primary
motion occurs between the femoral head of the prosthesis and
the inner surface of the polyethylene liner, allowing a secondary
motion to occur between the polyethylene liner and the acetabu-
lar cup [10,12]. This construction has proven to prevent implant
dislocation, improve range of motion, and decrease the risk of
dislocation [13,14]. Utilization of the TT scaffold is expected to
reduce the incidence of (aseptic) loosening of acetabular compo-
nent of the prosthesis. To the best of our knowledge limited data
has been published in literature regarding the survival of TT ace-
tabular implants, even more so regarding the use of TT implants in
complex primary and acetabular revision surgery. The aim of this
study was to evaluate five-year survival of the Delta One TT and
Delta Revision TT systems in patients undergoing primary com-
plex or acetabular revision surgery.
Materials and methods
A retrospective, single-center cohort study was performed
using prospectively collected data from our hospital’s electronic medical records. We included all patients who received a Delta
One TT or Delta Revision TT implant in acetabular (revision) sur-
gery between April 2011 and December 2014.
ASA classification was determined by the anesthesiologist dur-
ing routine pre-operative screening [15]. Routine pre-operative
antibiotic prophylaxis consisted of two grams of Cephazolin, in-
travenously administered at least 30 minutes before the start
of the procedure. All patients were operated one by one of four
experienced orthopedic surgeons. Surgery was performed under
general anesthesia, via the direct lateral approach to the hip as
first described by Hardinge except for two cases where an ante-
rior approach according to Smith-Petersen was performed based
on preference of the surgeon [16,17]. A DMC was implanted in pa-
tients with higher risk of instability and possible dislocation after
THA. Acetabular defects were evaluated during the surgical pro-
cedure, classified according to the Paprosky classification, and ad-
dressed if necessary [18]. Defects were primarily corrected by use
of autograft, harvested from the patient’s iliac crest, or allograft
bone substitutes. When needed, further defects were addressed
by use of hemispheric modules or augments.
Venous Thromboembolic (VTE) prophylaxis consisted of Na-
droparine (low molecular weight heparin) 9500 IE/mL daily. Pa-
tients weighing less than 100 kg received 0.3 ml (2850 IE) and
those weighing more than 100 kg received 0.6 ml (5700 IE) once
daily. This was administered during six weeks starting the first
post-operative day. Postoperative x-rays in anteroposterior and
lateral views were routinely performed one day after surgery to
confirm correct placement of the prosthesis. Patients were in-
structed by a physical therapist to follow standard precautions
after hip replacement surgery, according to hospital standards.
Partial weight-bearing mobilization using a walking aid was al-
lowed for six weeks after surgery, followed by full weight-bearing
mobilization.
Follow-up occurred according to our hospital standard pro-
tocol, i.e. patients were reviewed at our outpatient clinic at two
weeks, six weeks, three months, one year, three years and five
years postoperatively. X-rays in both anteroposterior and lateral
views were routinely performed. Cut-off point for follow-up was
determined as December 31st 2019 and maximum follow-up time
was set at five years.
Primary outcome consists of survival of the Delta One TT and
the Delta Revision TT cup. Also, clinical outcomes were analyzed,
and peri- and postoperative complications were registered and
graded according to the Clavien-Dindo classification [19].
Baseline characteristics and complications were studied us-
ing descriptive statistics, with mean (SD) and numbers (%) shown
when appropriate. To study the survival a Kaplan-Meier analysis
was performed and to study the effect of Paprosky score and
bonegraft on survival, a Pearson Chi-square test was performed
on the status at five years. Statistical significance is defined as a p-
value <0.05. Analysis was performed using IBM SPSS version 27.0
(IBM corp.).
This research has been approved by the IRB of the authors’ af-
filiated institution.
Results
72 patients received a Delta TT implant in complex primary and
acetabular revision surgery. The study population consisted of 18
(25%) male and 54 (75%) female patients, with a mean age of 72.4
(SD 12.4) years (Table 1). The prosthesis was implanted on the
right side in 29 (40.3%) cases and on the left side in 43 (59.7%)
cases. No bilateral procedures were performed.
The Delta One TT cup was placed in 52 cases; 20 patients re-
ceived a Delta Revision TT cup. The indication for surgery was
aseptic loosening of previous prosthesis in 18 cases (25%), dislo-
cation in 13 cases (18%), polyethylene wear in eight cases (11%),
Girdlestone in seven cases (9.8%), instability of prior implant in
seven cases (9.8%), migration of prior implant component in three
cases (4.2%) and osteolysis in three cases (4.2%), or ‘other’ in 13
cases (18%, e.g. secondary osteoarthritis due to hip dysplasia or
metallosis and pseudotumor after metal-on-metal prosthesis).
Dual mobility cups were implanted in 51 cases. Patients in our
cohort presented with Paprosky scores varying from 1 to 3B (Ta-
ble 1). When present, defects were corrected by use of autograft
bone substitution, harvested from the pelvic ring, in six cases
(8.3%) or allograft bone substitution in 18 cases (25%) in order to
provide sufficient stability for the implanted prosthesis. Five cases
(6.9%) received both varieties of bone grafts in order to achieve
optimal stability.
A total of eight patients required cup revision of their Delta
implant resulting in a cumulative survival of the Delta One TT and
Delta Revision Cup of 88.9% after five years of follow up (Figure 1).
Indications for revision surgery were prosthetic joint infec-
tion (PJI) in four patients (5.6%), aseptic loosening in one patient
(1.4%), persistent instability of the affected hip in two patients
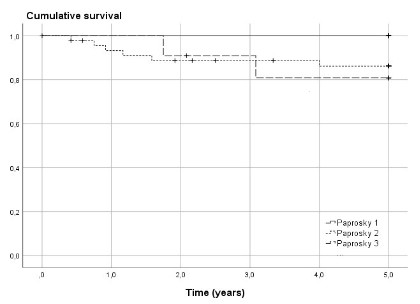
(2.8%) and migration of the cup in one patient (1.4%). Cumulative
survival of the implants for the Paprosky classification groups was
100% in Paprosky 1, 87.0% in Paprosky 2 and 81.8% in Paprosky
3 (Figure 2), but Paprosky score had no significant effect on the
survival (p = 0.272).
Also, the use of autograft, allograft, both types of bone substi-
tution, or no bone substitution did not have an effect on risk of
revision of the implant (p=0.211).
Eight patients (11.1%) died during follow-up. Of these eight,
one patient deceased on the third postoperative day from the ef-
fects of abdominal ischemia and aspiration. The remaining seven
patients died of unrelated causes during the follow-up period.
Three of the included patients underwent revision surgery af-
ter placement of a Delta TT prosthesis; however, the implanted
cups were not revised during these procedures. For this reason,
these three patients were classified as non-failure. One patient
needed revision due to failure of the dual-mobility liner, therefore
the cup required no revision and was left in situ. The second pa-
tient was in need of revision for complaints of instability due to a
stem implanted with too much anteversion. The stem was revised
and a 20° liner was placed. The third patient needed revision for
a dislocation which could not be treated by closed reduction. The
liner was exchanged for a dual-mobility liner.
Table 1: Baseline patient characteristics and surgery outcome.
|
Study population (N=72) |
No revision (N=64) |
Revision (N=8) |
| Age (average), years |
72.4 (SD 12.4) |
72.7 (SD 12.8) |
69.9 (SD 8.8) |
| Sex |
| ♀ |
54 (75.0%) |
46 (71.9%) |
8 (100%) |
| ♂ |
18 (25.0%) |
18 (28.1) |
0 (0%) |
| BMI |
26.6 (SD 4.1) |
26.3 (SD 3.7) |
29.1 (SD 6.1) |
| Laterality |
| Left |
43 (59.7%) |
41 (64.1%) |
2 (25.0%) |
| Right |
29 (40.3%) |
23 (35.9%) |
6 (75.0%) |
| Acetabular defect |
| Paprosky I |
15 (20.8%) |
15 (23.4 %) |
0 (0%) |
| Paprosky II |
46 (63.9%) |
40 (62.5%) |
6 (75.0%) |
| Paprosky III |
11 (15.3%) |
9(14.1%) |
2 (25.0%) |
| Acetabular defect |
| Delta One TT |
52 (72.2%) |
46 (71.9%) |
6 (75.0%) |
| Delta Revision TT |
20 (27.8%) |
18 (28.1%) |
2 (25.0%) |
| Bone graft |
| Allograft |
18 (25.0%) |
15 (23.4%) |
3 (37.5%) |
| Autograft |
6 (8.3%) |
4(6.25%) |
2 (25.0%) |
| Both |
5 (6.9%) |
4(6.25%) |
1 (12.5%) |
| None |
40 (55.6%) |
38 (59.4%) |
2 (25.0%) |
| Missing data |
3 (4.2%) |
3 (4.7%) |
- |
Discussion
Our study found a cumulative survival of the Delta One TT and
Revision TT cups of 88.9% after five years. Compared to the lit-
erature this is somewhat lower. Perticarini et al. report a survival
of the Delta TT cup after five years 99.3% [3]. This difference in
survival may be due to the fact that in our study Delta One TT and
Revision TT cups were used for complex primary and acetabular
revision surgery, as opposed to the Delta TT used for primary ac-
etabular surgery performed by Perticarini et al.
Whereas several studies have been conducted on short-to
mid-term clinical outcomes of Trabecular titanium cups, such as
Delta TT, Delta One TT and Revision TT cups, to our knowledge,
few studies have been conducted on the use of these cups in com-
plex primary and revision surgery. Munegato et al. report survival
of the Revision TT cup in 37 acetabular revisions of 91.7% when
using the cup for revision surgery with an indication other than
aseptic loosening. In this study mean follow-up was 3.3 years
(range 1.0-7.6 years) [20].
Perticarini et al. assessed the mid-term outcomes of Trabecu-
lar Titanium cups in revision surgery in 104 cases with a mean
follow-up of 7.6 years (range 2-12.2 years), reporting a survival
of 88.54% [21]. This is similar to the mid-term survival outcomes
of Delta TT systems, both Delta One TT and Revision TT cups in
complex primary or acetabular revision arthroplasty found in our
study.
With one case of aseptic loosening, our results are comparable
to those published by Gallart et al. [1] and Perticarini et al. [3,21]
on the use of Trabecular Titanium components, and to the results
published for the Trabecular Metal™ (TM) system by Zimmer [22].
Although recent literature suggests higher Paprosky bone de-
fect scores are associated with higher risk for implant failure our
study found no significant difference in revision rates when con-
sidering Paprosky bone defect classification [1,23,24].
Cumulative survival of the Delta One TT and Revision TT cups
as found in this study are in line with recent literature on use of
trabecular metal cups and are therefore regarded by the authors as a reliable representation of implant survival in primary complex
and acetabular revision surgery.
It should be noted that our study was focused on complex
primary acetabular surgery and need for revision of previous im-
plants as indication for surgery. For this reason, the outcomes of
this study should be interpreted as such and not as outcomes of
the use of implants in simple primary acetabular surgery. Further-
more, outcome data for Delta One TT and Revision TT was pooled.
Limitations
This study has two limitations. Firstly, the retrospective design
with its inherent limitations. We expect that for the execution of
the study a prospective design would not have yielded different
results as all parameters were collected from the hospital infor-
mation system and patient selection would not have been differ-
ent. Secondly, our study presents mid-term follow-up results and
further long-term follow-up is needed in order to gain valuable in-
sight in the long-term reliability of this particular type of implant.
However, the current results are valuable information concerning
these systems.
Conclusion
Five-year survival of the Delta One TT and Delta Revision TT ac-
etabular systems shows promising and encouraging results in pa-
tients undergoing primary complex or acetabular revision surgery.
References
- Gallart X, Fernandez-Valencia JA, Riba J, Bori G, Garcia S, et al. Tra-
becular TitaniumTM cups and augments in revision total hip ar-
throplasty: clinical results, radiology and survival outcomes. Hip
Int. 2016; 26: 486-491.
- Unger AS, Lewis RJ, Gruen T. Evaluation of a porous tantalum un-
cemented acetabular cup in revision total hip arthroplasty: clinical
and radiological results of 60 hips. J Arthroplasty. 2005; 20: 1002-
1009.
- Perticarini L, Zanon G, Rossi SM, Benazzo FM. Clinical and radio-
graphic outcomes of a trabecular titanium acetabular component
in hip arthroplasty: results at minimum 5 years follow-up. BMC
Musculoskelet Disord. 2015; 16: 375.
- Howard JL, Kremers HM, Loechler YA, Schleck CD, Harmsen WS,
Berry DJ, et al. Comparative survival of uncemented acetabular
components following primary total hip arthroplasty. J Bone Joint
Surg Am. 2011; 93: 1597-1604.
- Nečas L, Katina S, Uhlárová J. Survival analysis of total hip and knee
replacement in Slovakia 2003-2011. Acta Chirurgiae Orthopaedi-
cae Et Traumatologiae Cechoslovaca. 2013; 80.
- Marin E, Fusi S, Pressacco M, Paussa L, Fedrizzi L. Characterization
of cellular solids in Ti6Al4V for orthopaedic implant applications:
Trabecular titanium. J Mech Behav Biomed Mater. 2010; 3: 373-
381.
- Steno B, Kokavec M, Necas L. Acetabular revision arthroplasty us-
ing trabecular titanium implants. Int Orthop. 2015; 39: 389-395.
- Benazzo F, Botta L, Scaffino MF, Caliogna L, Marullo M, Fusi S, et al.
Trabecular titanium can induce in vitro osteogenic differentiation
of human adipose derived stem cells without osteogenic factors. J
Biomed Mater Res A. 2014; 102: 2061-2071.
- Bertollo N, Da Assuncao R, Hancock NJ, Lau A, Walsh WR. Influence
of electron beam melting manufactured implants on ingrowth and
shear strength in an ovine model. J Arthroplasty. 2012; 27: 1429-
1436.
- Parthasarathy J, Starly B, Raman S, Christensen A. Mechanical eval-
uation of porous titanium (Ti6Al4V) structures with electron beam
melting (EBM). J Mech Behav Biomed Mater. 2010; 3: 249-259.
- De Meo F, Cacciola G, Bellotti V, Bruschetta A, Cavaliere P. Tra-
becular Titanium acetabular cups in hip revision surgery: mid-term
clinical and radiological outcomes. Hip Int. 2018; 28: 61-65.
- Cuthbert R, Wong J, Mitchell P, Kumar Jaiswal P. Dual mobility in
primary total hip arthroplasty: current concepts. EFORT Open Rev.
2019; 4: 640-646.
- Schmidt A, Batailler C, Fary C, Servien E, Lustig S. Dual Mobility
Cups in Revision Total Hip Arthroplasty: Efficient Strategy to De-
crease Dislocation Risk. J Arthroplasty. 2020; 35: 500-507.
- Batailler C, Fary C, Verdier R, Aslanian T, Caton J, Lustig S. The evo-
lution of outcomes and indications for the dual-mobility cup: a sys-
tematic review. Int Orthop. 2017; 41: 645-659.
- Wolters U, Wolf T, Stutzer H, Schroder T. ASA classification and
perioperative variables as predictors of postoperative outcome. Br
J Anaesth. 1996; 77: 217-222.
- Hardinge K. The direct lateral approach to the hip. J Bone Joint
Surg Br. 1982; 64: 17-19.
- Smith-Petersen MN. Approach to and exposure of the hip joint for
mold arthroplasty. J Bone Joint Surg Am. 1949; 31A: 40-46.
- Paprosky WG, Perona PG, Lawrence JM. Acetabular defect clas-
sification and surgical reconstruction in revision arthroplasty. A
6-year follow-up evaluation. J Arthroplasty. 1994; 9: 33-44.
- Dindo D, Demartines N, Clavien PA. Classification of surgical com-
plications: a new proposal with evaluation in a cohort of 6336 pa-
tients and results of a survey. Ann Surg. 2004; 240: 205-213.
- Munegato D, Bigoni M, Sotiri R, Bruschetta A, Omeljaniuk RJ, Turati
M, et al. Clinical and radiological outcomes of acetabular revision
with the Delta Revision TT cup. Hip Int. 2018; 28: 54-60.
- Perticarini L, Rossi SMP, Medetti M, Benazzo F. Clinical and radio-
logical outcomes of acetabular revision surgery with trabecular
titanium cups in Paprosky type II and III bone defects. J Orthop
Traumatol. 2021; 22: 9.
- Jain S, Grogan RJ, Giannoudis PV. Options for managing severe ace-
tabular bone loss in revision hip arthroplasty. A systematic review.
Hip Int. 2014; 24: 109-122.
- Garcia-Cimbrelo E, Cruz-Pardos A, Garcia-Rey E, Ortega-Chamarro
J. The survival and fate of acetabular reconstruction with impac-
tion grafting for large defects. Clin Orthop Relat Res. 2010; 468:
3304-3313.
- Theil C, Schmidt-Braekling T, Gosheger G, Moellenbeck B, Schwar-
ze J, Dieckmann R. A single centre study of 41 cases on the use
of porous tantalum metal implants in acetabular revision surgery.
BMC Musculoskelet Disord. 2019; 20: 238.