Introduction
Cleft lip and palate are among the commonest congenital ab-
normalities affecting the head and neck region [1]. A Cleft is a de-
fect/opening that can affect the lip, alveolus, hard palate, and soft
palate, either in combination or in isolation. Cleft lip and palate
can occur either in combination with syndromes, in isolation, or
as part of other associated deformities. Congenital heart diseases
are most commonly associated with orofacial clefts and in this
case, screening for heart anomalies should be done in a child born
with orofacial clefts [2]. Children born with CLP may experience
trouble with feeding, hearing, speech, and dentition along with
its psychosocial effects of it which indeed can be corrected with
proper surgery, psychological intervention, and speech therapy
[3].
Incidence of Cleft Lip (CL), Cleft Palate (CP), and both (CLP)
have been studied throughout the globe. In Pakistan, it has been
found that cleft lip and/or cleft palate were present in 1.91 per
1000 births (1 per 523 births) [4]. Although, one of the most con-
genital anomalies in newborns, the prevalence of cleft lip and
palate varies worldwide owing to different factors contributing
to it. In terms of gender, cleft lip and palate in combination are
more prevalent in males as compared to isolated cleft palate be-
ing dominated in females [5].
Exact etiological factors that lead to cleft lip and palate are
currently being debated, but many factors do contribute to it.
Pregnant females taking teratogenic drugs leading to a child be-
ing born with cleft lip and palate along with radiation exposure,
maternal diabetes, maternal smoking, alcohol consumption, and
family history are among the commonest causes associated with
CLP [6]. It has been proven that early treatment of a child being
born with a cleft lip and palate leads to normal growth and devel-
opment along with normal speech, hearing, dentition, and feed-
ing abilities [7,8]. Moreover, if the treatment for such children is
not provided then all of these functions are affected to various
degrees which not only has physical but psychological impacts as
well. Early surgical treatment of CLP is the best choice for the child
to have normal development and fewer chances of handicapped
life.
When a child does not undergo surgical treatment, compli-
cations later on in life may develop [9]. Although treatment op-
tions are offered to adults who have CLP untreated during their
childhood, speech, in particular, remains affected with the rest
of the functions such as dentition, feeding, and hearing abilities
positively enhanced. Knowledge and awareness of CLP are now
considered to be prime concerns for parents due to its common
occurrence. CLP is a preventable and treatable condition that can
be very beneficial to restore normal life physically and psychologi-
cally for the affected child. Lack of knowledge about cleft lip and
palate has been known to be the primary reason for negligence
among the general population. Awareness levels of the parents
have been known to have a profound role in developing an at-
titude to provide the patients with timely treatment. Additionally,
family support also helps in overcoming psychological stress and
provides positive reinforcement about knowledge, awareness,
and practices regarding patients suffering from CLP [9].
Given the importance of the mother’s role in preventing and
possibly providing the right treatment for the child with CLP, knowledge, and awareness of mothers should be of paramount
importance. Alcohol consumption, lack of essential minerals,
diabetes, and exposure to radiation during pregnancy has been
known to be detrimental to the developing fetus, with Cleft lip
and palate being one of the possible anomalies a newborn might
be born with. Before a child is born, current modern enhance-
ments offer the parents to view some developmental abnor-
malities beforehand, with Cleft lip and palate being one of them.
Although it is possible to detect antenatally Cleft lip and palate,
a fetus with an isolated cleft palate cannot be detected before
birth [10]. With the right information, parents may be prepared
beforehand for the child which may be born with this pathology
and the additional needs the child may require [11]. Although CLP
is a readily managed anomaly, some parents do opt for termina-
tion when being informed of the antenatal diagnosis. This is again
mainly due to improper or lack of knowledge regarding CLP.
In this study, we aim to evaluate the general population’s
knowledge, awareness, and practices regarding patients being
born with Cleft lip and palate. Moreover, the impact of age, gen-
der, level of education, and occupation on knowledge, awareness,
and practices is also being assessed.
Methods and materials
In this cross-sectional survey-based study, we recruited a to-
tal of 505 participants using a convenience sampling method.
The study was carried out from August 2020 to August 2021. The
sample consisted of participants belonging to all age groups, visit-
ing the Fatima Memorial Hospital, Pakistan for oral-health related
concerns. A prevalidated questionnaire was used which consisted
of 4 parts: 1) questions about demographic data, 2) questions
about knowledge of Cleft lip and palate, 3) questions assessing
awareness levels of cleft lip and palate, and 4) questions deter-
mining practices followed regarding cleft lip and palate. To ensure
voluntary participation in this study, a consent statement was in-
cluded and then the response was recorded.
Firstly, in our study, we evaluated the knowledge levels of the
participants regarding cleft lip and palate through various ques-
tions such as understanding about cleft lip and palate, source of
information on CLP, risk factors associated, etiological factors, the
effect of gender, and complications which a child may develop
if left untreated. Secondly, awareness levels were assessed by
asking questions regarding treatment options available for cleft
lip and palate patients, the right time for treatment, the correct
initial treatment option, the possibility of antenatal diagnosis,
doctors to consult, and the association of family history. Lastly,
practices being followed were determined by asking questions re-
garding care required during pregnancy such as which foods and
medicines should and should not be consumed, social habits e.g.
smoking and alcohol, maternal diabetes, consulting a doctor for
treatment, and the importance of adulthood treatment of Cleft
lip and palate.
Participation in this study was primarily based on the general
population belonging to all age groups who visited the respec-
tive hospital for concerns related to oral health. Those who were
not able to read and write were excluded from this study. The
data that was gathered from this survey was kept anonymous and
confidential. The ethical approval was approved by the Fatima
Memorial Hospital. For Data analysis, SPSS statistical software version 25 was used. Descriptive statistics along with Spearman’s
correlation tests were used to analyze any significant relationship
between age, gender, level of education, and occupation with lev-
els of knowledge, awareness, and practices. A p-value of <0.05
was considered statistically significant.
Results
In this study, we received a total of 570 filled questionnaires,
out of which 65 were excluded based on being either incomplete-
ly filled or being of irrelevance. A total of 505 participant ques-
tionnaires were included in this study. The response rate was cal-
culated to be 88.6%. A strong relation of 0.85 was found between
the items used in this questionnaire using intraclass correlation.
Descriptive statistics along with Spearman’s correlation tests were
used to analyze any significant relationship between age, gender,
level of education, and occupation with levels of knowledge,
awareness, and practices of the participants regarding cleft lip
and palate.
Out of the 505 participants, 194 (38.4%) were males and 311
(61.6%) were females. The majority of 292 (57.8%) participants
belonged to the age bracket of 18-30 years with a minority of
18 (3.6%) being in the 51-60 years age group. Predominantly,
166 (32.9%) participants had undergraduate education and 181
(35.8%) had a graduate education. Regarding the current occu-
pation, 176 (34.9%) students, 155 (30.7%) healthcare profession-
als, and 62 (12.3%) businesses were the most commonly selected
ones as shown in Table 1.
Table 1: Clinicopathological characteristics of PEACs in compari-
son with MCC.
|
Variables |
N |
% |
| Age |
Below 18 years |
39 |
7.7 |
| 18-30 years |
292 |
57.8 |
| 31-40 years |
99 |
19.6 |
| 41-50 years |
37 |
7.3 |
| 51-60 years |
18 |
3.6 |
| Above 60 years |
20 |
4.0 |
| Gender |
Male |
194 |
38.4 |
| Female |
311 |
61.6 |
| Education |
Undergraduate |
166 |
32.9 |
| Graduate |
181 |
35.8 |
| Postgraduate |
130 |
25.7 |
| Below graduate |
28 |
5.5 |
| Occupation |
Student |
176 |
34.9 |
| Business |
62 |
12.3 |
| Healthcare Professional |
155 |
30.7 |
| Engineer |
29 |
5.7 |
| Teacher |
32 |
6.3 |
| Unemployed |
21 |
4.2 |
| Others |
30 |
5.9 |
Regarding knowledge, the majority of 413 (81.8%) participants
had heard previously about cleft lip and palate, with healthcare
professionals being the most common source of information for
151 (29.9%) participants along with friends and family and social
media. A few 45 (8.9%) participants had never heard about cleft
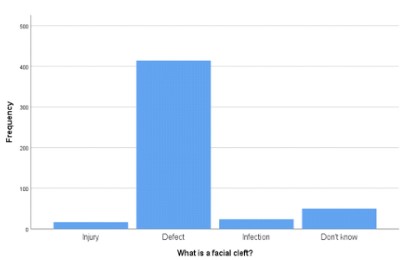
lip and palate. When describing a facial cleft, 82% (414 out of 505)
participants believed that a cleft is a defect with a few 9.9% (50
out of 505) not able to describe it, as shown in figure 1. Regarding the etiology, most of the 372 (73.7%) participants believed that
genetics caused cleft lip and palate, along with some selecting
medicines (29.7%), autoimmune (20.4%), and alcohol (20.4%) as
additional causes. Regarding risk factors about a child being born
with cleft lip and palate, predominantly, 51.9% (262 out of 505)
believed maternal smoking, maternal diabetes, family history,
medicines, and radiation as possible risk factors. A majority of
56.4% (285 out of 505) respondents said that child born with cleft
lip and palate faces difficulties in speech, hearing, and feeding.
The majority of 412 (81.6%) participants answered cleft lip and
palate occur both in males and females. More than half of 270
(53.5%) participants believed cleft lip and palate do not always
occur together. About 202 (40%) answered that cleft lip and pal-
ate accompany other abnormalities as well with 27.1% (137 out
of 505) disagreeing with it.
Regarding awareness, the majority of 384 (76%) participants
said cleft lip and palate are not contagious. Most of the 297
(58.8%) participants had never come across a patient suffering
from cleft lip and palate. 396 (78.4%) participants agreed that
treatment options are available for cleft lip and palate patients.
About 61.6% (311 out of 505) participants responded “No” to
cleft lip and palate being a burden to the parents with some 23%
(116 out of 505) considering it a burden. 250 (49.5%) participants
believed enough doctors are available to treat such patients, with
the majority 80.4% (406 out of 505) agreeing on surgery was the
best and first choice of treatment (73.3%). Regarding the best
time for treatment, 73.3% (370 out of 505) participants believed
infancy was the best time to start the treatment. A majority of 249
(49.3%) participants believed that cleft lip and palate can be diag-
nosed before birth. A majority of 167 (33.1%) respondents said
pediatricians should be the first doctor to consult when a child is
born with cleft lip and palate. Predominantly, 230 (45.5%) partici-
pants answered “Yes” to if one child or parent has CLP, it increases
the risk of another child also having it.
Regarding practices, 459 (90.9%) participants strongly agreed
that a healthy diet is important during pregnancy for newborns’
health. A majority of 422 (83.5%) respondents believed that
smoking cessation is important during pregnancy along with the
cessation of alcohol (83%). For pregnant women with diabetes,
the majority of 378 (74.9) said their blood sugar levels should be
controlled. Furthermore, unnecessary medicines should also not
be given to expecting mothers (90.5%). The majority of 91.5%
(462 out of 505) participants believed immediate doctor consul-
tation for a child with CLP. Predominantly, 311 (61.6%) did not attend an informative seminar on CLP. The majority of 90.9% (459
out of 505) participants believed gynecologist consultation to be
important for pregnant females. Regarding vitamins and mineral
intake, 464 (91.9%) participants agreed to be part of a healthy
diet during pregnancy. Regarding adult CLP treatment, 79.2% of
participants think they should be offered treatment, but speech
(62.6%) was the most commonly selected option which could not
be corrected during adult CLP treatment as shown in Figure 2.
Spearman’s correlation test was used to analyze any signifi-
cant relationship between age, gender, education, and occupa-
tion with knowledge, awareness, and practices regarding cleft lip
and palate. A significant relation was found between Knowledge
with age (p-value=0.01) and Education (p-value=0.001) and Prac-
tices with gender (p-value=0.01) and education (p-value=0.049)
as shown in table 2. No significant relation was found among the
other remaining variables.
Table 1: Correlation of knowledge, awareness, and practices with predictor variables.
| Parameters |
Correlations |
Age |
Gender |
Education |
Occupation |
Knowledge |
Awareness |
Practice |
| Age |
Correlation |
1 |
-0.139 |
0.409 |
0.372 |
0.109 |
-0.055 |
-0.063 |
| Sig. (2-tailed) |
|
0.002 |
0 |
0 |
0.014 |
0.216 |
0.156 |
| Gender |
Correlation |
-0.139 |
1 |
-0.017 |
0.087 |
0.027 |
-0.004 |
-0.108 |
| Sig. (2-tailed) |
0.002 |
|
0.711 |
0.05 |
|
0.928 |
0.015 |
| Education |
Correlation |
0.51 |
-0.115 |
1 |
|
0.039 |
0.086 |
0.044 |
| Sig. (2-tailed) |
0 |
0.022 |
|
0 |
0.44 |
0.85 |
0.382 |
| Occupation |
Correlation |
0.372 |
0.087 |
0.542 |
1 |
0.061 |
0.03 |
-0.02 |
| Sig. (2-tailed) |
0 |
0.05 |
0 |
|
0.17 |
0.499 |
0.652 |
| Knowledge |
Correlation |
0.109 |
0.027 |
0.148 |
0.061 |
1 |
0.289 |
0.092 |
| Sig. (2-tailed) |
0.014 |
0.542 |
0.001 |
0.17 |
|
0 |
0.039 |
| Awareness |
Correlation |
-0.055 |
-0.004 |
0.059 |
0.03 |
0.289 |
1 |
0.391 |
| Sig. (2-tailed) |
0.216 |
0.982 |
0.183 |
0.499 |
0 |
|
0 |
| Practice |
Correlation |
-0.063 |
-0.108 |
0.088 |
-0.02 |
0.092 |
0.391 |
1 |
| Sig. (2-tailed) |
0.156 |
0.015 |
0.049 |
652 |
0.039 |
0 |
|
Discussion
In this study, we assessed the knowledge, awareness, and
practices of the general population regarding cleft lip and palate.
To some extent, CLP is preventable, and if a child is born with it,
timely surgical treatment can return the child to normalcy and sat-
isfactory quality of life [12]. So, adequate knowledge, awareness,
and practice regarding CLP are of paramount importance. Fur-
thermore, an increased positive perception of CLP will be indeed
beneficial for the child with CLP to promote a better quality of life.
In our study, females were more aware of CLP as compared
to males. Furthermore, the majority of the participants were in
general aware of CLP. This is not surprising as the study was car-
ried out in locations where people mainly belong to good socio-
economic status. Poor knowledge about CLP has been reported in
previous studies in rural and urban Asia [13,14]. In general, high
knowledge levels were reported in our study (81.8%), these re-
sults contrast with previously carried out studies [15] where more
than half of participants did not hear about CLP, suggesting the
need to implement public health sessions to increase knowledge
about CLP.
A study by Owotade et al, concludes that more than 50% of the
females were unaware of CLP and that a similar percentage didn’t
participate in any public health program to enhance CLP knowl-
edge. Moreover, the more educated an individual was, the better
the knowledge about CLP [16]. Similar trends were also reported
in our study.
In terms of describing what a facial cleft looks like, most of
the participants in our sample described it as a “defect” of the
lip and palate. Furthermore, many understood that cleft lip and
palate can present as isolated deformities. Results of our study
as consistent with Owatade et al, the majority selected CLP as a
defect [16]. On the other hand, Middleton et al concluded that
the general population was not able to define a cleft (18.4%) [15].
Possible reasons for this could be lack of proper education, poor
socioeconomic status, and the way the questions might be asked
of the participants.
Regarding the cause of CLP, mostly the participants were aware
of it because of genetics, consumption of medicines, and alcohol.
Literature states, increased levels of cortisol, which is a cortico-
steroid, released during stress could increase the risk of the development of orofacial clefts [5]. Few participants (20%) in our
study select corticosteroids as a potential cause of CLP but further
research is mandated to figure out the possible relation. More-
over, diabetes, alcohol consumption, and family history were
possible risk factors for CLP. Kozma et al concur that uncontrolled
diabetes during pregnancy leads to increased chances of orofacial
cleft along with alcohol being a possible risk factor too [17]. Some
studies report self-perceived causes of CLP including exposure to
an eclipse, and black magic [18]. No relevancy has been stated of
these causes in the medical sciences, these are just self-perceived
causes with no supporting evidence.
A child being born with CLP may face difficulties with speech,
hearing, feeding, and dentition along with the psychosocial im-
pact of it. Most of the participants in this study were aware of
these problems. These results correspond with a similar study car-
ried out by Nujaim et al [19]. Surgery is the best treatment for a
child with CLP. This statement was agreed upon in our study along
with previous studies in the literature [15]. This surgical treatment
is most commonly offered by plastic and maxillofacial surgeons.
Some aspects of the treatment mandate the involvement of phy-
sicians from other specialties. So, in general, the treatment of CLP
is offered in a multi-disciplinary approach with a team of doctors.
Most of the participants in our study were not aware of the ap-
proach, and selected doctors of individual specialties.
Being born with cleft lip and palate in children has been associ-
ated with a deficiency of folic acid in pregnant females [20]. This
has been emphasized in our study, where many participants agree
on taking multivitamins as part of their diet during pregnancy.
A recent trend has been of encouragement of pregnant fe-
males to visit their gynecologist to keep their and yet to be born
child’s health to the best [21]. Due to this, knowledge of CLP is
primarily disseminated by doctors, as seen in our study. Further-
more, the diagnosis of CLP can be made before the birth of the
child. If it is present, this gives the parents an adequate amount
of time and counseling about the increased requirements of the
child being born with CLP.
Adults being untreated CLP during their childhood meet with
increased risks along with being unable to restore certain func-
tions to normalcy. In our study, speech was the most commonly
selected function to be impaired even after the treatment of CLP
during adulthood. This is supported by previous studies which not
only conclude impairment of speech even after treatment but the
imperfect nasolabial appearance was also found [22]. But offer-
ing treatment to adults remains beneficial to a great extent with
significant improvements in quality of life.
We evaluated the knowledge, awareness, and practices of
the general population regarding cleft lip and palate comprehen-
sively using validated tools. In this study despite the mentioned
strengths, we were met with a few limitations. Firstly, the sample
consisted of individuals mostly from the urban population with
good socioeconomic status. Lastly, the inclusion of pregnant fe-
males could be further beneficial to increase the scope of this
study.
Conclusion
In conclusion, the general population which was surveyed
showed adequate knowledge and awareness of cleft lip and palate with a supportive and positive attitude. Education plays an
important part in understanding CLP as a condition that is to an
extent preventable and treatable to near normalcy. To further in-
crease knowledge about CLP, awareness programs through public
healthcare programs regarding risk factors, diagnosis, causes, and
multidisciplinary treatment can be beneficial.
Declarations
Acknowledgments: The authors would like to thank all the
participants that were involved in this study.
Disclaimer: None.
Conflict of Interest: None.
Funding disclosure: None.
References
- Noorollahian M, Nematy M, Dolatian A, Ghesmati H, Akhlaghi S, et
al. Cleft lip and palate and related factors: A 10 years study in uni-
versity hospitalised patients at Mashhad - Iran. African J Paediatr
Surg. 2015; 12: 286.
- Kasatwar A, Borle R, Bhola NKR, Prasad GSV, Jadhav A. Prevalence
of congenital cardiac anomalies in patients with cleft lip and palate
– Its implications in surgical management. J Oral Biol Craniofacial
Res. 2018; 8: 241-244.
- Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate:
understanding genetic and environmental influences. Nat Rev
Genet. 2011; 12: 167-178.
- Elahi MM, Jackson IT, Elahi O, Khan AH, Mubarak F, et al. Epidemi-
ology of Cleft Lip and Cleft Palate in Pakistan. Plast Reconstr Surg.
2004; 113: 1548-1555.
- Burg ML, Chai Y, Yao CA, Magee W, Figueiredo JC. Epidemiology,
Etiology, and Treatment of Isolated Cleft Palate. Front Physiol.
2016; 7.
- Yaqoob M, Mahmood F, Hanif G, Bugvi S, Sheikh M. Etiology and
genetic factors in clefts of lip and/or palate reported at children′s
hospital, Lahore, Pakistan. Indian J Hum Genet. 2013; 19: 136.
- Shaw W, Semb G, Lohmander A, Persson C, Willadsen E, et al. Tim-
ing Of Primary Surgery for cleft palate (TOPS): protocol for a ran-
domised trial of palate surgery at 6 months versus 12 months of
age. BMJ Open. 2019; 9: e029780.
- Alazzawi O, Morioka D, Miyabe M, Tosa Y, Ohkubo F, et al. Naso-
labial Growth in Individuals With Unilateral Cleft Lip and Palate. J
Craniofac Surg. 2017; 28: e449-451.
- Shkoukani MA, Chen M, Vong A. Cleft Lip -A Comprehensive Re-
view. Front Pediatr. 20131.
- Gillham JC, Anand S, Bullen PJ. Antenatal detection of cleft lip with
or without cleft palate: incidence of associated chromosomal and
structural anomalies. Ultrasound Obstet Gynecol. 2009; 34: 410-
415.
- Nahai FR, Williams JK, Burstein FD, Martin J, Thomas J. The Man-
agement of Cleft Lip and Palate: Pathways for Treatment and Lon-
gitudinal Assessment. Semin Plast Surg. 2005; 19: 275-285.
- LOPES JFS, PINTO JHN, LOPES MMW, MAZOTTINI R, SOARES S. In-
terrelationship between implant and orthognathic surgery for the
rehabilitation of edentulous cleft palate patients: a case report. J Appl Oral Sci. 2015; 23: 224-229.
- Weatherley-White RCA, Eiserman W, Beddoe M, Vanderberg R.
Perceptions, Expectations, and Reactions to Cleft Lip and Palate
Surgery in Native Populations: A Pilot Study in Rural India. Cleft
Palate-Craniofacial J. 2005; 42: 560-564.
- Chan RKK, McPherson B, Whitehill TL. Chinese Attitudes toward
Cleft Lip and Palate: Effects of Personal Contact. Cleft Palate-Cra-
niofacial J. 2006; 43: 731-739.
- Middleton GF, Lass NJ, Starr P, Pannbacker M. Survey of public
awareness and knowledge of cleft palate. Cleft Palate J. 186AD; 23.
- Owotade F, Ogundipe O, Ugboko V, Okoje V, Olasoji, et al. Aware-
ness, knowledge and attitude on cleft lip and palate among ante-
natal clinic attendees of tertiary hospitals in Nigeria. Niger J Clin
Pract. 2014; 17: 6.
- Kozma A. Gestational Diabetes Mellitus and the Development of
Cleft Lip / Palate in Newborns. Acta Endocrinol. 2019; 15: 118-122
- Chung KY, Sorouri K, Wang L, Suryavanshi T, Fisher D. The Impact
of Social Stigma for Children with Cleft Lip and/or Palate in Low-
resource Areas. Plast Reconstr Surg - Glob Open. 2019; 7: e2487.
- Alnujaim NH, Albedaie ES, Alyahya LS, Adosary MA, Alotaibi FF, et
al. Awareness, knowledge and attitudes of Saudi pregnant women
towards cleft lip and palate. Curr Pediatr Res. 2017; 21: 595-603.
- Houston M. Taking folic acid at start of pregnancy seems to low-
er risk of cleft lip and palate. BMJ [Internet]. 2012; 345: e4614–
e4614.
- Carter EB, Tuuli MG, Caughey AB, Odibo AO, Macones GA, et al.
Number of prenatal visits and pregnancy outcomes in low-risk
women. J Perinatol. 2016; 36: 178-181.
- Murthy J. Management of cleft lip and palate in adults. Indian J
Plast Surg. 2009; 42: 116.