Introduction
HELLP syndrome (hemolysis, elevated liver blood tests and low
platelets) is a serious complication in pregnancy characterized by
hemolysis, elevated liver enzymes and low platelet count occurring in 0.2 to 0.6% of all pregnancies and in 10-20% of cases with
severe preeclampsia. Spontaneous hepatic capsular rupture is a
rare (0,015% of all pregnancies), but a life-threatening complication of HELLP syndrome with a mortality rate of up 50% for both
mother and infant. The clinical presentation of hepatic hematoma
is generally non-specific and may include right upper quadrant or
epigastric pain and vomiting. A high index of suspicion and prompt
recognition allows a multidisciplinary approach and mortality can
be reduced.
We present the case of a 34-year-old nulliparous woman with
a second trimester gestational hepatic rupture associated with
HELLP syndrome. We discuss the aetiology and treatment options
involving this rare presentation.
Case description
A 34-year-old nulliparous woman, with no history of relevant
medical conditions, was referred to the delivery room at 28 weeks
of gestation complaining of 3 hour severe abdominal pain localized to the right upper quadrant. Her blood pressure was 160/115
mmhg. No data on arterial hypertension during pregnancy. Proteinuria 1000 mg/dL in urine test. Pre-eclampsia was diagnoses.
The tracing on the fetal heart monitor indicated pathological fetal
distress. In light of these findings she underwent an emergency
caesarean section.
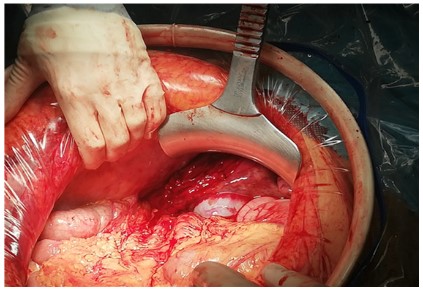
When entering in abdominal cavity a 1000 mL hemoperitoneum was detected. Hysterotomy was done and a 28 weeks alive
fetus was obtained. It was subsequently conversed to median
laparotomy. A subcapsular hepatic hematoma involving the entire
right lobe was found with hepatic rupture of segments V and VI
and active hemorrhage (Figure 1). Subdiafragmatic and hepatic
packing was performed with eleven gauze pads placed above and
around the liver in a routine manner. Finally a negative pressure
open abdomen was performed. During surgery, the diagnosis of
HELLP syndrome was confirmed with laboratory findings (hemoglobin 8.3 g/dL, platelets 66,000 mm3, AST 1404, ALT 770).
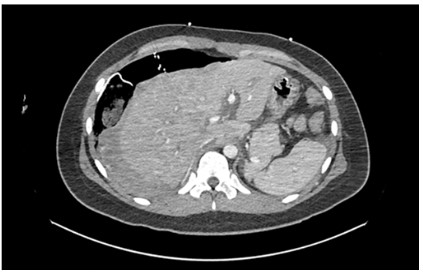
After hemodynamic stabilization of the patient an abdominal
CT angiography was done confirming hepatic subcapsular and parenchymal hematoma, with multiple foci of active venous bleeding in the area of the hepatic dome and right hepatic lobe (Figure B).
The patient was admitted to ICU where aggressive management with fluid therapy was continued. Renal and respiratory
function were preserved and treatment with broad-spectrum antibiotics was initiated due of febrile peaks.
A second-look surgery was performed 72 hours later, in which
the packing was removed and a large organized subcapsular hematoma was observed involving the right hepatic lobe, with the
left lobe appearing normal. Cholecystectomy was performed due
to the presence of cholelithiasis to avoid ischemic/infectious complications during the postoperative period. There were no signs
of active bleeding, so primary abdominal wall closure was performed.
The patient presented a satisfactory postoperative evolution
with progressive improvement of the distributive shock. During
her admission she required a total of two units of packed red
blood cells and three units of fresh frozen plasma. In the immediate postoperative she presented amnesia and pregnancy denial.
A cranial CT scan was performed with normal findings. Progressive recovery of platelet and liver enzyme levels (Table A), until
normalization and resolution of her confusional syndrome. The
patient was discharged on 18 postoperative day (POD).
Discussion
Spontaneous hepatic rupture is an infrequent but life-threatening condition of pregnancy associated with severe pre-eclampsia. Pre-eclampsia is defined as elevated blood pressure (>160/90
mmHg) with proteinuria (dipstick reading >1+ or >0,3 g of protein
in a 24-hour urine) after 20 weeks of pregnancy or after delivery.
It occurs in 8% of all pregnancies, and 10-15% of cases may be
complicated by Hemolysis, Elevated Liver Enzymes and Low Platelet Count (HELLP) syndrome [1]. HELLP syndrome was first defined
by Weinstein in 1982 [2]. It is a multisystemic disorder that carries significant maternal and perinatal morbidity and mortality.
This syndrome has an incidence of 0,17 to 0,85% of all pregnancies, whereas the risk of recurrence in a subsequent pregnancy is
about 19 to 27%. The incidence of spontaneous hepatic rupture
is reported to be between 1 case in 45,000-225,000 pregnancies
and only 1-2% of all of them in the context of HELLP syndrome [3].
The pathophysiology of HELLP syndrome is not well understood. The origin of preeclampsia/HELLP can be attributed to
defective trophoblastic invasion that leads in a deficient placentation. All this induces a generalized vasoconstriction state secondary to dysfunction in the vascular epithelium, rather than the
vasodilation typical of normal pregnancy. All this is manifested by
an imbalance between vasodilator prostaglandins (prostacyclins)
versus vasoconstrictors (thromboxanes) that generates an excess
production of proinflammatory cytokines (IL-2, TNF) causing endothelial damage. Vasospasm produces a reduction in plasma
volume leading to hemoconcentration and hypercoagulability. All
this leads to multi-organ hypoperfusion that worsens the maternal and fetal condition [4]. A periportal hemorrhage and intravascular fibrin aggregation in the liver cause sinusoidal obstruction,
intrahepatic vascular congestion, increased liver pressure, hepatic necrosis and intraparenchymal and subcapsular hemorrhage,
which may result in capsular rupture [5].
Henny et al. described a series of 75 patients where hematomas are more frequent in the right hepatic lobe (75% of cases),
compared to the left hepatic lobe (11%) or both (14%). In our patient the hematoma involved the right hepatic lobe, like the majority described [6].
The most common clinical sings of hepatic hematoma are right
upper quadrant pain and/or epigastric pain (70-90%), right shoulder pain, right lung base hypoventilation, nausea and vomiting.
These symptoms are supposed to be caused by the stretching of
Glisson’s capsule. Liver rupture is manifested as massive hypovolemic shock and abdominal distention. Most liver related complications of HELLP syndrome occur during the third trimester as in
our case, late in the second trimester and also a few cases have
been reported in literature during the immediate postpartum period [3].
Diagnosis is based on clinical suspicion and laboratory evidence
of severe anemia, elevated liver enzymes and thrombocytopenia
[7]. Abdominal CT with intravenous contrast is considered to be
the best diagnostic method, being more sensitive than abdominal
ultrasound. Nuclear magnetic resonance is also useful for surveillance of chronic hematomas [8]. In our case no imagen test was
needed because the blood in abdominal cavity was observed during the emergency caesarean section.
The management of this pathology requires a multidisciplinary
approach between gynecologists, general surgeons and intensive
care physicians. The main therapeutic objectives are: eliminate
the causal factor, end the pregnancy (emergency caesarian section) and control hemorrhage (exploratory laparotomy). Hemodynamic stabilization with aggressive volume resuscitation and
blood products represents a fundamental point of early support
[9]. If there is not hepatic rupture and the patient is hemodynamically stable, conservative nonoperative management for selected
patients has been recommended consisting on close monitoring
of the patient and imaging test controls [9,10]. However, if the patient presents hemodynamic instability despite adequate resuscitation or hemoperitoneum, it has been seen that surgery significantly reduces the mortality associated with this pathology [7,10].
In the cases of hepatic rupture, achieving liver hemostasis
though surgery is difficult because of the presence of multiple
areas that are affected by infraction and hematomas and especially because of coagulopathy. Surgical management of these patients must follow the same principles as damage control surgery.
Multiple surgical options have been described: hemostasis with
specific devices, hepatorrhaphy, vessels ligation, hepatic artery
ligation, collagen sponges, argon laser and perihepatic packing
followed by a second-look surgery [3]. Transcatheter Arterial Embolization (TAE) is a well-recognized treatment method that can
be performed as an alternative or as a complement to surgery.
In-Chul Nam et al. described that TAE is useful and less invasive
than other techniques and recommended it as a bridge between
perihepatic packing and hepatectomy if necessary [5]. The use of
hemostatic meshes has also been described, which have demonstrated their effectiveness in managing ruptured hematomas,
with less need for reinterventions [11]. In case of massive hematoma or necrosis of the hepatic parenchyma, partial hepatectomy
or liver transplantation may be necessary.
In our reported case, the diagnosis was intraoperative during cesarean section and liver packing was performed due to the
extensive capsular rupture in the liver, making it impossible to
achieve hemostasis in any other effective way. A CT angiography
was performed to assess possible arterial bleeding that could be
embolized, but this was not confirmed. A second-look laparotomy
was performed 72 hours later, verifying resolution of the bleeding
with the initial packing.
Conclusion
Hepatic subcapsular hematoma and hepatic rupture are infrequent but life-threatening complications that can occur during
pregnancy and are fundamentally related to pathologies such as
preeclampsia and HELLP syndrome. The first step is to end the
pregnancy and subsequently control the acute liver problem. Different surgical techniques have been described that should be
individualized for each patient according to damage control principles. A high index of suspicion and prompt recognition allows a
multidisciplinary approach and mortality can be reduced
Conflict of interest: The authors declare no conflict of interest.
References
- Vigil-De Gracia P, Ortega-Paz L. Pre-eclampsia/eclampsia and hepatic rupture. Int J Gynaecol Obstet. 2012; 118: 186-189.
- Weinstein L. Syndrome of hemolysis, elevated liver en- zymes and
low platelet count: a severe consequence of hypertension in pregnancy. Am J Obstet Gynecol. 1982; 142: 159-167.
- Pavlis T, Aloizos S, Aravosita P, Mystakelli C, Petrochilou D, et al. Diagnosis and surgical management of spontaneous hepatic rupture
associated with HELLP syndrome. J Surg Educ. 2009; 66: 163-167.
- Cararach V, Botet F. Preeclampsia. Eclampsia y Síndrome HELLP.
Protocolos diagnóstico terapéuticos de la AEP: Neonatología. Barcelona, 2008.
- Nam IC, Won JH, Kim S, et al. Transcatheter Arterial Embolization
for Spontaneous Hepatic Rupture Associated with HELLP Syndrome: A Case Report. Medicina (Kaunas). 2021; 57: 1055.
- Henny CH, Henny CP, Lim TE, Brummelkamp WH, Büller HR, et al.
Spontaneous rupture of the Glisson’s capsule during pregnancy:
an acute surgical emergency. Neth J Surg. 1992; 34: 72-75.
- Escobar Vidarte M, Montes D, Pérez A, Loaiza-Osorio S, José Nieto
Calvache A, et al. Hepatic rupture associated with preeclampsia,
report of three cases and literature review. J Matern Fetal Neonatal Med. 2018; 32: 2767-2773.
- Barton JR, Sibai BM. Hepatic imaging in HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count). Am J Obstet
Gynecol. 1996; 174: 1820-1825.
- González EY, Ávila EJF. Morbimortalidad materna asociada a ruptura hepática o hematoma subcapsular por preeclampsia-eclampsia y síndrome HELLP. Arch Inv Mat Inf. 2010; 2: 51-55.
- Moura C, Amaral L, Mendes J. Liver rupture in HELLP syndrome. J
Surg Case Rep. 2019; 10: 1-3.
- Ramírez Cabrera J, Campos Siccha G, Zapata Díaz B, et al. Hepatic
rupture in HELLP syndrome: electrofulguration and use of mesh.
Rev peru ginecol obstet. 2019; 65: 537-540.