Introduction
Forefoot deformities are relatively common in patients with
rheumatoid arthritis (RA). In particular, the prevalence of deformities increases in poorly controlled cases with medium- to longterm disease duration [1]. Hallux valgus, hammer toe, claw toe of
the 2nd -4th toes, digitus varus minimi, and flat foot deformity
are characteristic deformities of patients with RA [2,3]. In hammer toe, flexion of the proximal interphalangeal (PIP) joint causes
dorsal friction by the shoe, resulting in pain and ulceration. In addition, hyperextension of the Metatarsophalangeal (MTP) joint
may cause the metatarsal heads to deviate to the plantar side,
resulting in painful calluses.
Surgical procedures for hammer toes include flexor digitorum
longus tendon transfer [4], shortening osteotomy of the proximal
phalanx neck [5], PIP joint arthrodesis [6], and metatarsal shortening osteotomy [7]. Fixation methods for the PIP joint include
K-wire or headless screw insertion through the distal phalanx and
insertion of an intramedullary implant, either a single-device type
or a dual-component type implant. The dual-component type is
an interlocking mechanism after insertion of the implant into the
metaphyseal and basal phalanges, which simplifies the intraoperative procedure compared to the single-device type intramedullary implant.
We have reported that foot surgery is a risk factor for postoperative infection in RA patients [8]. PIP joint fusion with K-wire
fixation increases the infection rate because of the need for wires
protruding at the toe end. Implantable devices are preferrable.
Not only the hammer toe but also the hallux valgus and digitus
varus minimi need to be corrected, which increases operative
time. Shortening the operative time is also important to decrease
the infection rate.
The Nextra® Hammertoe Correction System (Zimmer-Biomet,
Warsaw, Indiana, USA) is the industry’s only adjustable, two-piece, hammer toe solution. The advantage of this implant is its
stability, versatility, and anatomic design. It was designed to maximize bone purchase, stabilize and secure the phalanx, and optimize screw design for repeatable outcomes [6]. The two-piece design with the RevLock® Adjustable Locking Mechanism provides
intermediate locking before final closure and allows for retained
compression. The anatomically correct design with 10 degrees of
angulation restores the natural state (Figure 1a).
To the best of our knowledge, the clinical and radiographic results of PIP joint arthrodesis by this dual-component intramedullary implant for RA forefoot deformity have not been reported.
Thus, the clinical and radiographic outcomes of this implant for
hammer toe deformity in patients with RA were investigated.
Materials and methods
Participants
This was a retrospective, observational study to analyze the
clinical and radiographic outcomes of a dual-component intramedullary implant for hammer toe deformity inpatients with RA.
A total of 11 consecutive toes in six patients were treated with the
Nextra® Hammertoe Correction System between April 2019 and
May 2022 and followed-up for at least six months. The research
period of this study was between April 2019 and November 2022.
All surgeries were performed by one senior surgeon who was a
specialist in foot and ankle surgery at one hospital. The inclusion
criteria were as follows: (1) hammer toe deformity; (2) claw toe
deformity; or (3) overlapping toe by rheumatoid forefoot. The
exclusion criteria were the presence of infection or peripheral
vascular disease. Patients stopped biological or targeted synthetic
Disease-Modifying Anti-Rheumatic Drugs (DMARDs) and continued conventional synthetic DMARDs during the perioperative period.
In accordance with the Declaration of Helsinki, written, informed consent for participation in the study was obtained from
all participants. This study protocol was approved by the institutional review committee of the hospital.
The patients’ baseline demographic characteristics are shown
in Table 1. The mean age at surgery was 62.6 ± 6.0 (range, 58-72)
years, and the mean follow-up duration was 21.0 ± 15.2 (range,
6-43) months. The mean disease duration was 22.7 ± 10.5 years,
and most patients had established RA. The Disease Activity Score
(DAS) composite of the erythrocyte sedimentation rate (ESR) and
the 28-joint score (DAS28-ESR) [9] was 3.38 ± 0.43, and many patients showed moderate disease activity. The Steinbrocker stage
and class were relatively high, and the median modified health
assessment questionnaire score was 0.625. Patients were treated
with methotrexate (66.7%) and biological or targeted synthetic
DMARDs (50%). Two-thirds of the patients were on glucocorticoids, with an average prednisone equivalent dosage of 3.2 ± 1.3
mg There were no untreated patients. The Larsen grade was 4 and
5 in two and four patients, respectively.
Surgical technique and postoperative procedure
All implants were the dual-component type intramedullary device (Nextra® Hammertoe Correction System). PIP joint arthrodesis was performed through a dorsal longitudinal incision, and the
extensor tendon was cut at the base of the middle phalanx. The
proximal phalanx was osteotomized perpendicular to the plantar surface, and the middle phalanx was osteotomized in plantar flexion of 5 to 10 degrees. A stem hole was reamed at the
proximal and middle phalanges, and the implants were fixed with
a screwed-in system at each bone. Each implant was connected
and confirmed to be locked (Figure 1b). When a gap developed
between the bones, bone grafting was performed. The extensor
tendon was sutured, and the skin was closed. All surgeries were
performed simultaneously with resection arthroplasty (LeLievre
method) [10] or joint preservation surgery [11] of the MTP joint.
The forefoot was dressed bulky, and the patients wore orthotics for forefoot unloading to weight-bearing on their heel from
one day until two weeks postoperatively. The patients were
changed to a functional insole and kept weight-bearing on their
heels for eight weeks. Passive range of motion exercises of the
ankle joint and toes were permitted from the day after surgery.
Assessment of clinical outcomes
Clinical outcomes at the preoperative, postoperative, and final follow-up visits were evaluated using the Japanese Society for
Surgery of the Foot (JSSF) lesser scale [12] and the self-administered foot-evaluation questionnaire (SAFE-Q) score [13]. Patient
satisfaction was evaluated after surgery and at final follow-up by
a visual analog scale (worst: 0 point, best: 10 points). Complications, including delayed wound healing, intraoperative fracture,
superficial infection, deep infection, and implant removal were
assessed and counted.
Assessment of radiographic parameters
Anteroposterior and lateral radiographs of each lesser toe were
taken at the preoperative visit and at each follow-up visit. The
radiographs were performed in the no-weight-bearing position.
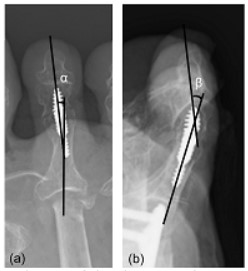
The alignment of the PIP joint was defined as the angle between
the long axis of the proximal phalanx and the middle phalanx on
both anteroposterior (Figure 2a: α angle) and lateral radiographs
(Figure 2b: β angle). In the anteroposterior position, varus was
defined as + and valgus as -. In the lateral position, flexion was
defined as + and extension as –. Bone fusion of the PIP joint was
evaluated at the preoperative visit and at each follow-up visit.
Statistical analysis
Continuous data are presented as means ± standard deviation (SD) for data with a normal distribution or as medians (25th,
75th percentiles) for data not normally distributed. The JSSF
scale, SAFE-Q score, and radiographic parameters (α angle and β
angle) at pre-operation, post-operation, and final follow-up were
compared by the Freidman signed-rank test, with the Bonferroni
correction. All statistical tests were two-tailed, and values of p <
0.05 were considered significant. All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM, Armonk, NY,
USA).
Results
Clinical outcomes
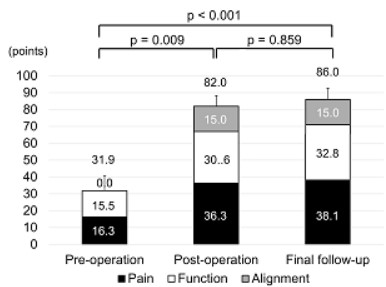
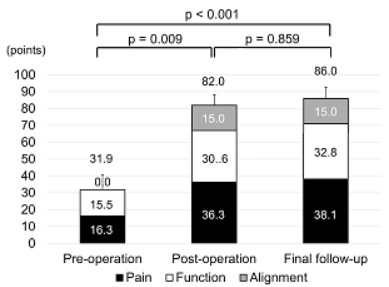
The preoperative total JSSF lesser score and subcategory scores
were low, as shown in Table 1 and Figure 3. Significant improvements in the total JSSF lesser score and all component scores were
seen between pre-operation and post-operation (total score: 31.9
± 9.0 points vs 82.0 ± 6.3 points, p = 0.009), and the significant
improvements were maintained until final follow-up (total score:
86.0 ± 6.8 points, p <0.001). The SAFE-Q scores were significantly
higher at post-operation and final follow-up than at pre-operation
(all p < 0.001), as shown in Table 2. Shoe-related points were relatively lower than other points at all times.
Patient satisfaction at post-operation was relatively high (8.4
±1.0 points) and maintained until final follow-up (8.6 ± 0.8 points).
Radiographic outcomes
Radiographic results are shown in Figure 4. The α angles were
improved at post-operation (2.5 ± 3.9°) and final follow-up (2.1 ±
4.3°) compared to pre-operation (9.1 ± 9.4°) (p = 0.128, p = 0.043,
respectively). The β angle also improved at post-operation (7.6 ±
2.1°) compared to pre-operation (74.1 ± 18.2°, p = 0.001) and was
maintained until final follow-up (7.8 ± 2.1°, p = 0.003). All cases
showed bone fusion of the PIP joint at six months postoperatively.
Complications
There were no cases of delayed wound healing, intraoperative
fracture, superficial infection, deep infection, or implant removal
by the time of final follow-up.
Table 1: Rheumatoid arthritis patients’ baseline demographic
characteristics.
|
6 RA patients, 11 lesser toes |
| Age, year |
62.6 ± 6.0 |
| Men: Women, n |
01:05 |
| BMI, kg/m2 |
22.1 ± 2.8 |
| Disease duration, years |
22.7 ± 10.5 |
| Follow-up duration, months |
21.0 ± 15.2 |
| DAS28-ESR |
3.38 ± 0.43 |
| mHAQ |
0.625 (0.5, 0.75) |
| Steinbrocker stage |
IV:6 |
| Steinbrocker class |
2:3, 3:3 |
| CRP, mg/dl |
0.09 (0.08, 0.14) |
| MMP3, ng/ml |
67.4 (57.2, 82.0) |
| RF positive. % |
83.3 |
| Methotrexate, mg/week, rate (%) |
7.0 ± 1.2 (66.7) |
| Glucocorticoid, mg/day, rate (%) |
3.2 ± 1.3 (66.7) |
| bDMARDs or tsDMARDs rate, % |
50 |
| JSSF lesser scale total, points |
31.9 ± 9.0 |
| Pain, points |
16.4 ± 8.1 |
| Function, points |
15.5 ± 3.3 |
| Alignment, points |
0 ± 0 |
| Larsen grade |
4:2, 5:4 |
Data are shown as means ± standard deviation (SD) for those with a
normal distribution or as medians (25th, 75th percentiles) for those not
normally distributed.
RA: Rheumatoid arthritis; BMI: Body Mass Index; DAS: disease activity
score; ESR: Erythrocyte Sedimentation Rate; mHAQ : Modified Health
Assessment Questionnaire; CRP: C-Reactive Protein; MMP3: Matrix
Metalloproteinase 3; RF: Rheumatoid Factor; bDMARDs: Biological
Disease-Modifying Antirheumatic Drugs; tsDMARDs: Targeted Synthetic
Disease-Modifying Antirheumatic Drugs; JSSF: Japanese Society for
Surgery of the Foot.
Table 2: SAFE-Q scores at pre-, post-operation, and final follow-up.
|
Pre-operation |
Post-operation |
Final follow-up |
| Pain, points |
52.6 ± 21.6 |
89.5 ± 8.3* |
89.5 ± 8.3* |
| Physical functions, points |
48.4 ± 18.3 |
82.9 ± 12.7* |
82.8 ± 12.7* |
| Social functioning, points |
40.5 ± 28.2 |
80.2 ± 21.8* |
80.2 ± 21.8* |
| Shoe related, points |
16.7 ± 6.5 |
65.1 ± 11.7* |
67.4 ± 10.8* |
| General health, points |
25.5 ± 12.5 |
84.1 ± 13.8* |
85.5 ± 14.0* |
Data are shown as means ± standard deviation (SD).
Continuous variables were analyzed using the Freidman signed-rank
test, adjusted Bonferroni.
*: p < 0.001 compared with the pre-operation score.
Discussion
This is the first study to investigate the clinical and radiographic
results of PIP joint arthrodesis by this specific dual-component
intramedullary implant for RA forefoot deformity. Strong initial
fixation was obtained, and bone fusion was achieved in all cases
by the interlocking mechanism of the Nextra® Hammertoe Correction System. Jay et al. reported the advantage of this system
[6]. The surgeon can seat the proximal and middle phalangeal
components of the 2-piece implant to the desired level in each
ossicle, thereby creating bone-to-bone contact as soon as the
implant components are coupled. The degree of bone-to-bone
contact remains constant thereafter, because each component
of the implant is screwed into the corresponding phalanx and,
as such, cannot piston, rotate, or flex. Witt et al. described the
characteristics of intramedullary fixation devices as resistance to
flexion, rotation, and pistoning, those that effect interfragmental
compression, and those that are not simply round in the crosssection [14].
In a systematic review comparing intramedullary implants
and K-wires, the only benefit of intramedullary implants was the
bone fusion rate, with no significant differences in pain relief,
patient satisfaction, function, or complication rates [15]. On the
other hand, in a randomized, controlled trial comparing clinical
scores and bone healing of separate type intramedullary implants
(47 toes) and K-wires (45 toes), patient satisfaction at one week
postoperatively and early bone healing were significantly better
with the separate type intramedullary implant than with the K-wires [6]. Patient satisfaction with the intramedullary implant was
due to the fact that the wire did not protrude from the phalangeal apex, which allowed for early bathing and the ability to wear
shoes. The bone-to-bone contact caused by crimping through a
locking mechanism was also a factor in the good bone fusion.
The advantages of the separate type intramedullary implants
are high patient satisfaction in the early postoperative period,
early postoperative bone fusion, and reduced risk of infection,
whereas the disadvantages are difficulty in removal due to infection and high cost.
RA patients are at higher risk of postoperative infection than
osteoarthritis patients [16]. In RA patients, foot and ankle surgery
is reported to have a higher risk of infection than that of other
sites [8,17]. In addition, osteoporosis is a complicating factor that
leads to poor initial fixation and delays bone healing. These considerations make dual-component type intramedullary implants
potentially more useful than K-wire fixation and single-device
type intramedullary implants.
The present study has several limitations that must be considered. First, the sample size was small, because metatarsal shortening osteotomy and resection arthroplasty have been mainly
performed for hammer toe in RA patients. Second, bone fusion
was determined only by radiography, with no CT performed.
Third, there was no comparison with K-wire fixation or single-device type intramedullary implants. Finally, the follow-up periods
were too short to evaluate the longevity of the dual-component
intramedullary implant. A longer follow-up period is necessary to
investigate the clinical and radiographic results in the future.
Conclusions
The present study showed the clinical and radiographic results
of PIP joint arthrodesis by a specific dual-component intramedullary implant for RA forefoot deformity. Anteroposterior and lateral alignments of the PIP joint on radiography were improved at
post-operation and maintained until final follow-up. There were
no cases of delayed wound healing, intraoperative fracture, superficial infection, deep infection, or implant removal by the time
of final follow-up. Patient satisfaction was high. The PIP joint arthrodesis with dual-component intramedullary implant might be
one of the useful methods for hammer toes in patients with RA.
Funding: None.
Conflict of interest statement: All authors declare no conflict
of interest.
Data availability: The datasets used and/or analyzed during
the current study are available from the corresponding author on
reasonable request.
References
- Michelson J, Easley M, Wigley FM, Hellmann D. Foot and ankle
problems in rheumatoid arthritis. Foot Ankle Int. 1994; 15: 608-613.
- Yano K, Ikari K, Iwamoto T, Saito A, Naito Y, et al. Proximal rotational closing-wedge osteotomy of the first metatarsal in rheumatoid arthritis: clinical and radiographic evaluation of a continuous
series of 35 cases. Mod Rheumatol. 2013; 23: 953-958.
- Tada M, Koike T, Okano T, Sugioka Y, Wakitani S, et al. Preference
of surgical procedure for the forefoot deformity in the rheumatoid
arthritis patients--A prospective, randomized, internal controlled
study. Mod Rheumatol. 2015; 25: 362-366.
- DiPaolo ZJ, Ross MS, Laughlin RT, Gould G, Flower K, et al. Proximal
phalanx and flexor digitorum longus tendon biomechanics in flexor to extensor tendon transfer. Foot Ankle Int. 2015; 36: 585-590.
- Ceccarini P, Rinonapoli G, Sebastiani E, Bisaccia M, Ceccarini A,
et al. Clinical Comparison Between Shortening Osteotomy of the
Proximal Phalanx Neck and Arthrodesis in Hammer Toe Surgery at
Mid-TermFollow-Up. J Foot Ankle Surg. 2019; 58: 221-225.
- Jay RM, Malay DS, Landsman AS, Jennato N, Huish J, et al. Dual-Component Intramedullary Implant Versus Kirschner Wire for
Proximal Interphalangeal Joint Fusion: A Randomized Controlled
Clinical Trial. J Foot Ankle Surg. 2016; 55: 697-708.
- Hofstaetter SG, Hofstaetter JG, Petroutsas JA, Gruber F, Ritschl P, et
al. The Weil osteotomy: a seven-year follow-up. J Bone Joint Surg
Br. 2005; 87: 1507-1511.
- Tada M, Inui K, Sugioka Y, Mamoto K, Okano T, et al. Delayed
wound healing and postoperative surgical site infections in patients with rheumatoid arthritis treated with or without biological
disease-modifying antirheumatic drugs. Clin Rheumatol. 2016; 35: 1475-1481.
- Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de
Putte LB, et al. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective
longitudinal study of patients with rheumatoid arthritis. Arthritis
Rheum. 1995; 38: 44-48.
- LeLièvre J. The pathology of the Foot. Physiology and Clinical Aspects and Medical, Orthopaedic and Surgical Treatment. Paris:
Masson et Cie. 1961.
- Hanyu T, Yamazaki H, Murasawa A, Tohyama C. Arthroplasty for
rheumatoid forefoot deformities by a shortening oblique osteotomy. Clin Orthop Relat Res. 1997; 131-138.
- Niki H, Aoki H, Inokuchi S, Ozeki S, Kinoshita M, Kura H, et al. Development and reliability of a standard rating system for outcome
measurement of foot and ankle disorders I: development of standard rating system. J Orthop Sci. 2005; 10: 457-465.
- Niki H, Tatsunami S, Haraguchi N, Aoki T, Okuda R, et al. Validity
and reliability of a self-administered foot evaluation questionnaire
(SAFE-Q). J Orthop Sci. 2013; 18: 298-320.
- Witt BL, Hyer CF. Treatment of hammertoe deformity using a one-piece intramedullary device: a case series. J Foot Ankle Surg. 2012;
51: 450-456.
- Wei RX, Ling SK, Lui TH, Yung PS. Ideal implant choice for proximal
interphalangeal joint arthrodesis in hammer toe/claw toe deformity correction: A systematic review. J Orthop Surg (Hong Kong).
2020; 28: 2309499020911168.
- Cordtz R, Odgaard A, Kristensen LE, Overgaard S, Dreyer L. Risk of
medical complications following total hip or knee arthroplasty in
patients with rheumatoid arthritis: A register-based cohort study
from Denmark. Semin Arthritis Rheum. 2020; 50: 30-35.
- Kadota Y, Nishida K, Hashizume K, Nasu Y, Nakahara R, et al. Risk
factors for surgical site infection and delayed wound healing after
orthopedic surgery in rheumatoid arthritis patients. Mod Rheumatol. 2016; 26: 68-74.