Introduction
Increased pressure in the pulmonary circulation in patients
with damage to the valvular apparatus of the heart reduces the
effectiveness of surgical intervention, reduces the topic of post-operative reverse remodeling of the cardiac cavities, and also
increases the risk of recurrence of AF after radiofrequency atrial
ablation according to the Maze IV scheme [1]. The feasibility of
correcting PH was discussed in S. Briongos Figuero et al., Where it
was demonstrated that a preoperative high degree of PH is closely
correlated with the preservation of PH even after surgical treatment of mitral valve disease (odds ratio 1.761; p = 0.03) [2].
The location of the sympathetic nerve plexuses in the adventitia of the trunk and the orifices of the pulmonary arteries responsible for spasm of the pulmonary arterioles and an increase in PH
was first reported in the works of J. Osorio in 1962 [3]. These data
were subsequently confirmed in B.G. Baylenet. al. [4] and C.E. Juratschet. al. [5].
Currently, conservative treatment of high PH does not allow
for a steady decrease in pressure in the pulmonary circulation,
and associated with the use of expensive drugs [6].
The first surgical interventions for high PH were first proposed
by S.L. Chen in 2013, in the form of endovascular catheter ablation of the trunk and the orifices of the pulmonary arteries,
which, according to the authors, allowed to significantly reduce
the pressure in the pulmonary artery [7].
In recent years, several works on the surgical correction of PH
in patients with mitral dysfunction during extracorporeal circulation, simultaneously with surgical treatment of mitral disease,
have been presented. A technique was proposed for radiofrequency ablation of the anterior wall of the trunk and the mouths
of the pulmonary arteries using a monopolar electrode. Also currently used is the method of circular radiofrequency denervation
of the pulmonary arteries using a bipolar RF clamps [8,9]. Despite
the existing correction methods of PH, the problem of surgical
treatment of high secondary PH is the most urgent, since there is
no generally accepted algorithm for treating this pathology, further investigation of the problem with finding the optimal surgical
technique for this category of patients is necessary.
Patients and methods
During the research work, an analysis of the surgical treatment of 202 patients with mitral valve disease complicated by
high PH (mean pulmonary arterial pressure (mPAP) is more than
40 mmHg) and AF was performed. Patients underwent surgical
correction of mitral valve disease – valve replacement or valve
repair – the first group of patients (n = 62). In patients of the second group (n = 89), mitral valve disease correction was also performed, as well as the Maze IV procedure was performed in connection with concomitant AF using the AtriCure bipolar radiofrequency ablator. Patients of the third group (n = 51) underwent a
comprehensive surgical intervention consisting in the mitral valve
intervention, surgical correction of AF in the form of the Maze IV
procedure, and circular PADN was performed. Inclusion criteria
was mitral valve disease complicated by AF and high secondary
PH. Exclusion criteria were history of pulmonary embolism, hemodynamically significant coronary artery lesions. The study has
been approved by local ethical committee, register number 10/D-2019 from 05.26.2019. All the studied patients before the operation, without fail, were informed about the upcoming additional
procedure PADN, which was planned to be performed with the
main stage of surgical correction, signed informed voluntary, according to the principles of clinical practice (Good Clinical Practice
- GCP), in accordance with the Helsinki Declaration.
Patients of all study groups were comparable for the main clinical and instrumental parameters (Table 1).
The presented data characterize patients of the 3rd group as
more severe in age, EUROSCORE, left ventricle contractility, dilatation of the left ventricle and the right heart, and the severity of PH.
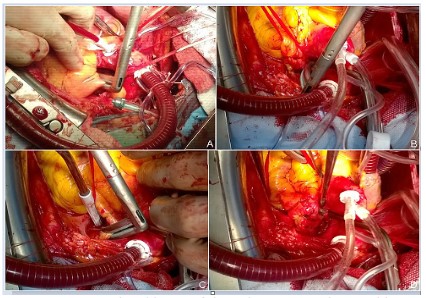
The PADN procedure was performed circularly with AtriCure’s
Isolator Synergy Bipolar Radiofrequency Clamps. After mobilization of the pulmonary trunk and orifices of bilateral pulmonary
arteries, in conditions of beating heart with the concomitant use
of cardiopulmonary bypass, 2 ablative circular lines were applied
to the distal part of the pulmonary trunk, each line consisted of 3
applications (Figure 1A).
Later, the orifices of the right pulmonary artery were isolated
and similar circular ablation lines were applied (Figure 1B).
In some cases, the isolation of the right pulmonary artery was
performed through the subaortic access, to the right of the aorta,
in the transverse sinus of the heart. Similarly, circular denervation
was performed in the area of the orifice of the left pulmonary
artery (Figure 1C).
Procedure in the final represents 6 ablation lines, 2 at the level
of the distal part of the pulmonary trunk and 2 at the orifices of
bilateral pulmonary arteries (Figure 1D).
Mean overall PADN procedure time was 5.5 minutes. After radiofrequency denervation of the pulmonary arteries antegrade
custodiole cardioplegia was performed into the aortic root and,
after the cardiac arrest, the main stage of the operation was performed - correction of valvular heart dysfunction and the Maze IV
procedure. Mean overall aortic cross-clamp time was 85.2 minutes, cardiopulmonary bypass time was 114.1 minutes. Patients
stayed in the intensive care unit for an average 2.4 days. Postoperative management of patients of the Denervation group did not
differ from the management of patients in the others ones. All
patients were followed with periodic visits through ECHO control
in 3, 6, 12, 24 months after surgery.
Statistical processing of the results was carried out in the program “SPSS Statistics 26”. Quantitative data were described as
mean and standard deviation (M ± σ), in the absence of a normal distribution, or rank data as the median and upper and lower
quartiles - Me (Q1-Q3).
The statistical significance of the differences for the quantitative data in the normal distribution was estimated by the Student
t-test, and in the absence of a normal distribution and for rank
data, it was evaluated by the Mann–Whitney U-test. Normality of
distribution was checked by the Shapiro-Wilk test. For qualitative
data (relative values), the differences were evaluated using the
Pearson’s chi-squared test (χ2). If the number of observations, at
least in one of the fields of Table 2, was less than 5, the calculation
was performed using the Fisher’s exact test.
If it was necessary to compare 3 groups at the same time, the
Kruskal-Wallis test (for quantitative and rank data) and the chi-squared test (for qualitative data) were used. Error probability (p)
was considered acceptable at p < 0.05. With the successive repeated application of the statistical criteria of Student, chi-square
and Mann-Whitney (alternately comparing the groups among
themselves), the probability of detecting differences, where there
are none, increases by N times. Therefore, in the triple sequential
comparison of the groups, the Bonferroni correction was used,
an acceptable significance level (p) was calculated as p = 0.05/n,
where n = 3, i.e., 0.0167.
Results
Fatal outcomes among patients occurred one in each group
and were caused by acute progressive heart failure on the first
day after surgery. There were no postoperative complications associated with the PADN procedure. According to the data of trans-thoracic ECHO, all patients showed improvement in the postoperative period (Table 2). There was no significant decrease in AF
frequency only in group 1.
Since the main criteria for evaluating the effectiveness of treatment is the achievement of target indicators, the final results
in the study groups are analyzed in the form of a share of the
achieved indicators.
For indicators of ECHO, the range of normal values were taken
(Table 3).
The table shows that with comparable initial indicators, the
achievement of the target indicators in group 3 is significantly
better, including in comparison with group 2, even taking into
account the Bonferoni correction. Positive changing according
to the McNemar criterion was noted for almost all indicators in
groups 2 and 3. Group 1 did not achieve a statistically significant
improvement in the sizes of LA and RA, normalization of mPAP,
restoration of sinus rhythm.
The presented ECHO data demonstrate significant positive
changes in the group of complex surgical treatment for reverse
remodeling of the cardiac cavities, lower mPAP, increase the left
ventricular ejection fraction, restore and restoration of the sinus
rhythm, in comparison with groups 1 and 2.
Circular denervation of the sympathetic ganglia in the trunk
and mouth of the pulmonary arteries, after the PADN procedure,
helps to relax smooth muscle fibers in the vascular wall, which
leads to dilatation of arteries and arterioles, increasing the capacity of the vascular bed in the pulmonary circulation and reduces
PH in the postoperative period.
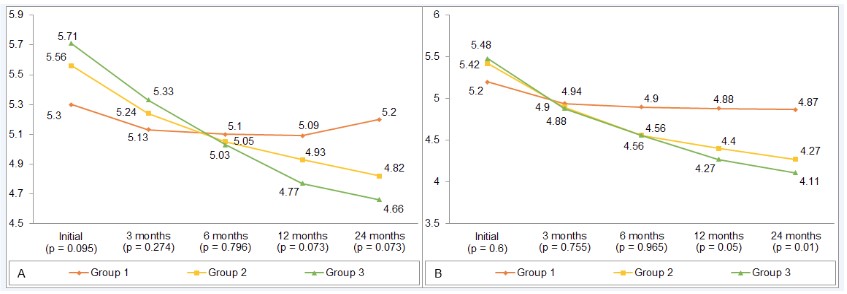
In the course of the work, the dynamics of mPAP the was analyzed according to transthoracic ECHO (Figure 2).
Indicators of PH in group 3, initially significantly worse, were
comparable with indicators of groups 1 and 2 already 3 months
after the operation, and subsequently the best indicators among
study groups. Normalization of PH contributed to a decrease in
pressure in the right heart, primarily in the right ventricle, which
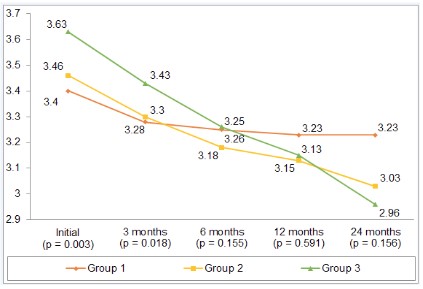
had a beneficial effect on the reverse remodeling of the right ventricular cavity in the postoperative period (Figure 3).
Also, significant existing dilatation of the right ventricle after
6 months was comparable in terms of average values to groups
1 and 2, and by 24 months it occupied a leading position among
all study groups. Concomitant tricuspid valve insufficiency, which
was observed in almost all patients and was eliminated during the
operation through repair, also had a positive trend in the postoperative period (Figure 4A).
The positive effect of surgical correction also affected the reduction of heart failure according to the 6-minute walk test (Figure 4B).
The results presented in the diagram demonstrate the significant advantage of the complex surgical treatment applied in
group 3 already 3 months after surgery, compared with groups 1
and 2.
The elimination of tricuspid insufficiency, against the background of a decrease in pressure in the right heart, contributed to
a reduction in the right atrium cavity (Figure 5A).
The presented diagram shows the best dynamics of cardiac
reverse remodeling in the group of complex surgical treatment
(group 3) - a more pronounced dilatation of the right atrium before surgery, was comparable with the average values of groups 1
and 2, and from 12 months had the best performance among the
study groups.
A comprehensive surgical approach in group 3 made it possible
to increase the effectiveness of surgical treatment of AF, which
significantly improved the results of restoration and preservation
of sinus rhythm in the postoperative period compared with patients of groups 1 and 2 (Table 2). The restored sinus rhythm contributed to a better reverse remodeling of the left atrium cavity
(Figure 5B).
The presented data demonstrate a significant reduction in
heart failure in group 3 from 12 months after surgery, compared
with patients of groups 1 and 2, which is due to positive changes in
the hemodynamic and structural parameters of the myocardium.
Table 1: Clinical and instrumental characteristics of the studied patients (n = 202).
|
Group 1 |
Group 2 |
Group 3 |
p Value |
| (n = 62) |
(n = 89) |
(n = 51) |
1-2 |
1-3 |
2-3 |
| Gender (male/female) |
19/43 |
28/61 |
23/28 |
0.916 |
0.116 |
0.108 |
| Age at operation, years |
56.3 ± 8.0 |
55.8 ± 8.3 |
59.4 ± 5.2 |
0.740 |
0.017#a |
0.005# |
| Cause of mitral valve disease, % |
| Rheumatic fever |
82 |
85 |
76 |
0.604 |
0.447 |
0.184 |
| Infective endocarditis |
8 |
9 |
20 |
0.842 |
0.073 |
0.072 |
| Degenerative |
10 |
6 |
4 |
0.345 |
0.235 |
0.657 |
| Type of AF |
|
|
|
|
|
|
| Long-term persistent |
77 |
84 |
86 |
0.167 |
0.321 |
0.749 |
| Persistent |
8 |
2 |
8 |
0.094 |
0.965 |
0.116 |
| Paroxysmal |
15 |
13 |
6 |
0.857 |
0.138 |
0.162 |
| Arrhythmia history, years |
2.7 ± 2.2 |
2.7 ± 1.7 |
2.6 ± 1.4 |
2.6 ± 1.4 |
0.887 |
0.688 |
| Atrial flutter, % |
10 |
20 |
14 |
0.081 |
0.501 |
0.385 |
| Carotid stenosis > 50%, % |
27 |
17 |
18 |
0.118 |
0.219 |
0.904 |
| Past medical history of a stroke, % |
10 |
8 |
8 |
0.867 |
0.320 |
1 |
| EuroSCORE |
5 (3-6) |
4 (3-6) |
5 (4-8) |
0.817 |
0.004# |
0.004# |
| Cardiopulmonary bypass time, min |
110 (90-136) |
136 (118-151) |
111 (87-130) |
0.006# |
0.511 |
<0.001# |
| Aortic cross-clamp time, min |
84.5 (70-102) |
107 (92-128) |
79 (67-102) |
<0.001# |
0.359 |
<0.001# |
| TVI 2-4 degree, % |
54.8 |
76.4 |
64.7 |
0.016# |
5.33 |
0.095 |
| NYHA III-IV class, % |
27.4 |
28.1 |
43.1 |
0.953 |
0.082 |
0.058 |
| LVIDd, cm |
5.5 (5.2-6.3) |
5.5 (5.2-5.7) |
5.6 (5.4-6.4) |
0.245 |
0.349 |
0.014# |
| LVIDs, cm |
4.2 (3.7-4.8) |
3.8 (3.6-4.1) |
4 (3.8-4.8) |
0.002# |
0.925 |
<0.001# |
| LVEDV, cm |
147.4 (129.5-201.2) |
143.2 (130.4-160) |
153.7 (135.3-208.5) |
0.176 |
0.465 |
0.016# |
| LVESV, cm |
76.4 (58.1-107.5) |
62 (54.4-71.2) |
70 (62.0-107.5) |
0.001# |
0.902 |
<0.001# |
| LVEF, % |
51 (43.9-57.9) |
56.3 (53.1-58) |
52.2 (49.1-55.1) |
<0.001# |
0.080 |
<0.001# |
| RVD, cm |
3.4 (3.2-3.6) |
3.4 (3.2-3.7) |
3.6 (3.4-4) |
0.182 |
<0.001# |
0.003# |
| LADs, cm |
5.1 (4.8-5.7) |
5.4 (5.2-5.6) |
5.5 (5.3-5.7) |
0.034 |
0.002# |
0.600 |
| RADs, cm |
5.2 (5-5.7) |
5.6 (5.2-5.9) |
5.8 (5.6-6) |
0.004# |
<0.001# |
0.095 |
| PASP, mmHg |
46 (43-49) |
46 (44-50) |
48 (45-60) |
0.440 |
0.002# |
0.018 |
aHereinafter, for most cases (for the age of patients and AF, Student t-test was used), intergroup differences were calculated by the Mann–Whitney
U-test due to the lack of a normal distribution (in this case, the data are presented as Me (Q1-Q3)), for qualitative values used the Pearson's chi-
squared test or the Fisher's exact test. The # sign indicates the required level of statistical significance, taking into account the Bonferroni correction.
LADs: Left Atrium Anterior-Posterior Diameter In Systole; LVEDV: Left Ventricular End-Diastolic Volume; LVEF: Left Ventricular Ejection Fraction;
LVESV: Left Ventricular End-Systolic Volume; LVIDd: Left Ventricular Internal Diameter In Diastole; LVIDs: Left Ventricular Internal Diameter In Systole;
PASP: Pulmonary Artery Systolic Pressure; RADs: Right Atrium Anterior-Posterior Diameter In Systole; RVD: Right Ventricular Basal Diameter; TVI:
Tricuspid Valve Insufficiency.
Table 2: Changing of echocardiographic parameters of the studied groups.
|
|
Group 1 |
Group 2 |
Group 3 |
p Value |
| (n = 62) |
(n = 89) |
(n = 51) |
1-2 |
1-3 |
2-3 |
| TVI 2-4 degree, % |
original |
54.8 |
76.4 |
64.7 |
0.016#a |
0.533 |
0.095 |
| 24 Mo. after |
32.80*b |
20.5* |
0* |
0.044 |
<0.001# |
<0.001# |
| NYHA III-IV class, % |
original |
100 |
98.9 |
100 |
0.953 |
0.082 |
0.058 |
| 24 Mo. after |
67.2 |
36.4* |
18.0* |
<0.001# |
<0.001# |
0.023 |
| LVIDd, cm |
original |
5.5 (5.2-6.3) |
5.5 (5.2-5.7) |
5.6 (5.4-6.4) |
0.245 |
0.349 |
0.014# |
| 24 Mo. after |
5.3 (5-6)* |
4.8( 4.6-5.1)* |
4.6 (4.5-5.3)* |
<0.001# |
<0.001# |
0.896 |
| LVIDs, cm |
original |
4.2 (3.7-4.8) |
3.8 (3.6-4.1) |
4 (3.8-4.8) |
0.002# |
0.925 |
<0.001# |
| 24 Mo. after |
3.9 (3.4-4.3)* |
3.3 (3.1-3.7)* |
3.2 (3-3.6)* |
<0.001# |
<0.001# |
0.625 |
| LVEDV, cm |
original |
147.4 (129.5-201.2) |
143.2 (130.4-160.0) |
153.7 (135.3-208.5) |
0.176 |
0.465 |
0.016# |
| 24 Mo. after |
135.3 (118.2-180)* |
105.9 (97.3-123.8)* |
97.3 (93.8-135.3)* |
<0.001# |
<0.001# |
0.858 |
| LVESV, cm |
original |
76.4 (58.1-107.5) |
62.0 (54.4-71.2) |
70 (61.9-107.5) |
0.001# |
0.902 |
<0.001# |
| 24 Mo. after |
65.9 (47.4-83.1)* |
44.1 (36.5-57.7)* |
42.6 (35-54.43)* |
<0.001# |
<0.001# |
0.691 |
| LFEV, % |
original |
51.0 (43.9-57.9) |
56.3 (53.1-58.0) |
52.2 (49.1-55.1) |
<0.001# |
0.08 |
<0.001# |
| 24 Mo. after |
53.4 (47.6-57.0)* |
57.9 (54.4-63.3)* |
58.2 (56.3-60.1)* |
<0.001# |
<0.001# |
0.857 |
| RVD, cm |
original |
3.4 (3.2-3.6) |
3.4 (3.2-3.7) |
3.6 (3.4-4) |
0.182 |
<0.001# |
0.003# |
| 24 Mo. after |
3.2 (3-3.4)* |
3.0 (2.9-3.1)* |
2.9 (2.8-3.2)* |
<0.001 |
<0.001 |
0.156 |
| LADs, cm |
original |
5.1 (4.8-5.7) |
5.4 (5.2-5.6) |
5.5 (5.3-5.7) |
0.034 |
0.002# |
0.600 |
| 24 Mo. after |
4.8 (4.5-5.3)* |
4.3 (4-4.6)* |
4.1 (3.8-4.3)* |
<0.001# |
<0.001# |
0.010# |
| RADs, cm |
original |
5.2 (5-5.7) |
5.6 (5.2-5.9) |
5.8 (5.6-6) |
0.004# |
<0.001# |
0.095 |
| 24 Mo. after |
5.1 (5-5.5)* |
5.0 (4.4-5.3)* |
4.5 (4.4-5)* |
<0.001# |
<0.001# |
0.073 |
| PASP, mmHg |
original |
46 (43-49) |
46 (44-50) |
48 (45-60) |
0.44 |
0.002# |
0.018 |
| 24 Mo. after |
32 (30-34)* |
26 (23.5-29.4)* |
23 (21-28)* |
<0.001# |
0.583 |
0.519 |
| AF, % |
original |
100 |
100 |
100 |
1 |
1 |
1 |
| 24 Mo. after |
95 |
34* |
16* |
<0.001# |
<0.001# |
0.022 |
aIntergroup differences were calculated by the Mann–Whitney U-test due to the lack of a normal distribution (in this case, the data are presented
as Me (Q1-Q3)), for qualitative values used the Pearson's chi-squared test or the Fisher's exact test. The # sign indicates the required level of
statistical significance, taking into account the Bonferroni correction.
bThe statistical significance of dynamic differences was indicated by the *sign in the data line after 24 months, for quantitative data it was
evaluated by the Wilcoxon sign test, for analysis of repeated measurements of qualitative characteristics - by the McNemar test with Yates
correction (changes in the percentage of TVI 0-1 degree, the NYHA II-IV share, AF percentage).
LADs: Left Atrium Anterior-Posterior olume; LVIDd: Left Ventricular Internal Diameter In Diastole; LVIDs: Left Ventricular Internal Diameter In
Systole; PASP: Pulmonary Artery Systolic Pressure; RADs: Right Atrium Anterior-Posterior Diameter In Systole; RVD: Right Ventricular Basal
Diameter; TVI: Tricuspid Valve Insufficiency.
Table 3: The share of target indicators 24 months after surgery in the study groups.
|
|
Group 1 |
Group 2 |
Group 3 |
p Value |
| (n = 62) |
(n = 89) |
(n = 51) |
1-2 |
1-3 |
2-3 |
| TVI 0-1 degree, % |
original |
45.2 |
23.6 |
35.3 |
0.005#a |
0.288 |
0.137 |
| 24 Mo. after |
67.2*b |
79.5* |
100* |
0.089 |
<0.001# |
<0.001# |
| TVI 0 degree, % |
original |
1.6 |
0 |
0 |
0.229 |
0.362 |
1 |
| 24 Mo. after |
0 |
3.4 |
88* |
0.091 |
<0.001# |
<0.001# |
| NYHA I-II class, % |
original |
0 |
1.1 |
0 |
0.402 |
1 |
0.447 |
| 24 Mo. after |
32.8* |
63.6* |
82* |
<0.001 |
<0.001 |
0.023 |
| Sinus rhythm preservation, % |
original |
0 |
0 |
0 |
1 |
1 |
1 |
| 24 Mo. after |
4.9 |
65.9* |
82* |
<0.001 |
<0.001 |
0.023 |
| LVIDd, cm |
original |
38.7 |
47.2 |
31.4 |
0.301 |
0.417 |
0.067 |
| 24 Mo. after |
50.8* |
87.5* |
92.0* |
<0.001# |
<0.001# |
0.414 |
| LVIDs, cm |
original |
24.2 |
38.2 |
19.6 |
0.07 |
0.559 |
0.023 |
| 24 Mo. after |
44.3* |
72.7* |
98* |
<0.001# |
<0.001# |
<0.001# |
| LVEDV, cm |
original |
21 |
21.3 |
11.8 |
0.955 |
0.193 |
0.154 |
| 24 Mo. after |
36.1* |
64.8* |
66* |
<0.001# |
<0.001# |
0.884 |
| LVESV, cm |
original |
14.5 |
19.1 |
11.8 |
0.463 |
0.668 |
0.26 |
| 24 Mo. after |
29.5* |
64.8* |
62* |
<0.001# |
<0.001# |
0.745 |
| LFEV, % |
original |
38.7 |
76.4 |
52.9 |
<0.001# |
0.13 |
0.004# |
| 24 Mo. after |
49.2* |
81.8* |
96* |
<0.001# |
<0.001# |
0.018 |
| RVD, cm |
original |
40.3 |
44.9 |
21.6 |
0.573 |
0.033 |
0.006# |
| 24 Mo. after |
68.9* |
83* |
96* |
0.044 |
<0.001# |
0.03 |
| LADs, cm |
original |
3.2 |
4.5 |
0 |
0.695 |
0.196 |
0.125 |
| 24 Mo. after |
1.6* |
23.9* |
48* |
<0.001# |
<0.001# |
0.004# |
| RADs, cm |
original |
4.8 |
2.2 |
0 |
0.381 |
0.111 |
0.281 |
| 24 Mo. after |
0 |
33* |
54* |
<0.001# |
<0.001# |
0.016 |
| PASP < 25 mmHg |
original |
0 |
0 |
0 |
1 |
1 |
1 |
| 24 Mo. after |
3.3 |
34.1* |
62* |
<0.001# |
<0.001# |
0.002# |
aIntergroup differences were calculated by the Pearson's chi-squared test or the Fisher's exact test. The # sign indicates the required level of
statistical significance, taking into account the Bonferroni correction.
bThe statistical significance of repeated measurements of qualitative traits was evaluated by the McNemar test with Yates correction.
LADs: left atrium anterior-posterior diameter in systole; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction;
LVESV: left ventricular end-systolic volume; LVIDd: left ventricular internal diameter in diastole; LVIDs: left ventricular internal diameter in systole;
PASP: pulmonary artery systolic pressure; RADs: right atrium anterior-posterior diameter in systole; RVD: right ventricular basal diameter; TVI:
tricuspid valve insufficiency.
Comment
The performed research work demonstrates the effectiveness
of complex surgical correction in patients with mitral valve disease, AF, and severe secondary PH, which, in addition to the standard mitral valve dysfunction and Maze IV procedure, underwent
the PADN circular procedure (group 3). The control groups were
initially comparable according to the main clinical and instrumental data, they also underwent surgery for mitral disease (group 1)
and simultaneous elimination of mitral dysfunction and AF (group
2), but patients of these groups did not undergo specific surgical
treatment of secondary PH. Even with a small number of studied
patients and the lack of data on the effectiveness of the PADN
procedure in the long term, the presented results demonstrate
the better reverse remodeling of the cardiac cavities, as well as a
significant reduction in PH, restoration and preservation of the sinus rhythm in the postoperative period, which enhances the first
effect. Ultimately, the regressing of heart failure in patients of the
3rd group of the study is more pronounced in comparison with
the control groups. The achieved result was obtained not only due
to mitral valve disease surgery correction and restoration of sinus
rhythm after the Maze IV procedure, but also due to the circular
PADN procedure. The proposed method for surgical correction of
PH was simple in technical design, did not take much time and
during the course of the research work proved to be absolutely
safe.
The result of our work was a demonstration of the effectiveness, practical significance and safety of the proposed methodology. In addition, no additional consumables were required
to perform the PADN procedure, since the same AtriCure radio
frequency destructor, which was used for surgical correction of
AF, was used. The use of a bipolar clamp-destructor allows radiofrequency exposure around the entire circumference of the pulmonary arteries, which is advantageous in comparison with the
impacts of only the anterior wall of the trunk and the orifices of
bilateral pulmonary arteries.
Based on the data obtained, the following conclusions can be
drawn:
1. The circular PADN procedure is effective and safe, can significantly reduce the level of PH in the postoperative period
(рχ2 = 0.018 compared with the group without PADN) and
promotes reverse remodeling of the cardiac cavities.
2. Comprehensive surgical correction of patients with mitral
dysfunction, AF, and high PH can significantly reduce heart
failure (рχ2 = 0.023 compared with the group without
PADN).
3. Further analysis of the effectiveness of radiofrequency denervation of the pulmonary arteries with the study of a larger number of patients, analysis of long-term results, as well
as determining the feasibility of this technique in patients
with non-valve forms of PH is needed.
Declarations
Conflict of interest: None declared.
Funding statement: This work is supported by the Russian Science Foundation under grant 21-75-10075.
References
- Babokin VE, Trofimov NA. Prevention of Atrial Fibrillation Recurrence after the Maze IV Procedure. Ann Thorac Surg. 2019.
- Briongos Figuero S, Moya Mur JL, Garcia-Lledo A, et al. Predictors
of persistent pulmonary hypertension after mitral valve replacement. Heart Vessels. 2016; 31: 1091-1099.
- Osorio J, Russek M. Reflex changes on the pulmonary and systemic
pressures elicited by stimulation of baroreceptors in the pulmonary artery. Circ Res. 1962; 10: 664-667.
- Baylen BG, Emmanouilides GC, Juratsch CE, Yoshida Y, French WJ,
et al. Main pulmonary artery distention: a potential mechanism
for acute pulmonary hypertension in the human newborn infant. J
Pediatr. 1980; 96: 540-544.
- Juratsch CE, Jengo JA, Castagna J, Laks MM. Experimental pulmonary hypertension produced by surgical and chemical denervation
of the pulmonary vasculature. Chest. 1980; 77: 525-530.
- Guazzi M, Vitelli A, Labate V, Arena R. Treatment for pulmonary
hypertension of left heart disease. Curr Treat Options Cardiovasc
Med. 2012; 14: 319-327.
- Chen SL, Zhang FF, Xu J, et al. Pulmonary artery denervation to
treat pulmonary arterial hypertension: the single-center, prospective, first-in-man PADN-1 study (first-in-man pulmonary artery denervation for treatment of pulmonary artery hypertension). J Am
Coll Cardiol. 2013; 62: 1092-1100.
- nova SS, Babokin VE. Denervation of Pulmonary Arteries in Patients with Mitral Valve Defects Complicated by Atrial Fibrillation
and Pulmonary Hypertension. Sovremennye tehnologii v medicine. 2019; 11: 95-105.
- Trofimov NA, Medvedev AP, Babokin VE. Effect of circular sympathetic denervation of pulmonary arteries on the degree of pulmonary hypertension in patients with mitral valve pathology and
atrial fibrillation. Clin Experiment Surg. Petrovsky J. 2019; 4: 32-41.