Introduction
Urinary lithiasis if defined by stony concretion in the urinary
track. In recent decades the incidence of urinary lithiasis is regularly increasing. In the United States, it is estimated that 11% of
men and 5.6% of women will have experienced urinary lithiasis
by the age of 70 years with a 3-fold higher risk in Caucasian compared to African American [1]. More than 80% of these lithiasis are of calcium nature, essentially oxalo-calcic. Although the
mechanisms of stone formation are well clarified by a good understanding of lithogenesis [2], the site of stone formation is also
very important [3]. Papillary biopsies show differences in the site
of crystal deposits based on the nature of the lithiasis. Idiopathic
calcium oxalate crystals are formed in interstitial areas containing calcium phosphate crystals at the level of Randall’s plaques
of papillary surface [3], while calcium phosphate crystals are associated with internal deposits of apatite or a mixture of other
crystals in the collecting system of the medullary [4].
Bladder localization represents 5% of all urinary tract lithiasis
[5], they develop over many years and have varying sizes [6]. This
explains why giant bladder lithiasis are very rare. In men, urinary bladder stasis secondary to lower urinary tract obstruction and
neurogenic bladder are the main factors promoting bladder stone
formation [6]. Bladder lithiasis can be latent for a long period as
opposed to to upper tract lithiasis causing pain. In the period
2006-2018, it is reported that 11 million patients suffering from
urolithiasis benefitted from opioid therapy [7].
The aim of our study was to report 2 cases of giant bladder calcium lithiasis to present the clinical presentation, etiologic factors
and treatment and to perform a review of the literature to explain
the origin of this type of lithiasis compared to upper urinary track
lithiasis.
Case presentation #1
Mr M.A, is a 70 years old man, university faculty living in urban area, with a history of surgery for cataract referred in April
2020 for chronic urinary retention. He reported a long history of
difficulty passing urine prior to a urinary retention that occurred
in November 2019 in France at which time a trans urethral Foley
catheter was placed and changed on the regular basis.
Physical examination found a patient in good general condition
(WHO I), a distended bladder up to level of the umbilicus, trans
urethral Foley catheter was in place draining purulent urines. Digital rectal examination found an enlarged, firm, regular and painless prostate without the median groove. There was no fever.
The patient was immediately admitted, the Foley catheter was
replaced by a 3-way Foley catheter, a progressive drainage was
performed with bladder irrigation by saline.
Blood cell count showed 13,700 white blood cell/μL with a predominance of neutrophils and a hemoglobin concentration of 9.7
g/dl. CRP level was 140,5 mg/L, creatinine level was 67,8 mg/L
and serum electrolytes level was normal. Urine culture diagnosed
a urinary infection by Klebsiella Pneumonia sensitive only to amikacin, the patient subsequently underwent half dose of amikacin over 4 days due to the renal failure. Ultrasound examination
showed a prostatic volume of 51 ml and a bilateral ureteral and
kidney dilatation with good corticosinusal differentiation.
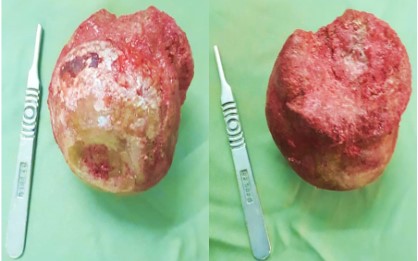
He underwent a cystolithotomy removing a giant lithiasis measuring 10 X 8 cm and weighing 581 g. The lithiasis was yellowish
and friable (Figure 1).
Post-operative course was marked by vesico cutaneous fistulae managed by prolonged drainage and regular dressing change.
The lithiasis was examined by spectrophotometry and infra-red
showing a composition of calcium oxalate (87%), calcium (10%)
and phosphor (3%). Trans Urethral resection of the prostate was
planned subsequently.
Case presentation #2
Mr T.P is a 65 years old man with a history of car accident in
1993 causing head trauma and coma. He was then admitted for
2 weeks in Intensive care unit with an indwelling Foley catheter.
He was referred to Urology department in September 2020 for
urinary retention preceded by a long period of difficulty passing
urine.
At examination the patient had a poor general condition (WHO
3), a distended bladder reaching the umbilicus, an enlarged prostate of benign appearance at digital rectal examination. The rest
of the clinical examination was normal.
An attempt to place a Foley catheter stuck in the urethra and
an attempt to place a suprapubic tube faced a very hard mass in the bladder.
Laboratory work found a creatinine level of 142.8 mg/I, hyperkaliemia (5,9 meq/L) and urine culture diagnosed an infection by
Klebsiella Pneumonia sensitive to chloramphenicol and amikacin
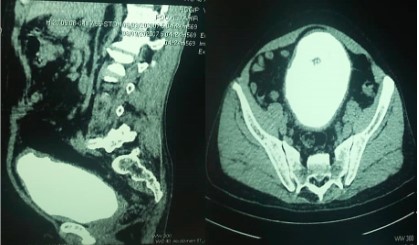
and the patient underwent antibiotic treatment. Ultrasonography
found a thickened bladder wall containing a giant lithiasis with an
important dilatation of both ureters and kidneys and a prostatic
volume of 67 ml. CT Scan without injection of contrast medium
confirmed the findings of ultrasonography and indicated a bladder lithiasis measuring 98x90x167 mm in size (Figure 2).
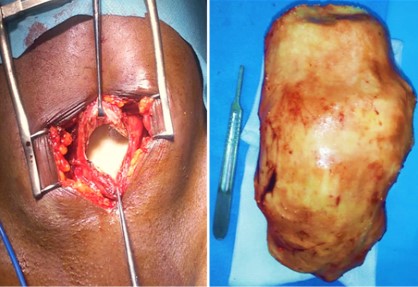
The patient immediately underwent a cystotomy showing a giant lithiasis occupying all the bladder, hard, yellowish and weighing 1517 g (Figure 3). A suprapubic tube was place to drain the
urines given the urethral stenosis.
Post-operative course was uneventful with a wound healing
without infection or fistula. The patient general condition improved and the creatinine and potassium levels became normal
at one-month post op. Spectrophotometric infra-red examination
of the lithiasis found a 100% phosphor calcic composition. The
patient was ordered to perform retrograde cystography to study
the urethral stricture but he was lost to follow-up.
Discussion
Bladder lithiasis poses a problem of its origin, most lithiasis
are formed in the kidneys and migrate into the ureters and bladder [3]. Local factors can then promote lithiasis growth. But the
bladder can be the initial site of lithiasis development mostly in
case of urinary stasis, like in our 2 cases. This is common in lower
urinary tract obstructions that cause post voiding bladder residue
and subsequently lithogenesis is initiated in the bladder [4]. Our
two patients presented an obstruction, the first one had a benign
prostatic hyperplasia complicated by urinary retention and the
second patient developed a urethral stricture secondary to a Foley catheter placement in a context of coma. Apart from lower urinary tract obstruction, neurogenic bladder is another important
cause of bladder urinary stasis that can promote in situ lithiasis
formation [4].
In our cases the composition of the lithiasis was essentially
made of calcium. Such findings are in accordance with the reported predominance of calcium lithiasis with a proportion of at
least 80% [2], this includes oxalocalcic and phophocalcic lithiasis.
However, Douenias R et al. reported a predominance of uric acid
lithiasis in bladder stones [6]. Urinary infection is often associated
with bladder stasis which in turn is a factor of urolithiasis formation. Infected urines by germs from the lithiasis can secondarily
cause post-operative wound infection and vesico cutaneous fistulae. Our first case experienced such a complication.
Although factors of lithogenesis in the bladder are mainly stasis and infection, the mechanism of lithiasis growth to the stage of
giant size remains to be explained. Delay in consultation in spite
of lower urinary tract symptoms is one of the key reasons especially because the bladder has the largest storing capacity of the
urinary tract segments allowing for a longer evolution of the disease conducive for lithiasis growth. Prolonged stasis due to the
bladder outlet obstruction contributes to the progressive growth
of the lithiasis.
Symptoms suggesting bladder lithiasis are dominated by supra-pubic pain, dysuria, hematuria, difficulty passing urine and irritative symptoms [8], however the condition can be asymptomatic.
Our two patients presented urinary retention given the big size of
the lithiasis and the underlying lower urinary tract obstruction.
Treatment consists of surgical ablation of the lithiasis and the
treatment of underlying condition. Our patients underwent open
cystolithotomy that will be followed by trans urethral prostatic resection in the first case and urethral reconstruction in the second
case after urethral imaging. Our surgical approach is similar to the
case report of Shrestha et al. [8] who removed a 950 g lithiasis in
a patient with no lower urinary tract obstruction or neurogenic
bladder. Other small size bladder lithiasis can be managed by a
variety of mini invasive endoscopic techniques: ultrasound, electrohydraulic, Holmium: YAG laser... [10].
Global bladder lithiasis management must also include prevention of recurrence taking into account the treatment of the
etiology, the composition of the lithiasis and the metabolic characteristics of the patients [11]. It is also important to treat urinary
infection that can promote bladder lithiasis [12].
Conclusion
Giant bladder lithiasis are rare and often secondary to neglected lower urinary tract disorders causing a stasis. Lithiasis
formation and growth can occur within many years and can be favored by delay in referral and lack of exploration. In the setting of
chronic bladder outlet obstruction, imaging should be performed
to search for lithiasis complication and treat both the lithiasis and
the obstruction.
References
- Stamatelou KK, Francis ME, Jones CA, Nyberg LM Jr, Curhan GC.
Time trends in reported pevalence of kidney stones in the United
States:1976–1994. Kid Int. 2003; 63: 1817-1823.
- Worcester EM, Coe FL, Elaine M. Clinical Practice Calcium Kidney
Stones. N Engl J Med. 2010; 363: 954-963.
- Miller NL, Gillen DL, Williams JC. A formal test of the hypothesis
that idiopathic calcium oxalate stones grow on Randall’s plaque.
BJU Int. 2009; 103: 966-971.
- Douenias R, Rich M, Badlani G, Mazor D, Smith A. Predisposing
factors in bladder calculi. Review of 100 cases. Urology. 1991; 37:
240-243.
- Schwartz BF, Stoller ML. The vesical calculus. Urol Clin North Am.
2000; 27: 333-346.
- Torricelli FC, Mazzucchi E, Danilovic A, Coelho RF, Srougi M. Surgical management of bladder stones: literature review. Rev Col Bras
Cir. 2013; 40: 227-233.
- Zhu D, Macdonald EJ, Lesko RP, Watts KL. National trends and prescription patterns in opiate analgesia for urolithiasis presenting to
Emergency Departments: Analysis of the National Hospital Ambulatory Medical Care Survey, 2006-2018. Urology. 2021; S0090-4295(21)01173-0.
- Papatsoris AG, Varkarakis I, Dellis A, Deliveliotis C. Bladder lithiasis:
from open surgery to lithotripsy. Urol Res. 2006; 34: 163.
- Shrestha N, Zhou L, Hu CH. Extraction of giant bladder calcium oxalate stone: A case report. Int J Surg Case Rep. 2020; 68: 151-153.
- Papatsoris AG, Varkarakis I, Dellis A, Deliveliotis C. Bladder lithiasis:
from open surgery to lithotripsy. Urol Res. 2006; 34: 163-167.
- Porena M, Guiggi P, Micheli C. Prevention of stone disease. Urol
Int. 2007; 79: 37-46.
- Mohamed AH, Yasar A, Mohamud HA. Giant bladder stone of 152g
in an 11-year child with recurrent urinary tract infections: A rare
case report and review of the literature. Urol Case Rep. 2021; 38:
101676.