Introduction
Good optics and infrared imaging and safe energy sources added recently in armamentarium of surgeons has increased safety
of laparoscopic cholecystectomy and CBD exploration. In spite of
advancement and improvement in techniques, certain anatomical variations spring surprises, and may lead to surgical complications -biliary and vascular. Laparoscopic cholecystectomy makes it
mandatory to have a thorough knowledge of normal anatomy and
variations in this region to reduce the likelihood of uncontrolled
intraoperative bleeding, iatrogenic extrahepatic biliary injury and
conversion to open cholecystectomy [1]. Incidence of conversion
to open surgery because of vascular injury is 0-1.9% and mortality
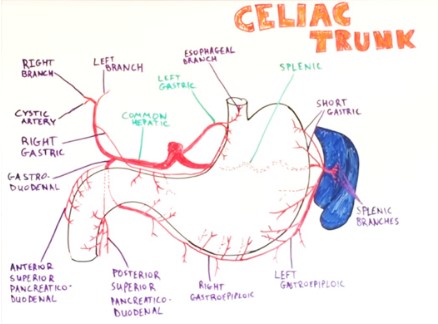
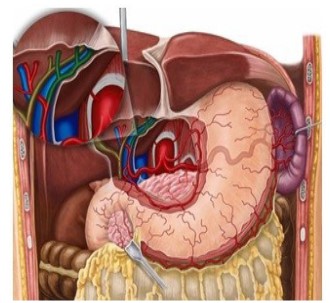
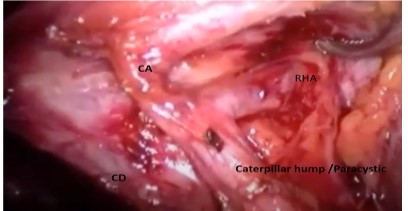
is 0.02% [2]. The right hepatic artery after its origin from hepatic
artery proper crosses anterior to the portal vein and then passes
behind the common hepatic duct to enter the Calot’s triangle
(bounded by cystic duct, common hepatic duct and lower edge
of the liver). As it approaches the cystic duct, it gives off the cystic
artery and then turns upwards, behind (and between) the right
hepatic and the cystic duct to the right lobe of the liver (Figure
1, and Figure 2). The cystic artery normally arising from the right
hepatic within the triangle, passes in the triangle toward the neck
of gall bladder where it typically divides into two branches one
of which runs on the attached surface of the gall bladder and the
other on its peritoneal surface [3]. Tortuous right hepatic artery,
running with upward and downward course producing hump is
rarely described anomaly [4]. This tortuosity of the right hepatic
artery is called caterpillar hump or Moynihan’s hump [5]. Both
inside and outside the Calot’s triangle, the right hepatic often
makes a characteristic caterpillar like loop, convexity of which
points downward, upward, to the right or to the left. In cholecystectomy, such tortuosity of the right hepatic is extremely vulnerable, for the cystic artery may arise from the distal or the proximal
end of the loop, in the latter instance crossing it.
The U shaped right hepatic artery has various positions with
reference to the cystic duct.
(A) More nearer the hump to CD shorter will be CA.
(B) The hump can be anterior or posterior to CHD.
(C) Hump can be single loop or double loop
(D) Cystic artery can be single or double (anterior and posterior)
(E) A bend in the course of the right hepatic artery throwing it into the caterpillar hump invites injury unless it is carefully
dissected free [12]. This variant of right hepatic artery invariably
leads to abnormalities of cystic artery formation which can result
in its injury during surgical procedures.
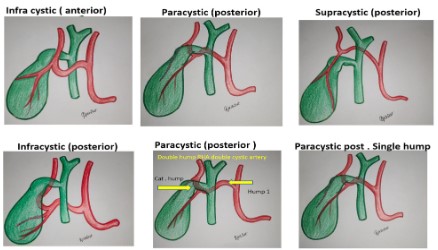
Types of caterpillar hump -Since cystic duct is taken as reference, depending on the anatomical relationship of caterpillar
hump to cystic duct classification of hump is done.
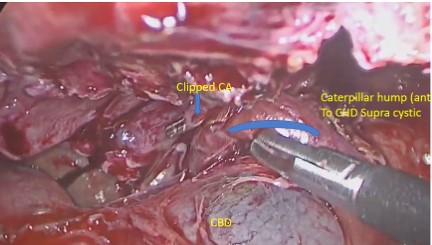
1) Supracystic: The hump is either anterior or posterior to
CHD, superior to the cystic duct, nearer to hilum of liver. Here the
cystic artery is long, originating from inferior part of loop hump.
Due to long cystic artery, and hump remaining away from surgical
dissection, mishaps are less during surgery.
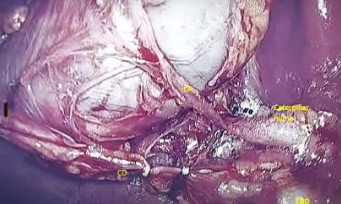
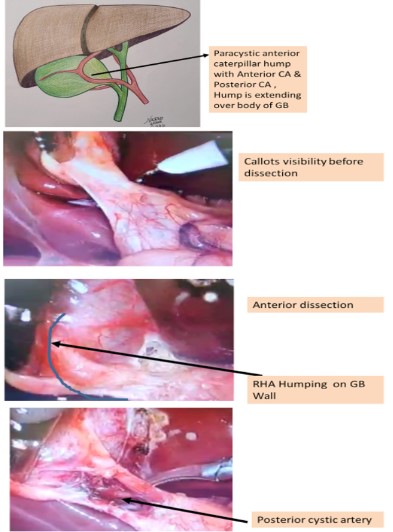
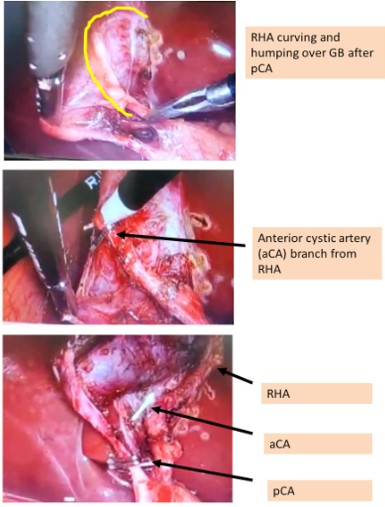
2) Paracystic: The hump is around the confluence of cystic artery and CHD. Here the hump usually gives off two branches, anterior cystic artery and post cystic artery. Since the hump is very
close to cystic duct, the cystic arteries are very short. The hump
(RHA) is mistaken for CA and high chances of vascular catastrophe
during surgery.
3) Infracystic: The hump is below the confluence towards duodenum, here again the CA is long, single, originating from ascending part of hump. Surgical mishaps are less for obvious reason.
Depending on other anatomical details caterpillar hump can
be classified further as follows:
A) Anterior/posterior (loop position in relation to CHD / CBD)
B) Single hump/double hump (depending on number of
hump) [8]
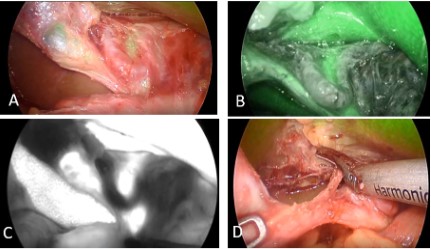
C) Single cystic artery / double cystic artery (Figure 3).
Surgical significance
Variant of right hepatic artery invariably leads to abnormalities of cystic artery formation which can result in its injury during
surgical procedures. Since the cystic artery arising from the loop
is typically short, it may get easily avulsed from the hepatic artery,
if excessive traction is applied to the gall bladder producing brisk
bleeding [24].
Sometimes tortuous right hepatic artery does not give a single
cystic artery but supplies the gall bladder with several small twigs.
The right hepatic artery is injured while securing them. Injury to
right hepatic artery can be fatal in presence of impaired liver function and associated biliary injury [24-26].
It is usually the right hepatic artery that is in danger during this
surgery and must be located before ligating the cystic artery [5].
Because numerous variations in origin and branching pattern of
right hepatic artery have been reported [27].
The Hump lies in close proximity to the gall bladder and cystic
duct and so it may be mistaken to be cystic artery and inadvertently ligated during surgical procedures like cholecystectomy and
liver transplantation [5,7,11,13]. So caterpillar hump should be
suspected when an unusually large ‘cystic artery’ is seen through
the laparoscope [5,12]. It must be emphasized that an artery resembling the cystic artery in its course and paralleling the cystic
duct is not necessarily the cystic artery but may be right hepatic
artery and the calibre of vessels to be divided is not a reliable index of whether it is cystic artery or right hepatic artery. Therefore,
it is essential to visualize right hepatic artery above and below the
origin of cystic branch [28,29].
Accurate knowledge of cystic artery and right hepatic artery
anatomy and its variations can reduce the likelihood of uncontrolled intraoperative bleeding, an important cause of iatrogenic
extra hepatic biliary injury and conversion to open cholecystectomy [29-31]. The incidence of conversion to open surgery due
to vascular injury is reported to be 0-1.9% and its mortality 0.02%
[29], hence these variations should stay in surgical conscience
to prevent procedure related morbidity. We aim to present the
variations in cystic artery seen in laparoscopic cholecystectomy in
our patient population.
Materials and methods
600 videos of laparoscopic surgery of gall bladder and CBD
exploration were retrospectively reviewed for presence of caterpillar hump in RHA in Rahate Surgical Hospital and Seven Star
Hospital, Nagpur, India from 2012 to 2021 April Lot of literature
reviewed. Type of hump and its anatomical relations and difficulty level of laparoscopic surgery because of hump was assessed
21 cases were found to have caterpillar hump. Various types of
humps as per relation with cystic duct defined as follows:
1) Supracystic hump (position of hump superior to cystic duct)
2) Paracystic (position of hump at same level of cystic duct)
3) Infracystic (position of hump below the cystic duct)
Depending on anterior or posterior position of hump in relation to CBD and CHD, hump was further classified as follows:
1) Supracystic: a) anterior, b) posterior
2) Paracystic: a) anterior, b) posterior
3) Infracystic: a) anterior, b) posterior
Further cystic duct number and position defined. A specific relationship between cystic artery number and type of hump was
noted as follows
1) Supracystic and Infracystic hump-only one cystic artery
which divides in to two anterior and posterior cystic arteries. Length of cystic arteries is long
2) Paracystic hump-Anterior and posterior cystic arteries originate separately, that means there are two cystic arteries.
Both cystic arteries are short in length. Hence, chances of
injuring RHA is high in Paracystic caterpillar hump.
Results
Table 1: Incidence percentage of types of caterpillar hump seen in present study (this is a single centre study, we need more multicentric
studies by surgeons and anatomist to know the incidence of caterpillar hump, its various types surgical corelation).
| SR. NUMBER |
TYPE OF HUMP |
ANTERIOR /POSTERIOR |
NUMBER OF CASES |
NUMBER OF CYSTIC ARTERIES |
% |
| 1 |
SUPRACYSTIC |
POSTERIOR |
11 |
One |
52.38 |
| 2 |
SUPRACYSTIC |
ANTERIOR |
2 |
One |
9.524 |
| 3 |
PARACYSTIC |
POSTERIOR |
5 |
Two |
23.809 |
| 4 |
PARACYSTIC |
ANTERIOR |
2 |
Two |
9.524 |
| 5 |
INFRACYSTIC |
POSTERIOR |
1 |
One |
4.762 |
| 6 |
INFRACYSTIC |
ANTERIOR |
NIL |
0 |
0 |
Table 2: Incidence of Caterpillar Hump of RHA in various studies.
| Sr no |
Study author name (cases) |
Year |
Caterpillar hump (%) |
| 1 |
Johnston et .al [8] |
1952 |
2.86% |
| 2 |
Bergamaschi et al [9] |
2000 |
12.90% |
| 3 |
Ayyaz et al. [10] |
2001 |
1% |
| 4 |
Hamza et al. [7] |
2008 |
4% |
| 5 |
Al-Sayigh [11] |
2010 |
4% |
| 6 |
Prithi et al. [12] |
2010 |
1.60% |
| 7 |
Jansirani et al. [5] |
2012 |
5% |
| 8 |
Dawani et al. [1] |
2013 |
5.90% |
| 9 |
Rahate et al [21] |
2021 |
3.50% |
Discussion
Laparoscopic cholecystectomy was initially associated with a
significant increase in morbidity due to increased incidence of biliary injuries and haemorrhages. This was perhaps due to a lack of
knowledge of the ‘laparoscopic anatomy’, two dimensional ‘laparoscopic view’ and the dissection with long instruments without
tactile feedback [29,32]. Misinterpretation of normal anatomy and
anatomical variations contributed to major postoperative complications [33]. Conventional textbook description of the regional
blood supply did not seem adequate in laparoscopic view [34].
With the availability of good optics supported by infrared imaging and improvement in energy sources for dissection, callots
anatomy became increasingly clear and safe. smallest of anatomical details and deviations were recorded.
Similarly, various classifications of cystic artery were proposed
in the literature. Ignjatovic et al [35] described 3 types of cystic artery; Type 1 was described as single artery in Calot’s triangle; Type
2 more than one artery in Calot’s triangle and Type 3 no artery in
Calot’s triangle. Balija et al [36] described two groups; in group 1,
cystic artery, either single or double, was present in the triangle
and in group 2 no artery was seen in the triangle on laparoscopic
visualization. He did not comment on cases where vessels were
seen both inside and outside the Calot’s triangle. Ding et al [29]
in their classification describe 3 groups; Group I have artery/arteries in the triangle, Group II has the artery outside the triangle
and Group III has compound arteries, both inside and outside the
triangle. They also described these arterial variations according
to their origin.
The commonest variation was that of double arteries in Calot’s
triangle in 11.8% patients 1. This pattern has been seen in 15 to
25% of many published series [36,37], but Suzuki has described
this pattern in only 2.45% of his patients [34]. At this point we can
say that multiple cystic arteries in callots are due to Paracystic caterpillar hump which previous workers failed to notice that time.
Balija describes a cystic artery originating from aberrant right
hepatic artery entering the Calot’s triangle from behind the portal
vein and paralleling the cystic duct, occasionally forming a prominence in this area (caterpillar hump). This artery yields multiple
small branches, rather than a single branch, but within the triangle [35].
With increase clarity in discection because of improved optics,
improved technicques and improved energy sources along with
development of infrared imaging, lot of clarity is there about biliary tree and biliary vascular anatomy.
Though we have classified the caterpiller hump variations some
times we come across exaggerated form of the type of hump.
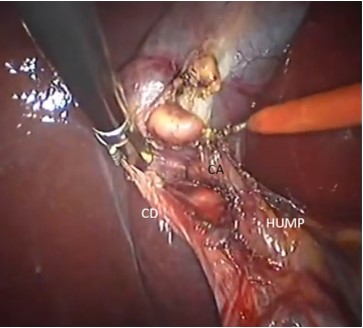
We also discuss here the extended type of caterpiller hump
here.
In one of the case the RHA was forming hump which was extended over body of gall bladder. RHA was having two Cystic arteries as branches; viz. Anterior and posterior cystic arteries.
Conclusion
With increasing incidence of gall bladder and ductal disease,
knowing the vascular anatomy and likelihood of complications
should be known to all surgeons. Ductal anatomy had been extensively studied and documented. Vascular anatomy has been little
neglected, this is an attempt to make surgeons aware of callots
triangle vascular anatomy. So that the surgeons are able to identify this arterial variation during their cholecystectomy surgeries. Potentially precarious RHA in caterpillar hump variation has
been classified and extensively studied for variations of positions
and cystic artery anomalies. The classification has been named
as NAGPUR CLASSIFICATION after the city of origin of the author.
If this caterpillar hump of right hepatic artery is present, the surgeons should locate the origin of cystic artery to avoid any unnecessary confusion between cystic artery and right hepatic artery
for preventing unnecessary damage to the right hepatic artery.
In an attempt to classify caterpillar hump, we can define, predict
position of cystic artery type and variation, thereby helping in preventing vascular complications during laparoscopic cholecystectomy and CBD exploration.
This is single centre observation involving a single surgical
team. This topic needs multi centre analysis with surgeons and
anatomist.
References
- Zubair M, Habib L, Mirza MR, Cnanna MA, Yousuf M, et al. Anatomical variations of cystic artery: telescopic facts. Med J Malaysia.
2012; 67: 494-496.
- Ding YM, Wang B, Wang WX, et al. New classification of the anatomical variations of cystic artery during laparoscopic cholecystectomy. World J Gastroenterol. 2007; 13: 5629-5563.
- Ding YM, Wang B, Wang WX, Wang P, Yan JS, et al. New classification of the anatomical variations of cystic artery during laparoscopic chole cystectomy. World J Gastroenterol. 2007; 13: 5629-5634.
- Hollinshed WH. The Liver and Gall bladder. Anatomy for Surgeons.
The Thorax Abdomen and Pelvis. vol. 2. New York: Harper and
Brothers, 1956; 346-347.
- Jansirani D, Mugunthan N, Phalgunan V, Deep SS. Caterpillar hump
of right hepatic artery: incidence and surgical significance. Natl J
Clin Anat. 2012; 1: 121-124.
- Michels NA. Blood Supply and Anatomy of the Upper Abdominal
Organs with Descriptive Atlas. Philadelphia: Lippincott Company.
1955; 171-175.
- Hamza MU, Jaffar AA, Hassan HA, Jasim ZM. Vascular and gall bladder variations in laparoscopic cholecystectomy. Med J Babylon.
2008; 5: 119-130.
- Johnston EV, Anson BJ. Variations in the formation and vascular relationships of bile ducts. Surg Gynecol Obstet. 1952; 94: 669-686.
- Kavitha B. An anatomical study of Moynihan’s hump of right hepatic artery and its surgical importance. J Anat Soc India. 2016.
- Bergamaschi R, Ignjatovic D. More than two structures in Calot’s
triangle: a post-mortem study. Surg Endosc. 2000; 14: 354-357.
- Ayyaz M, Fatima T, Ahmed G. Arterial anatomy in Calot’s triangle
as viewed through the laparoscope. Ann King Edward Med Coll.
2001; 7: 183-185.
- Al-Sayigh HA. The incidence of cystic artery variation during laparoscopic surgery. Med J Babylon. 2010; 7: 389-403.
- Mishall PL, Rajgopal L. Variant right hepatic artery forming Moynihan’s hump – clinical relevance. Int J Anat Var. 2010; 3: 144-145.
- Bhargava GS, Singh H, Singh HD, et al. Moynihan’s hump of right
hepatic artery: a case report and surgical significance. CIBTech J
Surg. 2014; 3: 42-44.
- Bagadabettu SN, Sirasanagandha SR, Kumar N, Shetty SD, et al.
Hepatosplenic trunk associated with tortuous course of right
hepatic artery forming caterpillar hump. N Am J Med Sci. 2012;
4:376-4378.
- Bulut T, Yamaner S, Bugra D, Akyuz A, Acarli K, et al. False aneurysm of the hepatic artery after laparoscopic cholecystectomy.
Acta Chir Belg. 2002; 102: 459-463.
- Alves A, Farges O, Nicolet J, Watrin T, Sauvanet A, Belghiti J. Incidence and consequence of an hepatic artery injury in patients with
post cholecystectomy bile duct strictures. Ann Surg. 2003; 238: 93-96.
- Schmidt SC, Settmacher U, Langrehr JM, Neuhaus P: Management
and outcome of patients with combined bile duct and hepatic arterial injuries after laparoscopic cholecystectomy. Surgery. 2004;
135: 613-618.
- Halasz NA: Cholecystectomy and hepatic artery injury. Arch Surg.
1991; 126: 137-138.
- Chapman WC, Halevy A, Blumgart LH, Benjamin IS: Post-cholecystectomy bile duct strictures: management and outcome in 130 patients. Arch Surg. 1995; 130: 597-604.
- Deziel DJ, Millikan KW, Economou SG Doolas A, Ko ST, Airan MC.
Complications of laparoscopic chomesystectomy: a national survey of 4,292 hospials and an analysis of 77,704 cases. Am J Surg.
1993; 165: 9-14.
- Bismuth H. How to treat a postoperative stenosis? in Bismuth H,
Lazorthes F (eds): Operative Injury of the Common Bile Duct. Paris,
Masson. 1981; 47-107.
- Nicholson T, Travis S, Ettles D, Dyet J, Sedman P, et al. Hepatic artery angiography and embolization for haemobilia following laparoscopic cholecystectomy. Cardiovasc Intervent Radiol. 1999; 22:
20.
- Connor S, Garden OJ. Bile duct injury in the era of laparoscopic
cholecystectomy. Br J Surg. 2006; 93: 158-168.
- Frilling A, Li J, Weber F, Frubauf NR, Engel J, et al. Major bile duct
injuries after laparoscopic cholecystectomy: a tertiary center experience. J Gastrointest Surg. 2004; 8: 679-685.
- Mishall PL, Rajgopal L. Variant right hepatic artery forming Moynihan’s hump – clinical relevance. Int J Anat Var. 2010; 3:144-145.
- Bhargava GS, Singh H, Singh HD, et al. Moynihan’s hump of right
hepatic artery: a case report and surgical significance. CIBTech J
Surg. 2014; 3: 42-44.
- IKeith L. Moore, clinically oriented anatomy, 6th edition, 2009;
287-288.
- Ding YM, Wang B, Wang WX, Wang P, Yan JS.Variant right hepatic
artery forming Moynihan’s hump: clinical relevance,
- New classification of the anatomic variations of cystic artery during laparoscopic cholecystectomy. World J Gastroenterol. 2007;
13: 5629-5634.
- Vishnumaya G, Potu BK, Gorantia VR, Thejodhar P. Anomalous origin of cystic artery from gastroduodenal artery- A case report. Int J
Morphol. 2008
- Tebala GD, Innocenti P, Ciani R , Zumbo A , Fonsi GB, Bellini P, et al.
Identification of gallbladder pedicle anatomy during laparoscopic
cholecystectomy. Chir Ital. 2004; 56: 389-926.
- Nagral S. Anatomy relevant to cholecystectomy. J Min Access Surg.
2005; 1: 53-58.
- Suzuki M , Akaishi S, Rikiyama T, Naitoh T, Rahman MM, Matsuno
S. Laparoscopic cholecystectomy, Calot’s triangle, and variations in
cystic arterial supply. Surg Endosc. 2000; 14: 141-144.
- Ignjatovic D, Zivanovic V, Vasic G, Kovacevic-McilwaineI. Cystic artery anatomy characteristics in minimally invasive surgical procedures. Acta Chir Iugosl. 2006; 53: 63-66.
- Balija M, Huis M, Nikolic V, Stulhofer M. Laparoscopic visualization
of the cystic artery anatomy. World J Surg. 1999; 23: 703-707.
- Hugh TB, Kelly MD, Li B. Laparoscopic anatomy of the cystic artery.
Am J Surg. 1992; 163: 593-595.