Introduction
Neonatal abdominal surgical emergencies include acquired or
congenital conditions of the digestive tract of newborns, which
manifest themselves from birth to the end of the first month of life
(0 to 28 days). These are abnormalities of structures or functions.
It is the most common surgical emergency in newborns [1,2].
Some emergencies are obvious from birth, making diagnosis easy.
However, others are revealed later, making the diagnostic process
requiring more in-depth conditioning and assessments. The
antenatal diagnosis has completely changed the behavior to adopt
[2]. In developed countries, screening and early management
of malformations in newborns have markedly improved their
prognosis [3]. In our countries, mortality is still high because of
the delay in diagnosis, and the low socio-economic level of our populations [4]. They are responsible for 20 to 30% of the causes
of infant mortality in the countries of the European community
[5,6]. In Mali in 2003 Barry. A et al found a mortality rate of
50% [7]. The aim of this work is to study the therapeutic and
evolutionary aspects of neonatal abdominal surgical emergencies
in the pediatric surgery department of the Mali hospital.
Materials and methods
This was a retro-prospective and descriptive study that took
place over three years from June 1, 2018 to May 31, 2021.
This study was carried out in the pediatric surgery department
of Mali hospital. All neonates aged 1 to 28 days hospitalized
for emergency neonatal abdominal surgery during the study
period were included. The parameters studied are: surgical
treatment, outcome of newborns, causes of death and length
of hospitalization. Data were entered and analyzed using SPSS
software version 25.0, Epic Info TM 7.lnk.
Results
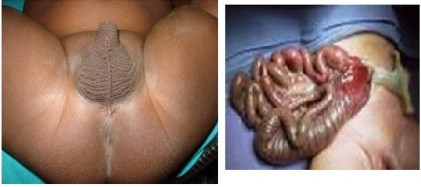
Anorectic malformations represented 51.7% followed by
laparoschisis 25.8% as recorded in (Table 1).
Table 1: Distribution of patients according to the pathologies
encountered.
| Pathology |
Workforce |
Percentage |
| TUE |
16 |
51.7% |
| Laparoschisis |
8 |
25.8% |
| Omphalocele |
3 |
9.7% |
| Hirschsprung's disease |
1 |
3.2% |
| Bad intestinal rotation |
1 |
3.2% |
| Hail atresia |
1 |
3.2% |
| Duodenal atresia |
1 |
3.2% |
| Total |
31 |
100% |
Group I: Intermittent Group; Group C: Continuous Group; SD: standard deviation.
The average treatment time was 48 hours with extremes of 1
and 7 days In our series, 44.5% were operated on within the first
24 hours of their admissions, 33.3% were operated on within 24-48 within hours of their admission and 22.2% were operated on
more than 72 hours after their admissions. Surgical treatment was
performed in 87.1%. All anorectal malformations benefited from
three-step surgery, namely colostomy, anoplasty and restoration
of digestive continuity. Gastroschisis, on the other hand, benefited from single-stage surgery. The omphaloceles were treated in two stages: tanning and then the disemboweling treatment.
Hirschsprung's disease benefited from a colostomy, intestinal
malrotation, duodenal atresia and small bowel atresia were operated on at one time. The complications recorded were respiratory
distress 76.5% followed by infection 17.6% and finally hemorrhage 5.9%. The mortality rate was 54.8%. Among the deaths are
all gastroschisis, 5 anorectal malformations, 1 small bowel atresia,
1 omphalocele, Hirschsprung's disease and intestinal malrotation.
The average hospital stay was 2.39 days with extremes of 1 and
45 days. At 15 months of follow-up, the evolution is marked in 3 of
our patients with anorectal malformations by an anal bud.
Discussions
The digestive surgical pathologies of the newborn have a
character of surgical emergency. The need for surgery as soon as
possible is therefore essential. In our study, 15 cases out of 31,
or 55.5%, were operated on within more than 48 hours of their
admission. The reasons for this delay in the surgical intervention
can be explained by the clinical state of the patients very altered
at their admission requiring intensive preoperative resuscitation,
the delay of an accurate diagnosis, the poverty of the parents who
must assume all the costs medical and treatment costs. These
same observations were made by Randriamizao in Madagascar
[8] who finds in his series, an average time between admission
and intervention of 44.6 ± 12.3 hours. In addition, they advanced
the same reasons for the delay in surgical treatment. The delay
in surgical treatment and the occurrence of complications prolonged the length of stay for some patients. The average length of
stay was 2.39 days with extremes of 1 and 45 days, 13 cases out of
31 so 41.9% progressed favorably towards healing against 18/31
(58%) of newborns who presented at least one complication either pre or postoperatively. Respiratory distress was the most
common complication with 10 cases out of 18, or 55.5% of cases.
All these respiratory distresses occurred in the immediate postoperative period, which made us suspect a problem of postoperative
resuscitation. Sepsis in 3 cases out of 18, i.e. 16.6% of cases Bleeding was encountered in 5.6% of cases (1/18) and was digestive.
These results corroborate with those found by Barry. A al in Mali
[7]. The fatality rate of neonatal digestive surgical emergencies in
our series is 54.8%. This rate is close to that of African countries,
which varies between 50 and 70%, and much higher than that of
developed countries, where it is 4 to 7% [9,10]. The delay in the
consultation by the ignorance of these pathologies, the absence
of neonatal resuscitation service, the non-respect of the prenatal
follow-up schedule, the absence of the antenatal screening were
the factors of poor prognosis.
Conclusion
Neonatal abdominal surgical emergencies constitute an absolute diagnostic and therapeutic emergency characterized by a
particularly high mortality. The prognosis could improve with an
efficient technical platform and qualified personnel.
References
- Fabrice CG. et al. Neonatal surgical emergencies at the provincial
general reference hospital of Bukavu in the Democratic Republic of
Congo. Bukavu: Pan African medical journal. 2016.
- Barry MA. Neonatal digestive surgical pathologies at Gabriel Touré
Hospital; medical thesis. Bamako: FMPOS, 111.
- Cstoll Y; Alembik B Dott ; MP Roth. Risk factors in congenital abdominal wall defect: a study in a series of 265,858 consecutive
births Annales de Génétique Scientific and Medical Editions Elsevier SAS. All rights reserved S00003399501010942/FLA. 2001; 44:
201-208.
- Oludayo A Sowande, Olakayode O Ogundoyin. Pattern and factors
affecting management outcome of neonatal emergency surgery in
lle-lfe, Nigeria Surgical pediatric.2007 ; 11: 71-75.
- Ralahy MF, et al. Neonatal mortality in the emergency department
of the CHU-JRA Antananarivo Madagascar. Review of anesthesia-resuscitation and emergency medicine. 2010; 1(2): 15-17.
- Aguenon AR, Atchade D, Tchaou BA and Goundote. Management
of digestive surgical malformations in children in the multipurpose
anesthesia and intensive care unit. Black Africa Med. 1996; 43(3):
160-163.
- Barry A. Neonatal Digestive Surgical Pathologies At The Gabriel
Toure Hospital [thesis]. [MALI]: USTTB; 2003.
- HMR Randriamizao. Neonatal digestive malformations seen in
the Surgical Resuscitation department of the University Hospital
of Antananarivo. Rev Anesth-Réanim Med Urg Toxicol. 2015; 7(2):
27-33.
- Harouna Y, Tardivel G, Bia M, Abdou I, Gamate Y: Neonatal intestinal obstructions: Our experience about 10 Med cases from Black
Africa. 1997; 44(12): 648-51.
- AR Aguemon, D Atchade, BA Tchou and Pr. Goudote Management
of digestive surgical malformations in children in the multipurpose
anesthesia-resuscitation department. Med of Black Africa: 1996;
43(3).