Introduction
The most common type of abdominal wall hernia is inguinal
hernia, which accounts for about 75% [1]. Amyand’s hernia is the
presence of a normal or inflamed vermiform appendix inside an
inguinal hernia sac. It is named in honour of the surgeon Claudius
Amyand who performed the first appendectomy of an appendix
located in the inguinal canal after a child swallowed a pin causing
appendicitis in 1735 [2]. Amyand’s hernia may be inflamed, incarcerated, perforated or completely healthy. Logan MT [3] reported
that the incidence of appendix as an inguinal hernia sac content is
less than 1%. The diagnosis of Amyand’s hernia is three-fold higher in the pediatric population due to patent precessus vaginalis
[4]. The mortality rate of Amyand’s hernia can reach 30%, most
commonly attributed to peritoneal spread of sepsis [5]. Although
Amyand’s hernia usually occurs on the right side, according to the
normal anatomical position of appendix, it can appear on the left side in situs inversus, gut malrotation and mobile cecum [6]. The
peculiarity of its clinical signs and symptoms together with the
inadequate radiological features of Amyand’s hernia make its diagnosis difficult pre-operatively, it is almost always found intraoperatively.
Case report
An 84 years-old man with underlying gout, hypertension and
benign prostatic hyperplasia presented with painful right inguinal swelling associated with abdominal distension and no bowel
output for 3 days. He denied fever and vomiting. Upon arrival
to the casualty, he was hemodynamically stable. On clinical examination, abdomen was soft, slightly distended. There was an
irreducible right inguinal swelling measuring approximately 4x
4cm, tender on palpation with no skin changes. Bilateral testes
and scrotal examinations were normal. Digital rectal examination was empty. Blood parameters showed no signs of infection,
however his venous blood gas was mildly acidotic. His chest X-ray
was normal. Abdominal X-ray revealed nonspecific large and small
bowel dilatation. He was given adequate fluid resuscitation. With
a preoperative provisional diagnosis of strangulated right inguinal
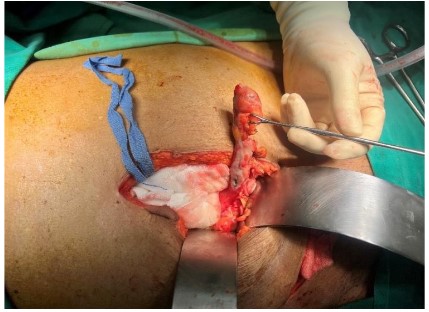
hernia, the patient underwent right inguinal exploration. Intra-operatively noted there was localized seropurulent collection in
the sac with edematous and inflamed appendix. Appendix base
was difficult to visualize, thus proceeded with a lower midline
laparotomy which revealed perforated appendix near its base.
There was no incarceration or adhesion, cord structures were
normal and preserved.
Appendectomy with lavage was done followed by herniotomy and herniorapphy using modified Bassini’s repair. Abdominal and inguinal incisions were closed without mesh placement.
Postoperatively, the patient had an uneventful recovery and was
discharged after 2 days with oral antibiotics. During follow-up a
month later, he was well with no recurrence. Histopathological
examination revealed perforated appendicitis.
Discussion
Many theories have been postulated for the occurrence of
Amyand’s hernia. Long appendix pointing towards the groin, loose
peritoneal reflections and redundant cecum causes the appendix
to reach and gets retained in the hernia sac [7]. The pathophysiology of Amyand’s hernia remains controversial. Studies indicated
that muscle contractions and sudden rise in intrabdominal pressure may compress the appendix in the external ring. This compromises its blood flow resulting in recurrent inflammation and
bacterial overgrowth. Besides that, an extraluminal obstruction
causes edematous appendix due to narrowing of hernia neck [8].
Unlike other inguinal hernia with bowel content, Amyand’s hernia
may appear without signs of obstruction and inflammatory markers stay within normal limits. Various complications may arise
from Amyand’s hernia such as perforated appendix with periappendicular or intraabdominal abscess, necrotizing fascitis of the
anterior abdominal wall, epididymo-orchitis or testicular abscess,
and in- situ arterial thrombosis in rare occurrence [9]. The most
common treatment modality is appendectomy via herniotomy
with primary hernia repair without mesh application. Lower midline laparotomy is advocated in perforation, pelvic abscess or
when other abdominal pathologies are encountered. Laparoscopic appendectomy in case of Amyand’s hernia with appendicitis
was first reported by Vermillion et al [8]. Multiple debates arise as
to whether to remove the appendix if it’s normal and mesh application. While some argued that appendectomy should be done
if evidence of inflammation, others supported appendectomy in
non-inflamed appendix to avoid future complications. The mere
manipulation of a healthy appendix may provoke inflammation
resulting in secondary appendicitis [10-12]. Appendectomy of a
healthy appendix is considered not necessarily beneficial as transection of a fecal-containing organ in a clean surgery increases
septic complications. Besides that, removal of appendiceal lymphoid tissue may compromise the pediatric patient’s immune development [12]. It is generally accepted that the use of mesh in
hernia repair in contaminated wounds is strongly opposed due
to the high risk of surgical site infection. However, several studies
reported the use of mesh repair and adequate antibiotic coverage without infection rate increments [13]. Biosynthetic meshes
may have a role in these, but they are not readily available. Ultimately, the surgical decision is in the surgeon’s hands, the aim
is to have a lower risk of surgical site infection than the risk of
hernia recurrence. This debate led Losanoff and Basson [14] to
propose a classification system for the principal of management
of Amyand’s hernia based on appendix state, presence of abdominal sepsis and concomitant abdominal pathology. Type 1 is a normal appendix in an inguinal hernia, to perform hernia reduction
and mesh placement. Type 2 is acute appendicitis localized in the
hernia sac, to perform appendectomy with primary hernia repair.
Type 3 is acute appendicitis complicated with peritonitis, to perform laparotomy, appendectomy and primary hernia repair. Type
4 is acute appendicitis with concomitant abdominal pathology, its
management is similar as type 3 with management of concomitant disease.
Conclusion
Amyand’s hernia may sometimes lead to serious and life-threatening complications, thus needs to be handled with utmost
vigilance. As it is commonly identified intraoperatively, every surgeon should be prepared to cope with such an unexpected situation and to proceed with the most suitable surgical modality for
an excellent outcome.
References
- Kingsnorth A, LeBlanc K. Hernias: Inguinal and incisional,” The Lancet. 2003; 362: 1561-1571.
- Sengul I., Sengul D, Aribas D. An elective detection of an Amyand’s
hernia with an adhesive caecum to the SAC: Report of a rare case,”
North American Journal of Medical Sciences. 2011; 391-393.
- JM;, L.M.T.N. Amyand’s hernia: A case report of an incarcerated
and perforated appendix within an inguinal hernia and review
of the literature, The American surgeon. U.S. National Library of
Medicine.
- Baldassarre. Amyand’s hernia in Premature twins,” Hernia.
2008;13: 229-230.
- D’Alia C. Amyand’s hernia: Case report and review of the literature,” Hernia. 2003; 7: 89-91.
- R;, G.S.S.R.K. Left-sided Amyand’s hernia, Singapore medical journal. U.S. National Library of Medicine.
- Barut İ, Tarhan ÖR. A rare variation of amyand?s hernia: Gangreneous appendicitis in an incarcerated inguinal hernia sac,” Electronic Journal of General Medicine. 2008; 5: 112-114.
- Solecki R, Matyja A, Milanowski W. Amyand’s hernia: A report of
two cases,” Hernia. 2003; 7: 50-51.
- Desai G, Suhani, Pande P, Thomas S. AMYAND’S HERNIA: OUR
EPERIENCE AND REVIEW OF LITERATURE. Arq Bras Cir Dig. 2017;
30: 287-288.
- PMC5793150.Cankorkmaz L. Amyand’s hernia in the children: A
single center experience,” Surgery. 2010; 147: 140-143.
- Cankorkmaz L. Amyand’s hernia in the children: A single center experience,” Surgery. 2010; 147: 140-143.
- Burgess PL, Brockmeyer JR, Johnson EK. Amyand hernia repaired
with bio-A: A case report and review. Journal of Surgical Education.
2011; 68: 62-66.
- Singal R. An incarcerated appendix: Report of three cases and a
review of the literature,” Hernia. 2010; 16: 91-97.
- Sharma H, Gupta A, Shekhawat NS. Amyand’s hernia: a report of
18 consecutive patients over a 15-year period. Hernia, 2007; 11:
31-35.
- Losanoff JE, Basson MD. Amyand hernia: A classification to improve management,” Hernia. 2008; 12: 325-326.