Introduction
The birth rate by CS has risen steadily in recent decades around
the world. In the United States, CS is the most frequently performed surgical procedure and constitutes 24.1% of the births [1].
In 1985, WHO advocated that national caesarean section rates
should be between 10% and 15% of births, assuming that pregnancy and childbirth are physiological phenomena and that dystocia remains the exception and should not exceed the average rate
of 10%. In 9 Asian countries, the birth rate by caesarean section
was at 27.3%. In 2010, the WHO was alarmed by the increasing
number of caesarean births in China, which was 45%. The recent
increase in CS rate is partly explained by the increase in maternal
age, the prevalence of obesity, multiple pregnancies, and the instances of uterine scarring. New indications, mainly ‘convenience’
cesareans, as well as the increasingly medico-legal constraints,
also contribute to this increased rate.
CS can be performed under General Anesthesia (GA), or Loco
Regional Anesthesia (LRA). LRA is to be favored because it yields
less maternal morbidity and mortality and has become the reference technique for non-urgent and semi-urgent situations [2]. It
includes spinal anesthesia, spinal anesthesia with epidural, and
epidural anesthesia. Spinal anesthesia is the most used anesthesia technique for CS. In fact, more than 95% of CS in the United
States and Canada are done under spinal anesthesia due to its
superiority to the epidural in terms of speed of installation and
efficiency.
As for the GA, its indications consist essentially of the contraindications and failures of the LRA: extreme urgency, abnormal
anatomy of the lumbar region, failure of spinal anesthesia, infection at the point of puncture, hemostasis disorders, unbalanced
intracranial hypertension, hemodynamic instability (especially in
a septic context), and maternal hemorrhage. The refusal of the
LRA by the parturient is also an indication of GA.
The latest report of the 2010 PERINAT survey shows that rates
for GA and LRA for CS in France are 5.8% and 94.2% respectively.
Therefore, it has become the least frequently used anesthesia
technique for CS because it leads to greater maternal morbidity
and mortality [3]. Recent reports point out the negative impact
of GA on fetal central nervous system development and advise
against using it for CS [4].
Our study aims to define indications along with maternal and
fetal outcomes for CS under GA.
Materials and methods
A retrospective descriptive study was conducted. The aim was
to evaluate the practice of CS under GA in our institution, its indications, and its fetal-maternal impacts to improve the care of the
woman and the newborn.
This observational study includes all women who underwent
caesarean delivery under GA at Hôtel-Dieu de France University
hospital in Beirut, between 2011 and 2017. The retrospective
study relies on information retrieval from medical files followed
by data analysis. We determined the incidence of GA during CS,
the maternal characteristics, the indications for CS, the GA indications, and the maternal and fetal complications.
After collecting the data, a descriptive and qualitative analysis
was performed. The results are presented in averages or medians
in cases of asymmetric distribution for quantitative variables and
as percentages for qualitative variables.
This study respects the principles of Helsinki Declaration and
has been approved by the ethics committee of Saint Joseph University in Beirut and is registered as CEHDF-1146.
Results
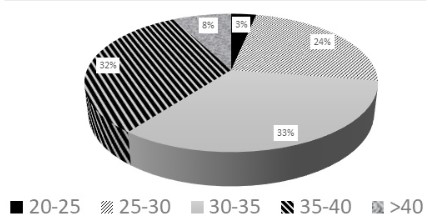
Ninety-one patients were included in the study. The average
age of patients under GA was 33 years old (23-46 years) with a
parity of 3.4 deliveries. 71% of patients had a BMI between 30-40
(Figure 1).
14% of the patients had a medical history, including, mainly,
hematologic problems such as coagulation factor deficiency, thalassemia, thrombotic disease, vasculitis (61%) and hypothyroidism
(15%). Epilepsy, poliomyelitis, and chronic renal failure treated by
transplant were also present.
Only three patients had a surgical history (gastric bypass, endometriosis by laparoscopy and resection of an ovarian cyst).
73% of patients who had a CS under GA suffered from at least
one complication during the pregnancy, listed in Table 1.
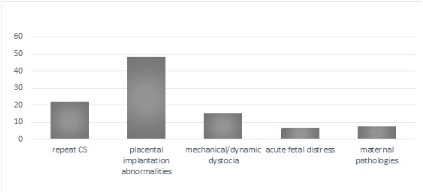
68% of CS under GA were performed before 37 weeks and only
32% were at term. The indications for CS in the studied population are divided into five broad categories (Figure 2). The CS performed under GA constitute 4% of all cesareans in our institution.
45% of the CS were done in a context of an emergency with the
main reason being the failure of LRA. Figure 3 shows the detailed
indications of the GA.
For scheduled CS, the most common indication of GA remained the placental implantation abnormalities requiring the
completion of a hysterectomy. Figure 4 shows the GA indications
for programmed or urgent CS.
64% of patients who underwent CS under GA had no postoperative maternal complications. Only 12% of patients suffered
a serious complication requiring intervention (uncontrollable
bleeding, serious infection, uterine atony). Anesthetic difficulties
were rare (3%) and consisted of two complications (difficulty with
intubation and severe hypothermia).
Admission in the intensive care units for surveillance was reported in 24% of the cases.
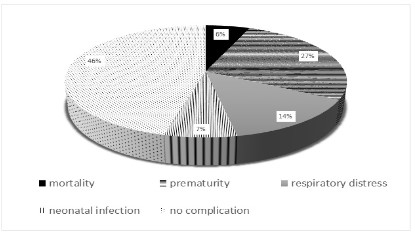
48% of newborns were transferred to the neonatal intensive
care unit for prematurity (27%), neonatal respiratory distress
(14%) and neonatal infection (7%). While 46% of newborns were
reported to not have any complications, 6% of the newborns, unfortunately, died following delivery (Figure 5).
Table 1: Complications occurring during pregnancy in patients
having GA during CS.
| Type |
% |
| Invasive implantation |
44% |
| Vaginal bleeding |
28% |
| Preterm labor |
14% |
| PROM |
12% |
| Urinary infection |
12% |
| Gestational diabetes |
10% |
| Preeclampsia |
7% |
| Amniotic fluid abnormalities |
6% |
| Placental abruption |
4% |
| Fetal anomalies |
4% |
| Hematological complications |
3% |
| Retroplacental Hematoma |
3% |
| Chorioamniotitis |
2% |
Discussion
Cesarean section is a major event in a woman’s life. Using GA is
an additional stressor for her. This mode of anesthesia has its own
risks making the indications a challenging decision. Our institution
is a reference center for pathological deliveries, especially abnormalities of placental implantation, which is the first indication of
CS under GA according to the results of this study. Routine repeat
CS are uniformly done under spinal anesthesia. The corrected rate
of 34%, of CS (not counting the iterative CS) includes a 4% rate of
CS under GA. This value is lower than the rates found in the literature [5]. Compared to such a high rate of CS, a 4% rate of CS under
GA is considered moderate.
Smoking and high blood pressure, which were prevalent in our
study, put patients at increased risk for complications in pregnancies (invasive insertion of the placenta, preeclampsia, placental
abruption) and, thus, at a high risk of an urgent CS [6,7].
The relatively high parity [8] and obesity [9] rates contribute
to the high prevalence of complicated cesareans and placental
implantation abnormalities in our studied population and among
other studies.
Prior medical history is mainly represented by hematologic
problems. However, abnormal blood crease does not systematically increase the indication of CS under GA. In fact, there is lack
of evidence investigating the most appropriate mode of delivery
in this population and the surgeon must rely on his best clinical
judgment to decide on the optimal delivery method [10].
A meta-analysis published in 2016 about maternal mortality
related to anesthesia, has shown that GA by itself is an independent risk factor for maternal mortality [11]. Thus, the GA for CS is a risk factor for maternal mortality, with an additional risk in
urgent situations. However, many of our cases were planned because of the high prevalence of placental implantation abnormalities among our studied population. Our institution is one of the
reference centers for this pathology which explains invasive placentation being the most common indication of CS in the studied
population. Failure of LRA is the second indication of GA in our series and ranks first for urgent CS. It could be explained by the lack
of time required for LRA and the stress of the situation which may
affect the performance of the anesthesia team. Devroe. S and al
found that the lack of clinical experience of the anesthetist and
especially the residents should be considered as an independent
risk factor for perioperative morbidity. Simulation training in highrisk situations would be an interesting way to overcome the rates
of LRA failure in emergent CS [12].
12% of women in the studied population had a serious early
complication related to the intervention. The population characteristics may have an impact on the complications. There is an
established correlation between obesity [13], advanced age [14],
multiparity, smoking [15], hypertension [15], and the occurrence
of post-operative complications and the urgent nature of cesarean section (which occurred in 45% in this series).
Prematurity is the most common neonatal problem and is related mainly to emergency situations, where maternal and fetal
prognosis becomes a priority at the expense of gestational age.
The neonatal respiratory distress is linked to the high rate of preterm birth, the CS itself, and the GA, which is also considered as
an independent factor of neonatal complications. Indeed, studies that compared materno-fetal outcomes between GA and LRA
found a significant .he APGAR score of newborns [16,17]. Similarly, Aiken et al., in a study about the unplanned secondary conversion of LRA to GA, reported a significant delay in the newborn's
breathing [18]. The fetal neurologic impact caused by the anesthetic products used in GA may also be responsible for it [19].
Conclusion
Cesarean section has consistently constantly increased over
the years in parallel to an increase in invasive placental implantations in cases which would lead to a high rate of GA in CS. An
effective collaboration between obstetricians and anesthetists is
required to lower the morbidity and mortality, mainly in emergent situations. Adequate prenatal follow-up of pregnancy could
possibly decrease the rate of emergency indications. Failure of
LRA can be addressed by increasing training and simulation in
high risk situations.
Conflicts of interest: None, the authors declare no competing
interests.
References
- Placeck P, Taffel S. Recent Patterns In Cesarean Delivery In The
United States. Obstet Gynecol Clin North Am. 1988; 15: 607-627.
- Bonnin, B, Fournet F. Anesthesia for Caesarean Delivery: Main
Methods and Indications. Douleur Et Analgesie. 2016; 29: 88-93.
- Afolabi B, Lesi F. Regional Versus General Anesthesia For Caesarean Section. Cochrane Database Syst Rev. 2012; 10: 20-23.
- Sobhy S, Zamora J, Wilson M. Anesthesia-related Maternal Mortality In Low-income And Middle-income Countries: A Systematic
Review And Meta-analysis. The Lancet Global Health. 2016; 4:
320-327.
- Béatrice B, Morgane K. Births In 2010 And Their Evolution Since
2000; Epidemiological Research Unit in Perinatal Health and Children’s Health, 2011.
- Eric J, Sally C. Placenta Accreta Spectrum: Pathophysiology And
Evidence-based Anatomy For Prenatal Ultrasound Imaging. Am J
Obstet Gynecol. 2018; 218: 75-87.
- Fatemeh S, Zahraa M. The Association Between Maternal Smoking
And Placenta Abruption: A Meta-analysis. J Matern Fetal Neonatal
Med. 2017; 30: 1963-1967.
- Cynthia M, Zhuoyang L. Incidence, Risk Factors And Perinatal Outcomes For Placenta Accreta In Australia and New Zealand: A Case control Study. BMJ Open. 2017; 7: 3-4.
- Daniel A, Enquobahrie P. Maternal Pre-pregnancy Body Mass Index And Circulating MicroRNAs In Pregnancy. Obes Res Clin Pract.
2017; 11: 464-474.
- Karanth L, Kanagasabai S. Maternal And Foetal Outcomes Following Natural Vaginal Versus Caesarean Section Delivery In Women
With Bleeding Disorders And Carriers. Cochrane Database of Systematic Reviews. 2017.
- Sobhy S, Zamora J, Dharmarajah K, Arroyo-Manzano D, Wilson M.
Anesthesia-related maternal mortality in low-income and middleincome countries: A systematic review and meta-analysis. Lancet
Glob Health. 2016; 4: 320-327.
- DevroeS,Van de Velde M, Rex S. General Anesthesia For Caesarean
Section. Curr Opin Anaesthesiol. 2015; 28: 240-246.
- Papachatzi E, Paparrodopoulos S. A Pre-pregnancy Maternal Obesity In Greece: A Case-control Analysis. Early Hum Dev. 2016; 93:
57-61.
- Osmundson S, Gould J, Butwick A. Labor Outcome At Extremely
Advanced Maternal Age. Am J Obstet Gynecol. 2014; 3: 362.
- Fatemeh S , Ensiyeh J. Smoking And Placenta Previa: A Meta-analysis. J Matern Fetal Neonatal Med. 2017; 30: 2985-2990.
- Anil I, Özkan O. Comparison Of Maternal And Fetal Outcomes
Among Patients Undergoing Cesarean Section Under General And
Spinal Anesthesia: A Randomized Clinical Trial. Sao Paulo Med J.
2015; 133: 228-230.
- Hoffman M, Hallett V, Carrie C. Fetal And Maternal Outcomes Following Cesarean Hysterectomy: A Comparison Of General vs. Regional Anesthesia. Obst Gyn. 2016; 127: 213-240.
- Aiken C, Bamber H. Maternal And Fetal Outcomes Following Unplanned Conversion To General Anesthetic At Elective Cesarean
Section. J Perinatol. 2015; 35: 695-699.
- Andropoulos D. Effect Of Anesthesia On The Developing Brain: Infant And Fetus. Fetal DiagnTher. 2018; 43: 1-11.