Case presentation
A 80 year old man with a prior history of benign prostatic hyperplasia was referred to neuromuscular clinic for evaluation of 6
months of progressive sensory neuropathy. He developed numbness in his left leg which one week later progressed to involve his
right leg and subsequently ascended over a month to the level
of his groin. On further questioning, he was newly insensate of
bladder and bowel movements requiring weekly suppositories for
bowel movements. He had newly required self-catheterization for
one month. He had absent sensation from his lower waist down
as well as altered perineal sensation. On exam, the patient had
moderate proximal and distal weakness in the bilateral legs and
reduced or absent sensation in the distal legs to vibration, position, and monofilament. Pinprick was absent in the dorsal feet
to the midfoot and posterior legs past the buttocks. Pin prick and
vibration was absent below the level of T10 on his back. His gait
was slow and ataxic requiring a cane.
Diagnosis and assessment
Nerve conduction study and electromyography showed absent bilateral sural sensory responses, normal peroneal and tibial
motor responses, and mild acute on chronic neurogenic changes
in the left gastrocnemius only; this was interpreted as a length-dependent sensory neuropathy and mild S1 radiculopathy with
incomplete reinnervation. MRI of the thoracic and lumbar spine
(Figure 1) showed confluent T2/STIR hyperintensity from the conus medullaris extending through the mid thoracic cord associated with patchy enhancement and serpiginous flow voids posterior
to the spinal cord.
The imaging findings are pathognomonic for a dural arteriovenous fistula (dAVF) with associated myelopathy.
Management
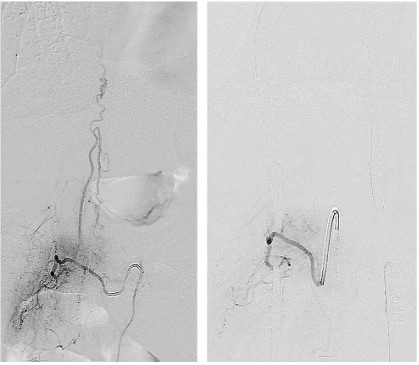
Diagnostic angiogram showed a dAVF supplied by the right L1
segmental artery with a draining vein (Figure 2, left). The fistula
was ligated following T12-L2 laminectomies. Follow up angiogram
demonstrated obliteration of the spinal dural AV fistula without
early venous drainage (Figure 2, right). Two-month post-operative
imaging showed resolution of serpiginous flow voids, significant
improvement in thoracic spinal cord edema (Figure 3), though still
some patchy edema remained in the distal conus medullaris (Figure 4). At follow up, the patient had improved gait, strength, and
sensation. He was able to walk but continued to have perineal
numbness and constipation.
Discussion
Spinal dural AV fistulas are the most common type of vascular
malformation of the spinal cord. Overall, they are still a rare and
reversible cause of progressive para- or tetraplegia. The annual incidence rate is estimated to be 5-10 cases per million [1]. The most
common demographic affected is elderly men. Shunting from a
radiculomeningeal artery into a radicular vein results in increased
spinal venous pressure, congestion of normal spinal veins, and
thus resultant spinal cord edema and dysfunction which are seen
on MRI as a longitudinally extensive area of spinal cord edema,
perimedullary flow voids and dilated vessels, and sometimes spinal cord enhancement. Treatment targets occlusion of the shunt,
either by embolization or neurosurgical ligation. Following successful occlusion of the fistula, symptoms often improve. Presenting symptoms are often nonspecific, and diagnosis hinges on MRI
imaging and diagnostic angiogram. Nevertheless, despite this being a treatable disease, the misdiagnosis rate is as high as 60%
and delayed diagnosis is often associated with poor outcomes [2].
There are two important takeaways to highlight in our case.
First, while cauda equina syndrome is often taught as an acute
presentation and requires emergent evaluation, this presentation
started with only sensory changes, and evolved over the next few
weeks to months into a fulminant cauda equina syndrome picture. Second, initial presenting symptoms of spinal dural AVF are
often nonspecific, and require a high degree of suspicion for accurate and timely diagnosis.
The patient’s clinical syndrome of lower limb weakness, sensory changes, saddle anesthesia, and bowel and bladder incontinence are consistent with cauda equina syndrome. Sensory neuropathy is characterized by often symmetric loss of sensation to
all modalities resulting in a sensory ataxia and loss of balance.
While sensory neuropathy can be rapid and, with severe loss of
proprioception, result in weakness due to inability to activate
muscles, saddle anesthesia and bowel and bladder dysfunction
are red flags for another process.
While most clinicians may be familiar that these red flags are
concerning for cauda equina syndrome, the traditional teaching is
that cauda equina presents acutely and requires emergent evaluation. However, an important feature to note in this case is that
this patient’s presentation started only with sensory changes and
evolved over the next few weeks to months into a fulminant cauda equina syndrome picture. If clinicians are not aware that this
syndrome can present on a more subacute time course, they may
not pursue further investigation into an etiology. In this case, the
patient’s progressive sensory neuropathy was reflective of an insidious process within the spine, namely a spinal dural AV fistula,
that could have been missed had the patient not been seen in
follow-up and had imaging not been pursued.
Spinal dural AVFs have been described to initially mimic a peripheral nerve disorder [3]. Regardless of the level of the fistula,
the caudal spinal cord is the first to be affected, resulting in initially nonspecific sensory and motor symptoms in the feet which
might mimic a polyneuropathy or polyradiculopathy, as was seen
in our case. By the time the classic hallmark of upper motor neuron findings with bowel and bladder dysfunction manifests which
makes the diagnosis clear, patients often are already suffering
from considerable deficits and delay in treatment can result in irreversible handicap.
This case demonstrates the importance of careful follow-up
and attention to progression of symptoms in cases of sensory
neuropathy. Also, while we frequently associate acute neurologic
symptom onset with need for acute management, this is not always the case. Despite a subacute time course with progression of
symptoms over 6 months, this patient had an underlying vascular
etiology that required emergent management. The development
of saddle anesthesia and bowel and bladder dysfunction should
trigger the clinician to expeditiously evaluate the patient for cauda equina syndrome, irrespective of a more indolent time course.
These patients should be immediately referred to neurosurgery
for definitive management. Awareness of these principles demonstrated by this case can help avoid delays in diagnosis which
translate to more negative neurologic outcomes.
Declarations
Funding: This case report received no funding.
Declaration of interest: The authors declare that they have
no known competing financial interests or personal relationships
that could have appeared to influence the work reported in this
paper.
References
- Koch C. Spinal dural arteriovenous fistula. Curr Opin Neurol. 2006;
19: 69-75.
- Ronald AA, Yao B, Winkelman RD, Piraino D, Masaryk TJ, et al. Spinal Dural Arteriovenous Fistula: Diagnosis, Outcomes, and Prognostic Factors. World Neurosurg. 2020; 144: e306-e315.
- Jellema, K et al. “Spinal dural arteriovenous fistulas: a congestive myelopathy that initially mimics a peripheral nerve disorder.”
Brain: A journal of neurology. 2006; 129: 3150-3164.