Introduction
Sebaceous hyperplasia is a benign condition that can be divided into two types, premature sebaceous hyperplasia and senile
sebaceous hyperplasia, depending on the age of the patient at
onset. Premature sebaceous hyperplasia is rare and easily misdiagnosed at the point of initial examination. Patients have an early
age of onset, mainly around puberty, and usually present with
small (<10 mm) papules (which can be partially umbilicated), or
in rare cases, fused and/or (papules >10 mm in diameter) linearly
distributed plaques, etc., the disease needs to be differentiated
from sebaceous nevus.
In this article, we detail a case of a large patchy, heterochromatic premature sebaceous hyperplasia, that occurred on the
face of a patient.
Case presentation
A 38-year-old male patient presented to our office complaining
of papules on the face, which we observed were also distributed
over the neck. These lesions had been getting progressively worse
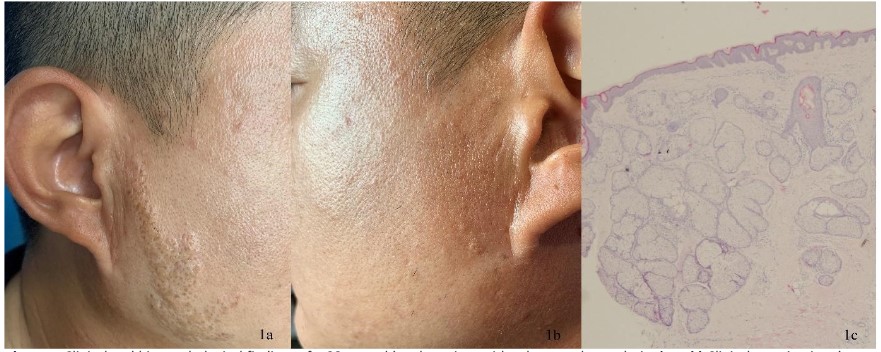
over a period of 28 years, but without any other symptoms. On
the right side of the face, we observed fused raised plaques which
measured 4 cm and had well-defined borders. Whereas, on the
left side of the face and neck we observed multiple papules which
exhibited an umbilical concave top and measured 2-3 mm (Figure
1a-1b). There was no family history of any similar disease. The session presentation was biopsied and the results were suggestive of
sebaceous gland hyperplasia (Figure 1c). The combination of clinical manifestations and pathology led to the diagnosis of Premature Sebaceous Hyperplasia (PSH). The right plaque lesion was excised in stages, and after one month, no recurrence was observed.
Discussion
PSH was first described by Durpe, in 1980 [1]. The disease has
a genetic susceptibility and an autosomal dominant inheritance
pattern [2]. It was once believed to be more prevalent in men.
However, in more recent years, more female patients have been
diagnosed with PSH, indicating that the disease is influenced by
factors other than hormone levels. Currently, the definitive etiology and mechanism are unknown and more cases are required
for clarification.
The average age of onset is between 12 and 26 years. However, congenital forms have also been reported in patients [3,4],
with Oh et al ., [3] classifying this condition as a misshapen tumour as opposed to PSH. There are also atypical presentations,
such as linear PSH or PSH of fused plaques [5,6]. Our case is the
third reported incidence of a patient presenting with a large,
fused plaque that resembles a sebaceous nevus [3,4]. In addition,
our patient noticed brown spots on the plaque, which is unusual.
On the right facial and cervical papules, as well as the surrounding normal skin, no heterochromatic manifestation was observed.
We consider this somehow due to the inhibition of keratin-forming cells. This is the first reported case. The histology is identical
to that of senile sebaceous hyperplasia but is differentiated from
sebaceous nevus.
PSH is characterized by a largely normal epidermis, with mature sebocytes clustered into clusters of sebaceous glandular lobules and ducts opening to the epidermis. Sebaceous nevus has
mostly hyperplastic epidermis with papillary hyperplasia, dilated
parietal sweat glands and no sebaceous ducts opening to the
epidermis, in addition to possible sebaceous gland hyperplasia.
PSH does not usually require treatment. However, if the papules
appear on the face, some patients opt for removal for aesthetic reasons. Treatment options include surgical excision and oral
treatment with isotretinoin. Claude first proposed isotretinoin for
treating PSH in 1985. He prescribed 40 mg twice per day for 2
weeks, which resulted in the rash disappearing. However, he observed the lesions recurred 3 weeks after the treatment was discontinued [7]. As a result of this, Boonchai investigated a regimen
of topical treatment, using 0.05% isotretinoin gel, and reported
satisfactory results after discontinuation of the drug [2]. In future,
larger studies are needed to demonstrate the potential benefits
of using isotretinoin to treat PSH. Our patient refused treatment
with isotretinoin for personal reasons, so we had to resort to surgical resecting.
In contrast to sebaceous nevi, PSH does not pose a risk of malignancy [8]. Despite this, an early diagnosis is necessary to avoid
unnecessary interventions.
Declarations
Acknowledgement: We thank the patient for allowing us to
take pictures and publish the treatment outcome.
Declaration of patient consent: The authors certify that they
have obtained all appropriate patient consent.
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
References
- Dupre A, Bonafe JL, Lamon R. Functional familial sebaceous hyperplasia of the face. Reverse of the Cunliffe acne-free naevus?
Its inclusion among naevoid sebaceous receptor diseases. Clin Exp
Dermatol. 1980; 5: 203-207.
- Boonchai W, Leenutaphong V. Familial presenile sebaceous gland
hyperplasia. J Am Acad Dermatol. 1997; 36: 120-122.
- Oh ST, Kwon HJ. Premature sebaceous hyperplasia in a neonate.
Pediatr Dermatol. 2007; 24: 443-445.
- Mandal RK, Das A, Chakrabarti I, Agarwal P. Nevoid sebaceous
hyperplasia mistaken as nevus sebaceous: Report of four cases.
Indian J Dermatol Venereol Leprol. 2017; 83: 213-216.
- Ozturk M, Ayhan E, An I, Akman Ilik Z, Kaya Ş. Premature or nevoid
sebaceous hyperplasia? Two case reports of a rare disease. Journal
of cosmetic dermatology. 2021; 20: 835-837.
- Wang Q, Liu JM, Zhang YZ. Premature sebaceous hyperplasia in an
adolescent boy. Pediatr Dermatol. 2011; 28: 198-200.
- Burton CS, Sawchuk WS. Premature sebaceous gland hyperplasia:
Successful treatment with isotretinoin. J Am Acad Dermatol. 1985;
12: 182-184.
- Grimalt R, Ferrando J, Mascaro JM. Premature familial sebaceous
hyperplasia: Successful response to oral isotretinoin in three patients. J Am Acad Dermatol. 1997; 37: 996-998.