Introduction
Blunt trauma of the chest consequent to car accidents can rapidly cause lethal multiple organ injuries.
The rupture of a cardiac chamber, most likely an atrium, following blunt chest trauma leads to immediate death in 80-90% of
the patients [1].
3.2% of the blunt chest traumas present one or more vertebral fractures [2]. The rigidity of the thoracic spine limits injury to
it. When there are thoracic vertebral fractures a large amount of
force has been sustained [3]. However, the combination of cardiac rupture and thoracic spine fractures was previously described
only once in a patient who experienced a complex polytrauma
characterized by rupture of the left atrium, fracture of D6 vertebrae and laceration of the trachea and left mainstem bronchus [4].
In this case a massive hemothorax required an Emergency Department Thoracotomy, whereas the repair of the spine injury
was delayed after the stabilization of vital parameters.
Case report
A 36 years old male was involved in a car accident with his motorcycle. Once he landed on the ground, he was hit directly on the
chest by the motorcycle itself bouncing on the asphalt.
On scene, Glasgow Coma Scale was 6 (Eyes: 3, Verbal: 5, Motor: 6). BP (blood pressure) was 75/50 mmHg, HR (heart rate) 115
bpm (beats per minute), Sat O2 97%, RR (respiratory rate) 25.
Crystalloid fluid infusion was started.
At the Emergency Room, BP was 80/40 mmHg, HR 125 bpm,
Hb (haemoglobin) 11.7 g/dl, Temperature 36.4°C.
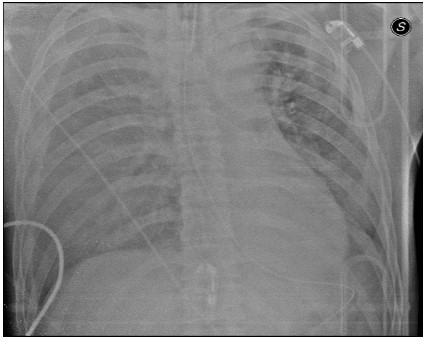
A chest X-Ray demonstrated a bilateral pleural effusion, massive on the right side, and an enlargement of the upper mediastinum (Figure 1). FAST (Focused Assessment with Sonography
for Trauma) confirmed the pleural effusion and demonstrated a
uncomplicated spleen injury. Blood and plasma infusion was initiated.
Due to the instability of vital signs, the patient was sedated and
intubated. A right pleural tube was placed, but due to a massive
blood supply the tube was immediately clamped. We decided to
transfer the patient to the operating room for an urgent thoracotomy. During the transfer to the operating room vital parameters
fell down (PA 50/20 mmHg) and immediately after having entered
the operating room we performed a right antero-lateral thoracotomy in the fifth intercostal space directly on the stretcher, without
even being able to set up the operative field (Figure 2).
After removing blood and clots through a wide pericardial gap,
a 2.5 cm blunt laceration of the right auricle was detected and
clamped with a hemostatic clamp. Blood pressure improved rapidly and the patient slowly recovered an hemodynamic stability. A
sudden cardiac arrest was treated with internal cardiac massage
with an instant recovery of electrical activity. The atrium laceration was stitched and no further cardiac or right thoracic injuries
were found after complete exploration.
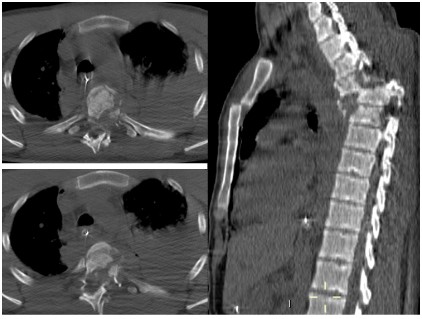
With stabilized vital signs the patient was submitted to a
whole-body CT scan that revealed the following abnormalities:
• Fractures of the left scapula and clavicle
• An uncomplicated spleen injury
• Fractures of D3-D4-D5-D6 with dislocation D4-D5, anterior
dislocation of the body of the sternum, dislocation of the
left costo-transverse articulations from D7 to D10 (Figure 3).
The patient was transferred to the Intensive Care Unit and his
post-operative course was uneventful.
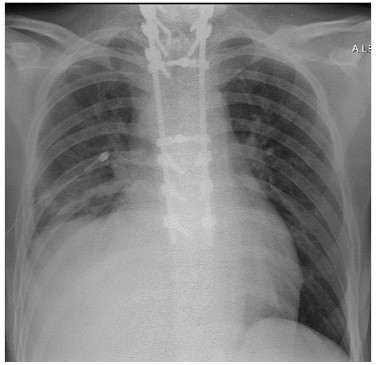
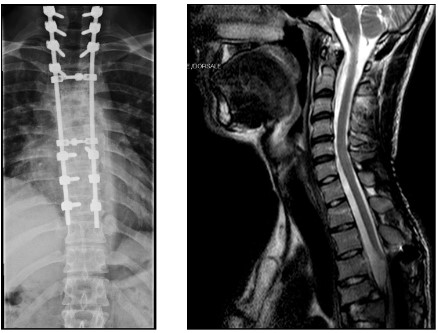
Eight days after the trauma a decompression and posterior fixation C7-D9 were performed (Figure 4). The patient woke up quadriplegic with level C5-C6, with no skeletal lesions. MRI revealed a
wide spinal cord traumatic lesion likely to be both contusive and
vascular, involving the middle of the spinal cord extending from
C5 to D4 (Figure 5).
30 days after the trauma the patient was transferred to the
Rehabilitation Unit with the diagnosis of a level C5 quadriplegia
(ASIA score A) due to a double spinal cord lesion.
At 15 months from surgery, he recovered the use of his upper
limbs (Figure 6), with residual paraplegia level T5, ASIA score A.
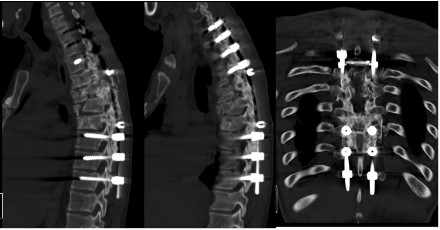
CT follow up shows posterior fusion with poor anterior support
(Figure 7).
Discussion
Patients with cardiac rupture following blunt chest trauma
rarely reach the O.R., as they die in most cases on the scene
or early in the E.R.. The mechanisms of cardiac rupture, in the
present case, was the crushing of the cardiac chambers between
the sternum and the spine [5]. Often, in patients who survive long
enough to be brought to the O.R., small atrial lacerations can be
sutured via median sternotomy or antero-lateral thoracotomy
without the need for cardiopulmonary bypass. Ventricular lacerations, on the contrary, are usually rapidly lethal [6].
The integrity of the pericardial sac is fundamental in the prognosis of patients with cardiac rupture: cardiac tamponade tends
to slow down the blood loss. The minutes earned through the
cardiac tamponade, in fact, may allow the patient to arrive at the
Emergency Room with more treatment options [7]. If the pericardial sac is torn, the primary manifestation of blunt traumatic
cardiac rupture is exsanguinating haemorrhage with massive hemothorax. This generally occurs in a small percentage (10%) of
patients who have an associated pericardial laceration. Mortality
rates are much higher in these patients for lack of the tamponade
effect of the intact pericardium [7].
In the case herein presented an Emergency Department Thoracotomy was performed. The indication was similar to the one with
the best prognosis, namely the deterioration of the clinical condition in the Emergency Department in the presence of an isolated
penetrating cardiac wound [8].
Emergency Department Thoracotomy for resuscitation of the
moribund patient with penetrating cardiovascular injuries was
promulgated by the Ben Taub General Hospital in 1967. Within a
decade, the Denver General Hospital and the San Francisco General Hospital challenged the unbridled enthusiasm for this heroic
procedure and proposed guidelines to minimize futile care. Nowadays the Western Trauma Association designed a multicenter
trial to examine the outcome of resuscitative thoracotomy [9].
Literature reports many cases of right atrium ruptures in thoracic trauma with no mention of associated spine fractures.
The thoracic spine provides a mechanical base of support for
the chest and its contents because it is a rigid structure between
the relatively mobile cervical and lumbar spines. It is capable of
flexion, extension and rotation, but is considerably less mobile
than other parts of the spine. The thoracic spine owes its relative rigidity to its internal structure and to the supporting ribs and sternum. Its rigidity limits injury to it. Conversely, injury to the
thoracic spine implies that a large amount of force has been sustained.
The patient at the time of the first aid showed a paralysis of all
four limbs after the transection of the thoracic spinal cord ischemic injury and contusion of the spinal cord in the cervical-thoracic
transition. Spinal stabilization and physiotherapy treatment have
minimized the cervical damage, allowing the recovery of the upper limbs.
The association of rupture of the right atrium and vertebral
fracture in blunt trauma has not yet been described in literature,
probably because the kinetics of trauma must be of such intensity as to leave no time to rescuers. This is the second case that
we face in a short period of time. In the first case we performed
first an urgent sternotomy for cardiac tamponade and after a few
days a spinal surgical repair. In that specific case, no neurological
sequelae occurred [4] (trauma of lesser intensity?). In the present
casean EDT was performed and delayed spinal surgery allowed
the recovery of motility of the upper limbs. The present case confirms that EDT is advisable in selected blunt trauma.
References
- SJ Khandhar, SB Johnson, JH Calhoon. Overview of Thoracic Trauma in the United States. Thorac Surg Clin. 2007; 17: 1-9.
- S Rajasekaran, RM Kanna, AP Shetty. Management of thoracolumbar spine trauma: An overview. Indian J Orthop. 2015; 49: 72–82.
- Sturm JT, Hines JT, Perry JF. Thoracic spinal fractures and aortic
rupture: a significant ad fatal association. Ann Thorac Surg 1990;
50: 931-933.
- S.N. Forti Parri, G.M. Guiducci, K. Kawamukai, C. Coniglio, G. Gordini, F. De Iure, R. Trisolini, S. Di Saverio, G. Tugnoli. Heart, tracheobronchial and thoracic spine trauma. Succesful multidisciplinar
management. J Acute Desease. 2014; 244-8.
- Richard Embrey. Cardiac Trauma. Thorac Surg Clin. 2007; 17: 87–93.
- T Hakuba, N Minato, T Minematsu, K Kamohara. Surgical management and treatment of a traumatic right atrial rupture. Gen Thorac
Cardiovasc Surg. 2008; 56: 551–554.
- YY Nan, MS Lu, KS Liu, YK Huang, FC Tsai, JJ Chu, PJ Lin. Blunt traumatic cardiac rupture: therapeutic options and outcomes. Injury,
Int. J. Care Injured. 2009; 40: 938–945.
- J.C. Mejia, R.M. Stewart, S.M. Cohn. Emergency Department Thoracotomy. Semin Thorac Cardiovasc Surg. 2008; 20:13-18.
- E. Moore et al. Defining the Limits of Resuscitative Emergency Department Thoracotomy: A contemporary Western Trauma Association Perspective. Journal of Trauma. 2011; 70: 334-339.