Introduction
MRI imaging plays an important role in musculoskeletal infections to allow prompt diagnosis and early treatment. Diffusion
Weighted Imaging (DWI) is an additional pulse sequence that can
be obtained in cases where infection is suspected to enhance the
diagnostic ability of an MRI [1]. DWI sequences are not routinely
obtained during standard imaging and there is a paucity of literature discussing their role in Musculoskeletal infection [2]. We
present a case report which illustrates the benefit of DWI imaging
in diagnosing a challenging case of de novo septic sacroiliitis.
Case report
A 59 year old male presented with pain in the right buttock
area that started rather acutely in relation to a nonspecific injury involving his Right Lower Extremity (RLE). Patient had a sudden
jerky movement of the RLE during a dream and hit his RLE along
the side of his recliner. He could not walk, or weight bear effectively following this incident and tried to take care of it by resting
at home for a few days and eventually presented to the ER by ambulance 3 days later since the symptoms progressively worsened.
The patient had a constant dull throbbing pain in his right buttock
that was non-radiating and aggravated by any movements of the
RLE or weight bearing. The patient denied fevers, chills, loss of
appetite or weight. He denied any intervention in the area in the
past. Patient had a past medical history of Hypertension, Hyperlipidemia, Gastro-esophageal reflux disease and post-traumatic
stress disorder. Patient was a nonsmoker with a history of alcohol
abuse and a remote history of methamphetamine use but denied
any recent use of street drugs.
He was awake, alert, and oriented on examination with no
acute distress. Patient demonstrated exquisite tenderness along
the Right Sacroiliac Joint line inferior end w/o local swelling/
warmth/ erythema over any area. His hip joint line was without
any tenderness to palpation. His affected LE was without any e/o
deformity or limb length discrepancy. Log rolling of the hip was
without any pain. Hip rotations in flexion were painless. Flexion-Abduction-External Rotation and Patrick test reproduced pain.
Patient was able to perform only a limited active straight leg raise.
Passive straight leg raising demonstrated increased pain beyond
70 degrees. Patient was found to be neurovascularly intact on examination.
Patient’s labs showed a white cell count of 9.5 and an ESR
of 55 and CRP of 13.9 on admission. Patient was found to have
positive blood cultures on the day of admission that were later
demonstrated to grow Streptococcus infantarius type II subspecies infantarius. Patient’s ECHO was negative for vegetations or
other abnormalities. His pelvis and hip x-rays were negative for
any abnormalities (Figure 1). Patient was empirically started on iv
Ceftriaxone based on susceptibility testing.
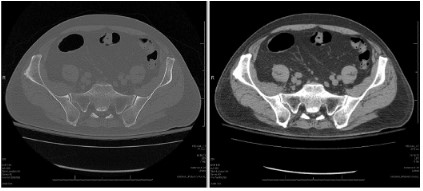
Advanced imaging included CT scans of the pelvis followed by
an MRI. CT Pelvis was w/o any destructive or bony changes at the
R SI joint (Figure 2). No e/o hip effusion/ bony involvement was
found. MRI was w/o remarkable changes that could fully explain
patient presentation. Diffusion weighted images appeared to
show some hyperintense signal in the area around the inferior SI
joint and beneath the iliacus however other series especially the
T2 weighted images did show any correspond images (Figure 3).
The MRI scan was read out as negative for any abnormalities. Due
to correlation of signal changes on diffusion weighted images with
area of TTP and pain on clinical exam as well as a strong clinical
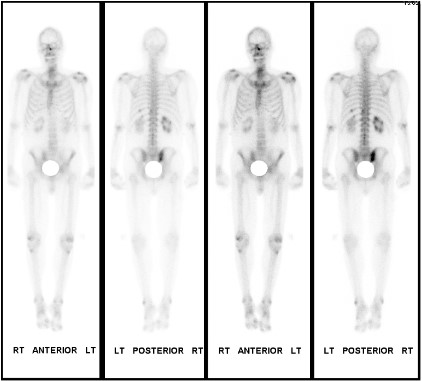
suspicion NM bone scan was ordered as the next step. The bone
scan detected increased perfusion and blood pool activity in the
right sacroiliac joint with increased uptake of Technitium-99m in
the right sacroiliac joint. A diagnosis of Right septic sacroiliitis was
thus established (Figure 4).
Discussion
Accurate diagnosis and prompt treatment is crucial in case of
musculoskeletal infection. MRI imaging has become the mainstay
of MSK imaging with standard imaging including the spin-echo,
proton density, and short tau inversion recovery (STIR) MRI sequences. Routine MRI imaging sequences may not be specific
enough in some instances especially when IV contrast cannot be
given. Diffusion Weighted Imaging (DWI) sequences can provide
the necessary information in such cases and avoid delays in diagnosis [2]. DWI sequences are based on the diffusion of water
molecules at the microscopic level and the relatively impeded
movement of intracellular water compared to extracellular water
provides the differentiation between tissues with high cellularity
versus those with cellular disruption or necrosis. DWI imaging has
some limitations related to artefacts at tissue interfaces or metal
implants and low resolution. Despite these limitations, DWI has
been helpful in diagnosis of vertebral fractures, bone marrow infection, bone marrow malignancy, primary bone, and soft tissue
tumors [1].
A hyperintense signal on DWI sequence is usually associated
with the impeded motion of intracellular water. In this case the
hyperintense signal of purulent material is secondary to its viscosity which impedes the movement of water in an abscess [1]. This
quality of purulent collections can help differentiation of septic
from non-septic effusions, bursitis, and tenosynovitis [2]. Hyperintense signal on DWI can also help differentiate spine infection
from MODIC changes as well as pyomyositis from necrotic tumors
[2]. This modality has a wide variety of application in musculoskeletal infection and its addition to routine imaging sequences when
infection is suspected can enhance the utility of MRI imaging. In
a DWI study the strength and duration of application of diffusion
sensitizing gradients is indicated by their “b-value” and the Apparent Diffusion Coefficient (ADC) is calculated as a measure of tissue
diffusivity. The appearance on high b value and high ADC images is
helpful in differentiating various pathologies. The sensitivity and
specificity of diffusion-weighted images for detecting soft tissue
abscesses has been found to be 92% and 80%, respectively [3].
Noncontrast-enhanced MRI with DWI has comparable diagnostic
performance to contrast-enhanced MRI for diagnosing soft-tissue
abscesses [4]. In an DWI study the strength and duration of application of diffusion sensitizing gradients is indicated by their “b-value” and the Apparent Diffusion Coefficient (ADC) is calculated
as a measure of tissue diffusivity. The appearance on high b value
and high ADC images is helpful in differentiating various pathologies. Infectious Sacroiliitis is a rare disease, with misleading clinical
signs that often delay diagnosis and critical antibiotic treatment
[5]. The disease has a prevalence of only 2–5/100 000 people per
year in the general population and diagnostic imaging is very important in early diagnosis. In the case described above diagnosis
of joint infection was possible only because of DWI images that
were obtained. These images highlighted the hyperintense signal
in and around the sacroiliac joint because of the purulence secondary to the septic joint arthritis. DWI sequences enabled early
diagnosis and prompt treatment of this patient.
Conclusion
Magnetic Resonance Imaging (MRI) with Diffusion Weighted
Imaging (DWI) sequences should be strongly considered during
routine imaging protocols for the detection of sacroiliitis, allowing
early detection and prompt treatment of this rare condition.
References
- Khoo MM, Tyler PA, Saifuddin A, Padhani AR. Diffusion-weighted
imaging (DWI) in musculoskeletal MRI: a critical review. Skelet Radiol. 2011; 40: 665-81.
- Kumar Y, Khaleel M, Boothe E, Awdeh H, Wadhwa V, Chhabra A.
Role of diffusion weighted imaging in musculoskeletal infections:
current perspectives. Eur Radiol. 2017; 27: 414-23.
- Unal O, Koparan HI, Avcu S, Kalender AM, Kisli E. The diagnostic
value of diffusion-weighted magnetic resonance imaging in soft
tissue abscesses. Eur J Radiol. 2011; 77: 490-4.
- Chun CW, Jung JY, Baik JS, Jee WH, Kim SK, Shin SH. Detection of
soft-tissue abscess: comparison of diffusion-weighted imaging to
contrast-enhanced MRI. J Magn Reson Imaging. 2018; 47: 60-8.
- Woytala PJ, Sebastian A, Błach K, Silicki J, Wiland P. Septic arthritis
of the sacroiliac joint. Reumatologia. 2018; 56: 55-8.