Background
Coccidioidomycosis is an endemic fungal infection in arid areas of Southwestern US and Northern Mexico. It is difficult to diagnose and treat, may take years to make the correct diagnosis,
may leave sequelae and could even be fatal. This patient was misdiagnosed and treated for 17 years as synovial chondromatosis.
Coccidioidomycosis frequently mimics other diseases, and a high
index of suspicion is needed to make the correct diagnosis.
Case
A 61-year-old, male, diabetic, Filipino patient presented in
2016 complaining of intermittent right shoulder pain since 1999
and an enlarging mass in right shoulder area since 2002. He was
evaluated at another hospital with MRI and an open biopsy and
diagnosed and treated as Synovial Chondromatosis. He underwent arthroscopic synovectomy and debridement in May 2010.
The operative report mentioned no loose bodies in the GH joint
but hundreds of osseocartilaginous bodies were evacuated from the subacromial space. Because of continuing pain another arthroscopy was done in Nov 2015, for synovial chondromatosis.
Multiple osseocartilaginous bodies were again excised from the
subacromial space.
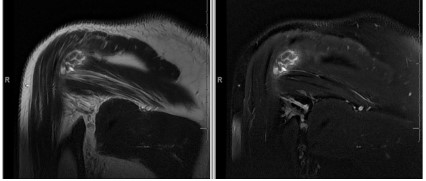
He came to our clinic in July 2016 with continued pain and mild
swelling. X-rays were normal, MRI findings were compatible with
multiple loose bodies and a partial Rotator Cuff tear (Figure 1). Exam showed mild decrease in ROM and mild weakness. There
were no masses, cellulitis, draining sinuses or increased warmth.
He underwent arthroscopy in October 2016 which showed
multiple cartilaginous, pedunculated, and free bodies were found
in the subacromial and subdeltoid space and similar bodies were
detected in the glenohumeral joint which were removed and
sampled for histopathology (Figure 2).
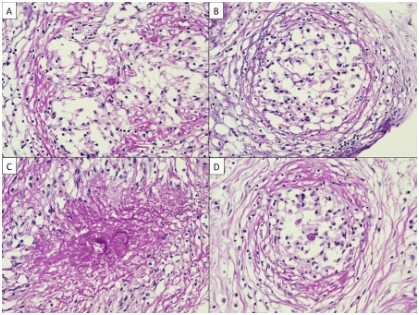
Histopathology sections demonstrated eosinophilic fibrous
nodules, with chronic granulomatous inflammation with multinucleated giant cells. Studies were negative for amyloid, acid fast organisms, foreign body giant cells and cartilage or bone. Gomori’s methenamine and Periodic Acid–Schiff–Diastase (PASD) stains
showed the presence of yeast forms (Figure 3).
The specimen was further studied for fungal identification by
ribosomal focus DNA sequencing using PCR which was positive for
Coccidioides immitis and posadasii [1].
Upon questioning, patient remembered having had an episode
of Coccidioidomycosis in 1994 when he had an upper respiratory
infection with low grade fever, myalgias, cough and positive serology for Cocci. No treatment was given, he was lost to follow-up.
CT of the thorax showed 3.5 cm left upper lung nodule. Bone
scan was negative for any other involvement. He was treated with
Fluconazole 600 mg daily and later with Voriconazole. Serology
remained positive at last follow-up. Repeat MRI showed no recurrence, but patient remains with mild pain and stiffness.
Discussion
Coccidiodes Immitis and Posadasii is a dimorphic fungus that
is found in the soil of arid regions of the Southwest USA, California Central Valley, Northern Mexico, and parts of South America.
It was first reported by Alejandro Posadas, an Argentinian pathologist in 1892. Spores are inhaled during soil disturbances by
earthquakes, dust storms, farming or construction. It is commonly
known as Valley Fever or Desert Rheumatism in the CA Central
Valley.
It is estimated that 80% of persons living in endemic areas become infected within 5 years. It is also estimated that more than
100,000 cases occur annually. Immunocompromised patients are at risk for dissemination as are people from Philippines, Mexico,
African Americans, residents of endemic zones and women in
their 3rd trimester of pregnancy. 60% of the cases may have only
flu like symptoms which resolve spontaneously without treatment, and it is never diagnosed.
The life cycle starts as a mold in the soil with branching septate
hyphae and long filaments. The mold is the least infectious form.
Its growths rapidly in the rainy season and the filaments break off
into arthrospores which become airborne when the dry soil is disturbed. These disarticulate into single rectangular arthroconidia
which are the infective particles which go to the alveoli, become
round and begin the yeast stage of their life cycle. Internal division
starts within 24 to 72 hours; they become filled with thousands of
endospores which are released to form new spherules.
Dissemination occurs in 1% of cases and the most common
sites are the lungs, pleura, lymph nodes and skin. In 10 to 50%
of these cases skeletal infection occurs with osteomyelitis, septic
arthritis, and meningitis. The spine, bony prominences and the
epiphysis of long bones are a frequent site of infection. Recurrences are frequent once the treatment is stopped.
The diagnosis is frequently delayed, and misdiagnosis is common [2-5]. Serology is diagnostic but, in many cases, the definitive
diagnosis is made either by DNA sequencing on biopsy specimen,
I&D of abscesses or aspiration of fluid from the site with fungal
cultures. Complement fixation is usually positive and if greater
than 1:16 indicates dissemination. IgM antibody titers reach the
maximum level at the 3rd week of the disease, can cross react with
other fungal diseases. Serology is negative in about 20 to 25% of
immunocompromised patients.
Articular findings are usually synovitis, effusion, periarticular
bone destruction, osteomyelitis, erosions, and osteopenia [3,5-8].
In our case there were no bony erosions but multiple pedunculated and loose bodies that resembled synovial chondromatosis in
the subacromial space and in the glenohumeral joint.
Infection of synovial tissue has been reported previously in
the knee. Pollock et al reported four cases which showed findings
similar to those in our case, but hyphal forms were not reported
[9]. The presence of hyphal forms of C. immitis in tissue specimens is rare and has been reported in cases of meningitis and
pulmonary infection but reported for the first time in synovial tissue in our case [4,10]. The primary infection is usually not treated
since it is seldom diagnosed and generally is self-limiting with no
residual symptoms. Antifungals such as Fluconazole are usually
recommended for 6 to 12 months and may be recommended for
life in the immunocompromised patient. Amphotericin B is given
IV for disseminated disease and intrathecal for meningitis. Synovectomy, I&D, sequestrectomy, arthrodesis, even amputation is
sometimes necessary.
Conclusion
Coccidioidomycosis is an endemic disease that is rarely diagnosed in its acute phase when it spontaneously resolves as a
flu-like episode. It is also frequently misdiagnosed because it can
mimic other diseases. A high index of suspicion is essential when
there has been exposure in endemic areas. The treatment can be
difficult, and it can frequently recur once medical treatment is discontinued.
Lessons from this case are to get a detailed history, have a high
index of suspicion and always consider cultures of biopsy specimens.
References
- Moncada PA, Budvytiene I, Ho DY, Deresinski SC, Montoya JG,
Banaei N. Utility of DNA sequencing for direct identification of invasive fungi from fresh and formalin-fixed specimens. Am J Clin
Pathol. 2013; 140: 203-8.
- Taxy JB, Kodros S. Musculoskeletal coccidioidomycosis: unusual
sites of disease in a nonendemic area. Am J Clin Pathol. 2005; 124:
693-6.
- Arora NP, Taneja V, ReyesSacin C, Bhanot R, Natesan SK. Coccidioidomycosis masquerading as malignancy. BMJ Case Rep. 2012;
2012: bcr1220115357.
- Kaufman L, Valero G, Padhye AA. Misleading manifestations of
Coccidioides immitis in vivo. J Clin Microbiol. 1998; 36: 3721-3.
- Li YC, Calvert G, Hanrahan CJ, Jones KB, Randall RL. Coccidiomycosis infection of the patella mimicking a neoplasm - two case reports. BMC Med Imaging. 2014; 14: 8.
- Wascher DC, Hartman GP, Salka C, Mertz GJ. Coccidiomycosis presenting as a popliteal cyst. Arthroscopy. 1998; 14: 99-102.
- McConnell MF, Shi A, Lasco TM, Yoon L. Disseminated coccidioidomycosis with multifocal musculoskeletal disease involvement.
Radiol Case Rep. 2017; 12: 141-45.
- TG. A twenty-eight-year-old female with right shoulder pain. New
Jersey Med J Med Soc New Jersey. 2005; 101: 31-6.
- Pollock SF, Morris JM, Murray WR. Coccidioidal synovitis of the
knee. J Bone Joint Surg Am. 1967; 49: 1397-407.
- Kleinschmidt-DeMasters BK, Mazowiecki M, Bonds LA, Cohn DL,
Wilson ML. Coccidioidomycosis meningitis with massive dural and
cerebral venous thrombosis and tissue arthroconidia. Arch Pathol
Lab Med. 2000; 124: 310-4.