Introduction
Spleen is sometimes referred to as the “Neglected organ” because it is always seen on computed tomography (CT) or Magnetic
Resonance Imaging (MRI) scans, but rarely develops disease [1].
In addition, splenic metastases from solid tumors are considered
an exceptional clinical diagnosis and are usually found as part of
a broader metastatic disease. Sclerosing angiomatoid nodular
transformation (SANT) of the spleen, first reported in the literature by Martel et al. [2]. in 2004, is a rare benign non-neoplastic
vascular splenic lesion of uncertain etiology that often masquerades as a potentially malignant entity during the diagnostic process, but surgery remains the only method of diagnosis. In this
paper we report a case of SANT of the spleen operated at our
hospital.
Case report
A 67-year-old female with appropriately managed and monitored AJCC stage II sigmoid colon cancer surgery on 2006, was
newly found to have a splenic incidentaloma on CT of the abdomen and pelvis on 2017. The patient had no previously diagnosed medical conditions other than colon cancer and no family history
of cancer. The patient was treated with six cycles of leucovorin/5-fluorouracil after colon cancer surgery. The patient suffered from
abdominal discomfort approximately two months ago to this visit
and underwent colonoscopy and CT scan. All of her blood tests,
including CEA (carcinoembryonic antigen), were normal. The abdomen was unremarkable except for a low midline laparotomy
scar from a previous open anterior resection for colon cancer.
Colonoscopy and CT revealed no sign of local and systemic tumor
recurrence. However, CT scan with contrast in late arterial phase
demonstrated a pole of spleen (Figure 1). The radiological differential diagnosis was focused on suspected metastatic mass or primary splenic angiosarcoma. Based on this CT finding, the patient
underwent a laparoscopic splenectomy under the diagnosis of
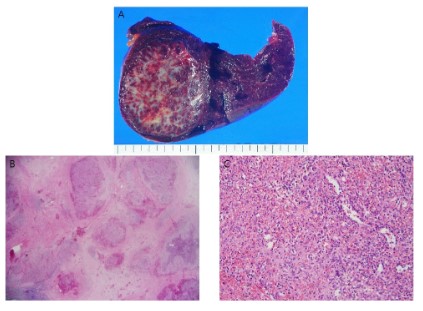
metastatic splenic tumor. This tumor was finally proved by pathological examination to be a SANT of spleen. Macroscopically, the
spleen, measuring 13.0x6.0x5.0 cm, was enlarged by the mass,
which measured 6.0x5.0 cm. The cut surface of the splenic mass
was firm, gritty consistency with variegated appearance (Figure
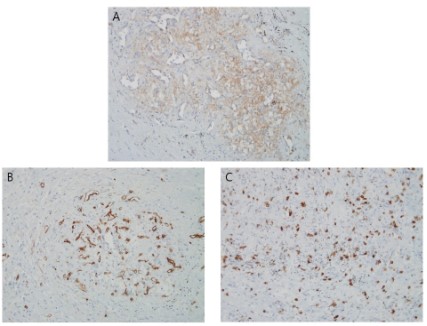
2A). Microscopically, the mass was composed of multiple vascular
structures separated by fibrous connective tissue (Figure 2B and
C) and immunohistochemical analysis revealed positive staining
for CD31, CD34 (Figure 3A and B) and negative for CD8 (Figure 3C)
consistent with diagnosis of a cord capillary-like type of the SANT.
Recovery was satisfactory and the patient was discharged on the
14th postoperative day with no complications.
Discussion
SANT of the spleen is rare, newly recognized, non-neoplastic
vascular lesion of the spleen whose pathogenesis is still uncertain.
It usually found in middle-aged adults, slightly female dominant
but gender bias seems to be vanished and neutralized as more
cases are collected [4]. Most of patients have no clinical symptoms, diagnosed by incidentally during imaging or other medical
procedure of un-related purpose. For symptomatic cases, abdominal pain or discomfort is predominant.
In gross appearance of SANT is solid, well-circumscribed, non-encapsulated nodular lesion distinct from splenic parenchymal.
The pathologic features of SANT is creating the angiomatoid nodules mixture of spindle cells, inflammatory infiltrate, and endothelial vascular proliferations [5]. SANT has three district types of
immunophenotype compared to normal composition of splenic
red pulp [6]. The first one is cord capillary-like type, consists of well-formed cord capillaries in an organized lobular arrangement
in lining endothelial cells, expresses CD34 and CD31 but not for
CD8. The second type, vessel consistent with splenic sinusoids
and include endothelial cells expresses CD31, CD8 but not for
CD34. The third type consists of small veins are arranged complex
mesh like patterns expresses only CD8, not for CD34 and CD31. In
our case, it was compatible cord capillary-like type [7].
The differential diagnosis of splenic mass is various and there
are many benign and malignant lesions. Cystic lesion of the
spleen; congenital true cysts, post-traumatic pseudocyst, etc; can
be identify by imaging modalities with ease. Solid lesion of the
spleen however, have more difficulty in differential, such as hemangioma, hamartoma and angiosarcoma, etc. Hemangiomas of
the spleen can be distinguished from SANT by MRI scan by their
high T2 signal intensity. Hamartomas and angiosarcoma also can
be seen hyper-intensity on T2-weighted images, distinguished
from SANT.
Rachel BL et al. [8]. report characteristic CT and MRI findings
of SANT, including peripheral enhancing radiating lines in arterial
or portal phase, progressive enhancement, hypo-intensity on T2-weighted image, CT scan shows "spoke wheel" pattern, the result
of contrast penetrating the center of the mass from the vascular rim, progressive central enhancement with delayed imaging.
Although there are some notable findings suggest SANT, definite
diagnosis still impossible without tissue diagnosis, especially in
patients who diagnosis malignant disease previously.
SANT of the spleen usually found as incidentaloma, and difficult to diagnosed just by imaging modalities, surgical resection
seems to be necessary eventually. SANT considered as benign,
primary non-neoplastic lesion, Weinreb et al. [9]. report that core
needle biopsy can be used diagnostic option for tissue confirm.
However there is important issue which the risk of intraperitoneal
seeding if the lesion proved by malignant feature, such as metastatic tumors or angiosarcoma. [4] Ruper L et al [10]. report a case of
rapidly growing SANT for 1 year follow-up who underwent anterior resection for stage III rectal cancer. Due to including malignant
pathologic disease in differential diagnosis for SANT, and there is
no reliable radiologic feature has been identified to distinguishing
between these conditions currently, SANT would be diagnosed on
the basis of surgical histopathology for a while.
Conclusion
Most of the patients with pathologically confirmed SANT of
the spleen were asymptomatic preoperatively and thus were usually found incidentally as a splenic incidentaloma prior to surgery
[11]. Unfortunately, there are no definitive diagnostic imaging
methods that can differentiate between SANT and splenic metastases before surgery without pathologic confirmation [12]. Most
of the cancer survivors who incidentally detected splenic mass
prefer to undergo splenectomy due to fear of metastasis. Therefore, to avoid unnecessary psychological stress or splenectomy,
we believe that efforts should be made to perform relatively non-invasive diagnostic methods such as preoperative image-guided
splenic core biopsy. Further research should focus on clinical and
radiological diagnosis of SANT as well as on treatment of patients
with asymptomatic and small findings.
Declarations
Ethics approval and consent to participate: Institutional Ethical committee approved the study. Written informed consent was
obtained from the patient to publish this report in accordance
with the journal’s patient consent policy.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any
accompanying images. A copy of the written consent is available
for review by the Editor-in-Chief of this journal.
Availability of data and materials: Non applicable.
Competing interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or
publication of this article.
Funding: The author(s) received no financial support for the
research, authorship, and/or publication of this article.
Authors and affiliations: Department of General Surgery, Inha University Hospital, Inha University School of Medicine, Incheon
22332, Korea.
Authors' contributions: Moon Suk Choi wrote and revised the
main manuscript. Jihyun Seo prepared the figure. Keon-Young Lee
reviewed the reference. Moon Suk Choi and Sun Keun Choi reviewed all the manuscript.
All authors read and approved the final manuscript.
References
- Giovagnoni A, Giorgi C, Goteri G. Tumours of the spleen.
Cancer Imaging. 2005;5:73-77.
- Martel M, Cheuk W, Lombardi L, Lifschitz-Mercer B, Chan
JK, Rosai J. Sclerosing angiomatoid nodular transformation
(SANT): Report of 25 cases of a distinctive benign splenic
lesion. Am J Surg Pathol. 2004; 28:1268-1279.
- Bamboat ZM, Masiakos PT. Sclerosing angiomatoid nodular
transformation of the spleen in an adolescent with chronic
abdominal pain. J Pediatr Surg. 2010; 45: E13-16.
- Falk GA, Nooli NP, Morris-Stiff G, Plesec TP, Rosenblatt S.
Sclerosing Angiomatoid Nodular Transformation (SANT) of
the spleen: Case report and review of the literature. Int J
Surg Case Rep. 2012; 3: 492-500.
- El Demellawy D, Nasr A, Alowami S. Sclerosing angiomatoid
nodular transformation of the spleen: case report. Pathol
Res Pract. 2009; 205: 289-293.
- Pradhan D, Mohanty SK. Sclerosing angiomatoid nodular
transformation of the spleen. Arch Pathol Lab Med. 2013;
137: 1309-1312.
- Kim HH, Hur YH, Koh YS, et al. Sclerosing angiomatoid nodular transformation of the spleen related to IgG4-associated
disease: report of a case. Surg Today. 2013; 43: 930-936.
- Lewis RB, Lattin GE, Jr., Nandedkar M, Aguilera NS. Sclerosing angiomatoid nodular transformation of the spleen:
CT and MRI features with pathologic correlation. AJR Am J
Roentgenol. 2013; 200: W353-360.
- Weinreb I, Bailey D, Battaglia D, Kennedy M, Perez-Ordonez
B. CD30 and Epstein-Barr virus RNA expression in sclerosing
angiomatoid nodular transformation of spleen. Virchows
Arch. 2007; 451: 73-79.
- Langer R, Dinges J, Dobritz M, et al. Sclerosing angiomatoid
nodular transformation of the spleen presenting as a rapidly
growing tumour in a patient with rectal cancer. BMJ Case
Rep. 2009; 2009.
- Ong BS, Thomas R. Sclerosing Angiomatoid Nodular Transformation (SANT): A Rare Splenic Tumor and Unusual Cause
of Anemia. Am J Case Rep. 2021; 22: e933598.
- Efared B, Sidibe IS, Erregad F, Hammas N, Chbani L, El Fatemi H. Sclerosing angiomatoid nodular transformation of
the spleen (SANT) in a patient with clear cell carcinoma of
the uterus: A case report. J Med Case Rep. 2018; 12 :377.