Introduction
According to the Lancet, the global prevalence of chronic kidney disease is about 11%-13% [1], and there are about 150 million
patients with chronic kidney disease in China, and the retention
of 24h urine specimens for quantitative urinalysis is one of the
mandatory clinical tests for patients with chronic kidney disease
[2]. Properly obtained 24h urine specimens are not only an important indicator to reflect the severity of the disease and predict the
development of the disease, but also provide a scientific basis for
the formulation of treatment plans [3-5]. Therefore, the correct
retention of 24h urine specimens is a key component of quantitative urine protein testing.
The retention time of 24-hour urine specimens is long and the
process is complex [6-8]. This is the main reason why specimens
are prone to get an error testing result. Failure to retain or preserve 24-h urine specimens will directly affect test results, leading
to misdiagnosis as well as inappropriate treatment measures and
increased patient burden [9]. Several studies [10-12] have shown
that the reasons for specimen failure during 24h urine specimen
collection include contamination of the specimen with stool or
blood, failure to drain all urine into the collection device within 24h of specimen collection due to out-of-home examination,
and deterioration of the specimen due to improper placement
of urine; and in clinical practice, there are also problems such as
incorrect recording of urine volume during specimen collection,
inadequate mixing of urine during collection, and spillage of urine
specimens during collection. The traditional 24h urine specimen
collection method also requires the patient to record the urine
volume in a measuring cup after each urination and then pour it
into the urine collection bucket, which not only causes discomfort
to the patient but also pollutes the ward environment, resulting
in poor patient satisfaction with the operation of 24h urine collection. At the same time, the nurses may also have large testing errors due to uneven mixing and inadequate use of test tubes when
collecting 24h urine.
To address these issues, existing studies have focused on improving the specimen retrieval process and developing new urine
specimen retrieval containers. In terms of improving the 24h
urine specimen collection process, the use of quality control circle
tools [13,14], humanistic medicine skills [15], and new teaching
methods, such as the graphic method [16], have been used with
some success. In terms of developing new urine specimen retention containers, Zhang Suyi et al [17] developed a urine specimen
collector for infants and children with a small capacity, and its
scope of application was only for children who had a single urine
test tube specimen retained. The urine specimen collection bag
developed by Ji Huiqin et al. [18] is suitable for the retention of
urine specimens that require the addition of preservatives. Some
scholars have also developed an intelligent visualized 24h urine
specimen collection container, which can solve the problems of
inaccurate urine volume recording and uneven mixing of urine by
manual operation, but it is only applicable to patients who can get
out of bed for toileting and cannot solve the problem of 24h urine
specimen collection for bedridden patients and urine leakage due
to patients going out for examination [19].
In a comprehensive analysis of the above new containers, all
of them have narrow applicability and safety issues to be considered. Therefore, in this study, we developed a new urine collection device and its automatic stirring system consisting of urine
jug, accumulation bag, sampling tube, magnetic stirrer and connecting pipeline, and transformed it into a practical finished product for clinical application, which has the advantages of bedside
urine collection, direct urine volume reading from the accumulation bag scale and automatic urine mixing compared with the
traditional urine specimen retention method. The device has the
advantages of collecting urine at the bedside, reading urine volume directly from the accumulation bag scale and mixing urine
automatically, reducing the steps of manual measuring and mixing, making urine specimen retention more safe, convenient and
clean, and has obtained good application effect in clinical practice.
At present, this device has obtained the national utility model patent (patent No.ZL201920738748.X).
Objects and methods
Subjects one hundred patients admitted to our department
from September 2022 to February 2023 who required 24h urine
protein quantification specimens were selected as study subjects.
Inclusion criteria: ① age≥14 years; ② the patient who need
to keep 24h urine specimens; ③ voluntary participation in this
study. Exclusion criteria:① patients with cognitive or mental
impairment that prevented them from cooperating; ② patients
with urinary and fecal incontinence; ③ those who were allergic
to the contact materials used in this device. The 100 patients who
met the exclusion criteria were divided into a test group and a
control group using the random number table method, with 50
patients in the test group and 50 patients in the control group.
The purpose, procedure and precautions of this study were fully
explained to the patients before the start of the study, and informed consent was obtained from the patients. There was no
statistical difference between the two groups in terms of general
information such as gender, age, education level, disease diagnosis, fall risk assessment, and the ability to take care of themselves
(Activists of Daily Living, ADL) (P>0.05) (Table 1).
Methods
Control group 24h urine specimen collection was performed
using the traditional way of retaining 24h urine specimens. After
the doctor’s order for 24h urine specimen collection, the nurse
in charge gave the patient a warm reminder card for 24h urine
specimen collection and explained the steps and precautions for
collection to the patient or family. The patient prepares the urine
bucket with lid and measuring cup, and stores each urine in the
prepared urine bucket with lid within 24h after the bladder is
emptied at 7:00 AM on the day of specimen collection. The 10 ml
urine specimen was removed from the urine cup and poured into
a urine test tube and sent for testing immediately.
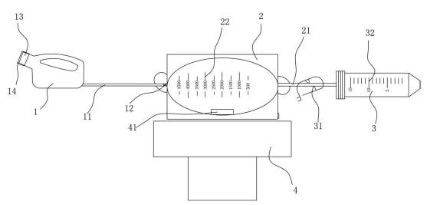
Experimental group: The new urine collection device and its
automatic stirring system (Figure 1), which was researched and
designed by our department, were used for the retention and
sampling of 24h urine specimens: all medical and nursing staff
participating in this study were uniformly trained and familiar
with the specific use of this device and the operation procedure,
and when patients needed to retain 24h urine specimens, nurses
instructed patients on site to use this collection device, with the
following specific operation steps. ① explain to the patient the
function of the device and the purpose of its use; ② instruct the patient to discharge all urine into the accumulation bag through
the urinal interface every time he urinates within 24h after emptying the bladder at 7:00 AM on the day the specimen is retained;
③ discharge the last urine into the device at 7:00 AM the next
day and read the total amount of urine through the accumulation bag scale; ④ place the new urine collection device with 24-hour urine in the automatic stirrer, set a fixed time (15 sec), start
the stirrer, and drive the magnetic rotor of the accumulation bag
to rotate under magnetic force, so that the urine is fully stirred evenly; ⑤ Remove a 10ml urine specimen through the opening
and closing port of the accumulation bag and pour it into a urine
test tube for immediate delivery.
Table 1: Comparison of general information between the two groups.
Items |
Groups |
P-value |
Test group (n=50) |
Control group (n=50) |
Gender |
Male |
29 (58.0%) |
28 (56.0%) |
0.840 |
Female |
21 (42.0%) |
22 (44.0%) |
Education level |
Primary School and below |
15 (30.0%) |
12 (24.0%) |
Junior High School |
13 (26.0%) |
16 (32.0%) |
High School |
10 (20.0%) |
12 (24.0%) |
College / Bachelor |
12 (24.0%) |
9 (18.0%) |
Graduate Student |
0 |
1 (2.0%) |
Diagnosis |
Chronic Nephrotic Syndrome |
27 (54.0%) |
31 (62.0%) |
0.159 |
Hematuria |
1 (2.0%) |
0 |
Acute kidney failure |
1 (2.0%) |
4 (8.0%) |
Chronic Kidney Failure |
10 (20.0%) |
3 (6.0%) |
Chronic kidney disease 5 stage |
9 (18.0%) |
12 (24.0%) |
Fever |
1 (2.0%) |
0 |
Urinary tract infection |
1 (2.0%) |
0 |
Falls risk assessment |
low-risk |
35 (70.0%) |
44 (88.0%) |
0.084 |
mid-risk |
9 (18.0%) |
4 (8.0%) |
high-risk |
6 (12.0%) |
2 (4.0%) |
ADL |
Self Care |
33 (66.0%) |
43 (86.0%) |
0.119 |
Partial self-care |
11 (22.0%) |
5 (10.0%) |
Medium help needed |
5 (10.0%) |
2 (4.0%) |
Needs a lot of help with heavy dependence |
1 (2.0%) |
0 |
Tips: 1: urinal; 2: Accumulation bag; 3: Sampling tube; 4: Magnetic stirrer;
11: First line; 12: Anti-reverse flow design; 13: Urinal interface; 14: Seal
(male urinal for urinal mouth cover, female urinal for urinal mouth plug);
21: Second line; 22: Accumulation bag scale; 31: Switch; 32: Sampling
tube scale; 41: Magnetic rotor.
Evaluation indicators
Qualified rate of 24-hour urine specimen collection The trained
and qualified nurses recorded the qualified situation of 24-hour
urine specimen collection for each of the 2 groups of patients, and
the collected data were statistically analyzed.
Time required to collect 24h urine The time required to automatically mix the urine after collection to collect the urine specimen was recorded separately for each patient, and the collected
data were statistically analyzed.
Patient satisfaction survey of container use. A homemade satisfaction questionnaire was used to collect opinions by means of
a questionnaire star after explaining the evaluation content and
requirements to patients. The content of the satisfaction questionnaire included patient comfort, convenience of use, manipulation of the device, safety of operation and overall evaluation of
the 24h urine specimen retention operation. A five-point Likert
scale [20] was used, with 1 being very dissatisfied, 5 being very
satisfied, and a total score of 4 to 20, the higher the score, the
higher the satisfaction level. The satisfaction questionnaire scores
collected were integrated in the back office and the data were
statistically analyzed.
Statistical methods: The data were entered using Excel 2019 double-checked and statistically analyzed using SPSS 24.0. The t-
test was used to compare the sample means of the two groups,
and the χ-test was used to compare the sample rates of the two
groups. p<0.05 was considered to be statistically different.
Results
In this study, among the 50 patients who collected 24h urine
specimens by the traditional method, 43 specimens (86%) passed
the test, while among the 50 patients who collected 24h urine
specimens using the new urine collection device and its automatic stirring system designed by our department, 49 specimens
(98%) passed the test, and there was a statistical difference in the
passing rate of urine protein specimens between the two groups
of patients (Table 2).
Table 2: Comparison of the passing rate of urine protein specimens retained by the two groups of patients.
Groups |
Urine specimen passing rate |
Test group (n=50) |
43 |
Control group (n=50) |
49 |
P-value |
0.027 |
The time required for 24h urine specimen collection in both
groups, the mean time required for urine specimen collection in
the control group was 68.86 sec; the mean time required for urine
specimen collection in the test group was 43.46 sec, the clinical
time required for two different urine collection methods was significantly better in the test group than in the control group (P<
0.0001) (Table 3).
Table 3: Comparison of the time consumed by nurses collecting specimens in the two groups.
|
Groups |
Cases |
Average time/s |
Standard
deviation |
t |
P-value |
Time consumed by nurses collecting specimens |
Test group |
50 |
43.46 |
1.876 |
-43.471 |
<0.0001 |
Control group |
50 |
68.86 |
3.681 |
Table 4: Comparison of satisfaction of 24h urine specimens retained by patients in both groups.
|
Likert's five-point scale |
Test group |
Control group |
P-value |
Satisfaction with the urine collection device |
strongly approve=5 |
33 (66.0%) |
16 (32.0%) |
<0.0001 |
approve=4 |
16 (32.0%) |
20 (40.0%) |
undecided=3 |
1 (2.0%) |
14 (28.0%) |
disapprove=2 |
0 |
0 |
strongly disapprove=1 |
0 |
0 |
Satisfaction with the convenience of the urine collection device |
strongly approve=5 |
35 (70.0%) |
12 (24.0%) |
<0.0001 |
approve=4 |
14 (28.0%) |
21 (42.0%) |
undecided=3 |
1 (2.0%) |
16 (32.0%) |
disapprove=2 |
0 |
1 (2.0%) |
strongly disapprove=1 |
0 |
0 |
Satisfaction with urine collection device handling |
strongly approve=5 |
34 (68.0%) |
15 (30.0%) |
<0.0001 |
approve=4 |
16 (32.0%) |
20 (40.0%) |
undecided=3 |
0 |
14 (28.0%) |
disapprove=2 |
0 |
1 (2.0%) |
strongly disapprove=1 |
0 |
0 |
satisfied with the comfort of the urine collection device |
strongly approve=5 |
37 (74.0%) |
13 (26.0%) |
<0.0001 |
approve=4 |
13 (26.0%) |
19 (38.0%) |
undecided=3 |
0 |
17 (34.0%) |
disapprove=2 |
0 |
1 (2.0%) |
strongly disapprove=1 |
0 |
0 |
satisfied with the safety of the urine collection device |
strongly approve=5 |
35 (70.0%) |
17 (34.0%) |
<0.0001 |
approve=4 |
14 (28.0%) |
13 (26.0%) |
undecided=3 |
1 (2.0%) |
19 (38.0%) |
disapprove=2 |
0 |
1 (2.0%) |
strongly disapprove=1 |
0 |
0 |
The results showed that patients in the test group were more
satisfied with their comfort, ease of use of the device, ease of
handling of the device, safety of device operation, and overall satisfaction with the 24h urine specimen retrieval operation than the
control group (P<0.0001) (Table 4).
Discussion
Retention of 24h urine specimens for urine quantitative analysis is one of the mandatory clinical tests for patients with chronic
kidney disease [1,2], and the correct retention of 24h urine specimens is a key part of urine quantitative testing [21], which has
important significance for the diagnosis and treatment of clinical
diseases. Studies have shown [22,23] that factors affecting the accuracy of urine specimen test results in clinical practice include
urine specimen storage temperature, storage methods, preservatives, urine collection factors and clinical medication factors, and
errors in test results of 24h urine specimens can lead to misdiagnosis and omission of the condition, cause improper diagnostic and treatment measures, increase the medical burden on patients, and reduce the quality of patient treatment. The results of
this study found that the new urine collection device and its automatic stirring system can improve the qualified rate of patients’
24h urine specimen retention, reduce the error of urine specimen
testing, and improve the accuracy of diagnosis and treatment
compared with the traditional way of 24h urine specimen retention. In a survey of patients’ satisfaction with 24h urine specimen
collection using a homemade satisfaction scale, patients who
used the new urine collection device and its automatic agitation
system for 24h urine collection were significantly more satisfied
with the device and the operation, and the closed nature of the
device itself prevented the spillage of urine during the operation
and the spread of odor during urine collection, which also This
also helps to improve patient satisfaction during hospitalization,
increase patient acceptance of the hospital, and promote the
doctor-patient relationship.
Also, it was found in this study that the time required for nurses
to collect 24h urine was shortened with the use of the new urine
collection device and its automatic agitation system, which improved the clinical efficiency of nurses. During the case collection
process, there was no statistical difference in the fall risk scores
between the two groups, but some of the patients who used the
traditional 24h urine collection responded that they were prone
to the risk of slipping when they went to the toilet at night to
retain urine specimens, so we expect that the improvement of
the 24h urine specimen retention method will improve the safety
of patients during hospitalization and reduce the occurrence of
adverse events of patient falls.
The present study is still deficient in that during the 24h urine
storage period, the delivery time and room temperature changes
can also affect the metabolism of bacteria in urine, thus affecting the urine test results [24]. Free [25] has proposed the idea
of cryopreservation of urine specimens, and some studies have
shown that the urine retention method with a small number of
samples without preservatives at (4±2)°C can completely replace
the traditional method of urine retention [26]. In order to further
improve the effectiveness of the new urine collection device and
its automatic stirring system accumulation bag, and to improve
the accuracy of 24h urine specimen testing, the device can be set up with a temperature-controlled outer bag to maintain the urine
stored in the accumulation bag at (4±2)°C for 24h to ensure the
quality of retained specimens. Therefore, we will modify and upgrade the device later to make it better for clinical use.
Summary
A new type of urine collection device and its automatic stirring
system designed by our department can improve the qualified
rate of 24h urine specimens retained by patients; reduce the time
spent by nurses to collect 24h urine specimens, improve the clinical efficiency of nurses and increase the satisfaction of patients
who have 24h urine specimens retained, which is worth promoting in the clinical application.
Acknowledgements: The authors thank all of the patients analysed in this study. All of the authors have final responsibility for
the decision to submit this manuscript for publication.
Funding: This work was supported by the Guangdong Medical
Science Research Fund [Grant number A2022393].
References
- Hill NR, et al. Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis. PLoS One. 2016; 11: e0158765.
- Ene-Iordache B, et al, Chronic kidney disease and cardiovascular
risk in six regions of the world (ISN-KDDC): A cross-sectional study.
Lancet Glob Health. 2016; 4: e307-19.
- Chang PY, et al, Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine (Baltimore).
2016: 95: e4203.
- Yang DY, et al, Severity of Preoperative Proteinuria is a Risk Factor
for Overall Mortality in Patients Undergoing Nephrectomy. J Urol.
2017; 198: 795-802.
- Koo HS, et al, Analysis of correlation between 24-hour urinary sodium and the degree of blood pressure control in patients with
chronic kidney disease and non-chronic kidney disease. J Korean
Med Sci. 2014; 29: S117-22.
- Shafiee MA, et al. Are individual analyses of multiple short urine
collections throughout the 24 hours superior to a standard 24-hour urine collection in precipitation risk assessment of healthy
subjects? Nephrology (Carlton). 2021; 26: 234-238.
- John KA, et al. Accuracy and Usefulness of Select Methods for Assessing Complete Collection of 24-Hour Urine: A Systematic Review. J Clin Hypertens (Greenwich), 2016; 18: 456-67.
- Ghiraldi EM, LE. Braitman and JI. Friedlander, Factors Associated
With Compliance With 24-Hour Urine Collection. Urology, 2020;
142: 65-69.
- Miler M, A.-M. Šimundić. Low level of adherence to instructions
for 24-hour urine collection among hospital outpatients. Biochemia Medica, 2013: p. 316-320.
- Chan KH, et al. Initial collection of an inadequate 24-hour urine
sample in children does not predict subsequent inadequate collections. J Pediatr Urol, 2019; 15: 74 e1-74 e7.
- Mann SJ, LM Gerber. Addressing the problem of inaccuracy of
measured 24-hour urine collections due to incomplete collection.
J Clin Hypertens (Greenwich). 2019; 21: 1626-1634.
- McGuire BB, et al. Predicting Patients with Inadequate 24- or 48-Hour Urine Collections at Time of Metabolic Stone Evaluation. J
Endourol, 2015; 29: 730-5.
- Karacan C, et al. Evaluation of Urine Collection Methods for the
Diagnosis of Urinary Tract Infection in Children. Medical Principles
and Practice. 2010; 19: 188-191.
- Tosif S. et al. Contamination rates of different urine collection
methods for the diagnosis of urinary tract infections in young children: An observational cohort study. Journal of Paediatrics and
Child Health, 2012; 48: 659-664.
- Boyd C et al. An intervention to increase 24-hour urine collection
compliance. Urology Practice. 2019; 6: 29-33.
- Xiang A, et al. Improving Compliance with 24-H Urine Collections:
Understanding Inadequacies in the Collection Process and Risk
Factors for Poor Compliance. Current Urology Reports. 2021; 22:
38.
- Puntambekar V, Eliza, TP Sinha. A Novel Urine Collection Device
Prototype for Non-Toilet-Trained Male Babies. Indian J Pediatr.
2022; 89: 622.
- Eisinger, S.W., et al., Evaluation of the BD Vacutainer Plus Urine
C&S Preservative Tubes compared with nonpreservative urine
samples stored at 4 degrees C and room temperature. Am J Clin
Pathol. 2013; 140: 306-13.
- Hayward G, et al. Urine collection devices to reduce contamination
in urine samples for diagnosis of uncomplicated UTI: A single-blind
randomised controlled trial in primary care. Br J Gen Pract. 2022;
72: e225-e233.
- Bertram D, Likert scales. Retrieved November; 2007; 2: 1-10.
- Sakuma M, et al. Availability of 24-h urine collection method on
dietary phosphorus intake estimation. Journal of Clinical Biochemistry and Nutrition. 2017; 60: p. 125-129.
- Ohnmacht C et al. Sample stabilization strategies: a case study review of unique sample collection and handling procedures. Bio-analysis. 2019; 11: 1867-1880.
- Peplies J. et al. Influence of sample collection and preanalytical
sample processing on the analyses of biological markers in the
European multicentre study IDEFICS. Int J Obes (Lond). 2011; 35:
S104-12.
- Hedström M, et al. The effect of urine storage temperature and
boric acid preservation on quantitative bacterial culture for diagnosing canine urinary tract infection. BMC Veterinary Research.
2021; 17: 1-8.
- Free HM. Urinalysis in clinical laboratory practice. 2018: Crc Press.
- Jung, CE, et al, Benchmarking urine storage and collection conditions for evaluating the female urinary microbiome. Scientific reports, 2019; 9: 13409.