Introduction
Fungal otitis media (FOM) refers to a type of otitis media in
which fungi are cultured in the contents of mastoid cavity in the
middle ear. It is often complicated with chronic suppurative otitis
media. It is reported that the incidence of FOM is as high as 48.9%
[1]. FOM is often manifested as earache, itching, and purulent ear
discharge [2]. We describe a novel case of nasopharyngeal space
occupying,but it turned out to be FOM.
Case report
A 87-year-old male patient was initially presented to hospital
with a 30-year history of otopyorrhea that aggravated with earache in his left ear for 1 week. An examination revealed that his
left external auditory canal swelled and ached with more purulent
secretion. Computed tomography (CT) of the temporal bone indicated that mastoid air cells, tympanic antrum and tympanum were
filled with the typical appearance of soft tissue mass, while the examination demonstrated no shadow 6 months ago. The initial diagnosis was: 1. Left chronic tympanitis during acute exacerbation
with acute otitis externa; 2. right chronic tympanitis. Antibiotic
therapy was performed with Cefoperazone Sodium and Sulbactam Sodium for two weeks. Then the swelling and aching external
auditory canal was eased, and the purulent secretion significantly
decreased. Two months later, the patient had a headache on the
left side. The headache was expressed in persistent pain. There
was no blood in the snot, blurred vision, nausea, vomiting, neck
mass, limb numbness, and movement disorders. Anodyne was administered to relieve headache, then the patient went to hospital
again after a week. The patient’s past medical history is hypertension treated to be normal and without history of diabetes, coronary heart disease, or history of head injury. No obvious abnormal
changes was demonstrated in general examination. Otolaryngology examination revealed that bilateral external auditory canals
didn’t swell, and there was a little bit purulent secretion in the
left side. Large perforation of right tympanic membrane tension,
no secretion in drum chamber. There are 2 medium sized perforations in the left tympanic tensions arranged back and forth, with a
few white purulent secretions in the tympanic cavity. There is no
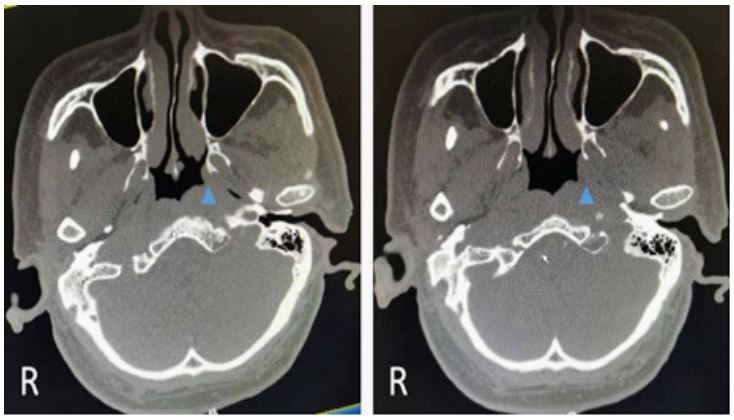
pain, pressured the mastoid and the head. Auxiliary examination:
on CT, scattered shadow existed in the mastoid, tympanic antrum,
and tympanic cavity, which reduced significantly compared with
the results 2 months ago, but the pharyngeal recess disappeared
and bulged out, which showed a typical image of nasopharyngeal
cancer and considered to attribution of nasopharyngeal space occupying lesions. It was postulated to be malignant tumors (Figure
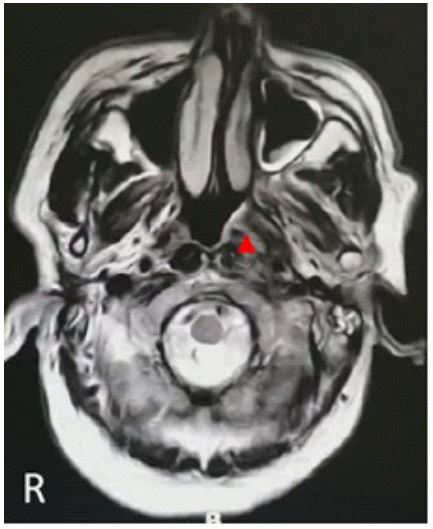
1). Skull base detected by Magnetic Resonance Imaging (MRI) was
demonstrated in Figure 2. The initial diagnosis: 1. Left nasopharyngeal space occupying lesions with undefined nature; 2. Bilateral chronic otitis media. Purulent secretion from the external auditory canal was collected and cultured, the patient was considered
probably to be infected by yeast. A nasopharyngeal biopsy was
performed after local anesthesia with video-naso-pharynogo-laryngoscopes, and the result indicated inflammatory changes, and
repeated test showed the same. The patient was discharged on
Cephalosporin for 1 week, but the headache wasn’t eased. Subsequently, the patient went to the department of otolaryngology
and head surgery at the West China Medical School of Sichuan
University. Considering the possibility of nasopharyngeal cancer, a
nasopharyngeal biopsy was also performed. Inflammatory changes were confirmed in two times of test. Bilateral external auditory canals didn’t swell, and there was a little bit purulent secretion in the left side, large perforation of tympanic membrane in
the right side, and no cancer cells in secretion of the tympanum.
Amoxicillin was administered for 10 days for antibiotic therapy,
but headache wasn’t relieved. The positron emission tomography
and computed tomography (PET/CT) suggested the presence of
inflammation. Purulent secretion from the external auditory canal
was collected and cultured again, the patient was still considered
probably to be infected by yeast. It was assumed to be otitis media infected by epiphyte complicated with osteomyelitis in temporal bones. Antifungal treatment was performed with Voriconazole
for 30 days. After the first day of treatment, the headache disappeared. Headaches didn’t occur any more, and the subsequent
secretion of left external auditory canal were collected for culture
in the course of use and after the medication respectively, neither bacteria nor fungi were found. About one week after the end
of antifungal treatment, the secretions in the left external auditory canal completely disappeared. Endoscopic examination of
bilateral tympanic cavity showed no secretion, granulation tissue
and polyps. Video-naso-pharynogo-laryngoscope revealed that
the nasopharyngeal space occupying vanished, and the pharyngeal recess didn’t bulge out. CT examination of temporal bones
(Figure 3) and skull base detected by MRI (Figure 4) examinations
showed that the nasopharyngeal space occupying disappeared.
Recurrence wasn’t seen in the follow a year.
Discussion
Fungal otitis media: Fungal otitis media (FOM) refers to a type
of otitis media in which fungi are cultured in the contents of mastoid cavity in the middle ear. It is often complicated with chronic
suppurative otitis media. It is reported that the incidence of FOM
is as high as 48.9% [1]. The etiology of FOM may include application of antibiotics and glucocorticoid to chronic suppurative otitis
media, which inhibits sensitive microbes, and then insensitive microbes, such as fungi, take the opportunity to proliferate, which is
also called double infection [3-5]. Repeated recurrence of chronic
otitis media resulting in sebaceous gland injury so that secretion
acidity decreases, which lessens the inhibitory effect on fungi.
Dampness of the external auditory canal is conducive to fungi
growth. Patients’ unhealthy lifestyles such as swabing ears with
unclean items. Lower resistance, and impaired local immunity
caused by increase of age, diabetes mellitus, and glucocorticoid
administration [6].
Clinical manifestations of FOM are repeated recurrence of
ear effusion, external ear eczema, complicated with itching and
otalgia, tinnitus, and hearing loss of various degrees [1]. In recent
years, with the rising of patients with diabetes, hematologic diseases, radiotherapy or chemotherapy, and the widespread administration of glucocorticoids, abuse of broad-spectrum antibiotics, the administration of immunosuppressants, and stuff like that
have resulted in an increasing incidence in fungal otitis media.
Main examination of FOM concludes laboratory identification of the fungus served as gold standard. Commonly used examinations
are fungus microscope examination, fungal culture, histopathological methods, and fungal DNA detected [7,8]. These tests could
aid the diagnosis of fungal diseases. Other tests could be videootic-endoscope which facilitate to see hyphae and plaque in the
ear canal, tympanic membrane and middle ear cavity whose tympanic membrane is perforated. FOM has similar manifestations
with suppurative otitis media on temporal bone CT and ear MRI.
At present, there may be no reports about specific image findings for fungal otitis media. Because the clinical manifestations
of FOM are similar to those of suppurative otitis media, it is difficult to make a definite diagnosis based on clinical manifestations
and physical signs alone, and it is more likely to cause misdiagnosis. However, if otorrhea occurs with protracted course, multiple
treatments and long-term administration of multiple antibiotics
are ineffective, or patients have underlying diseases such as diabetes, it should be predicted that FOM occurs, and it should be
applied that microscopic examination of fugus, fungal culture and
histopathological examination [9].
The experience and lessons of this case: Having a review of
this case: the patient had a long history of chronic otitis media,
the initial diagnosis was chronic tympanitis during acute exacerbation with acute otitis externa, and then the condition improved
after antibiotic treatment, but two months later, non-specific
symptoms of non-chronic suppurative otitis media occurred such
as headaches and neoplasm in nasopharynx. Additionally, it was
considered to be the nasopharyngeal space occupying, not excluding nasopharyngeal cancer because of the high similarity of
its image findings with nasopharyngeal cancer and the patient’s
high-risk factors [10]. However, inflammatory changes were inspected by four pathological biopsies of two 3A grade hospital
and PET/CT examination, and positive fungal culture results were
obtained twice. The final diagnosis was fungal otitis media, and
antifungal therapy was effective, and the long-term follow-up
showed good prognosis.
Why did this patient develop fungal otitis media?
Etiology could be that chronic otitis media caused the alterations of acidic environment of the middle ear and the external auditory canal, and reduced its resistance to fungi, antibiotics were
administered by intravenous drip at hospital for two weeks and
sequentially applied by ear drop for more than one month, which
leading to the inhibition of bacteria and the proliferation of fungi
in the middle ear and temporal bone so that double infection occurred, and the 87-year-old patient had impaired resistance although he did not have basic diseases such as diabetes.
Why wasn’t fungal otitis media early diagnosed?
Reasons could be the antibiotic therapy was initially effective,
the main symptoms at the second visit to hospital are headache
without typical manifestations of FOM such as itching, tinnitus,
earache, and external ear canal eczema, examination indicated
nasopharyngeal space occupation, similarity to nasopharyngeal
cancer, patient’s dwelling in high prevalence area of nasopharyngeal cancer, and the patient’s belonging to high-risk group, and
there are numerous fungi in the nature so that it weakened the
testimonial power of a single positive fungal culture result.
Why did patients have headache and nasopharyngeal space
occupying?
This is how headache and nasopharyngeal space occupying
is developed: long-term chronic otitis media caused middle ear
mucosal injury and fungal infection occurred after repeated antibiotic treatment. Subsequently, the temporal bone osteomyelitis
occurred due to the severe fungal infection, resulting in headache, swelling of the peripheral soft tissue of the temporal bone,
and lymphoid reactive hyperplasia in pharyngeal recess near the
petrous apex, which demonstrated nasopharyngeal recess bulging out on CT, the typical images of nasopharyngeal carcinoma,
causing misdiagnosis probably.
Conclusions
Chronic suppurative otitis media is a common and prevalent
disease in the otolaryngology. If repeated antibiotic treatment is
performed and resistance is impaired, fungal otitis media would
develop, severe fungal otitis media would cause temporal bone
osteomyelitis, and then the temporal bone osteomyelitis would
cause swelling of the peripheral soft tissue of the temporal bone
and lymphoid reactive hyperplasia in pharyngeal recess near the
petrous apex, which manifests as bulging pharyngeal recess in
nasopharynx, especially similar to the nasopharyngeal carcinoma
from endometrium on image. Patients could have headaches for
this disease, which is resembling the symptoms of nasopharyngeal cancer. In clinical practice, it is easy to be misdiagnosed as
nasopharyngeal cancer, and then repeated nasopharynx biopsies would be performed, which would induce patient’s suffering
without definite diagnosis. Under this situation, fungal culture of
secretion in the middle ear should be done, and patient should
be diagnosed as fungal otitis media on the basis of the findings
of PET/CT examination. However, temporal osteomyelitis caused
by fungal otitis media is rare and arduous to diagnose early. Since
temporal osteomyelitis is deep infection, potent antifungal agents
are required based on drug sensitivity assay. The therapeutic regimen is administering voriconazole for 1 month. Consequently, the
advice to strengthen supervision of the antibiotics treatment of
senile patients with chronic otitis media should be proposed.
Multiple culture of secretion should be performed to detect alterations in pathogens early.
Declarations
Conflicts of interest: None. The patient agreed with the publication of the case and provided informed consent for it.
Disclosure: This research did not receive any specific grant
from funding agencies in the public, commercial, or not-for-profit
sectors.
Author contributions: Conceptualization: Da-zhong Y. Data curation: Jing Huang, Da-zhong Y, Feng-bo Y. Resources: Jing Huang,
Feng-jiao L. Supervision: Feng-bo Y. Writing: Jing Huang, Feng-bo
Y.
References
- Talwar P, Chakrabarti A, Kaur P, Pahwa R K, Mittal A, Mehra Y N. Fungal infections of ear with special reference to chronic suppurative otitis media. Mycopathologia. 1988; 104(1): 47-50.
- Punia Rajpal Singh, Singhal Surinder K, Kundu Reetu, Das Arjun, Chander Jagdish. Fungal Suppurative Otitis Media (Histopathology) Among Patients in North India. Head Neck Pathol. 2019; 13(2): 149-153.
- Mittal A, Mann S B, Panda N K, Mehra Y N, Talwar P. Secondary fungal infections in chronic suppurative otitis media. Indian J Otolaryngol Head Neck Surg. 1997; 49(2): 112-6.
- Schrader N, Isaacson G. Fungal otitis externa:its association with fluoroquinolone eardrops. Pediatrics. 2003; 111(5 pt 1): 1123.
- Seelig MS. The role of antibiotics in the pathogenesis of Candida infections. Am J Med. 1966; 40: 887-917.
- Van T A, van R J. Aspergillus mastoiditis, presenting with unexplained progressive otalgia, in an immunocompetent (older) patient. Eur Arch Otorhinolaryngol. 2009; 266(10); 1655-7.
- Kim EJ, Catten MD, Lalwani AK. Detection of fungal DNA in effusion associatedwithacute and serous otitis media. Laryngoscope. 2002; 112(11): 2037-41.
- Catten Md, Murr AH, Goldstein JA, Mhatre AN, Lalwani AK. Detection of fungi in the nasal mucosa using poly merase chain reaction. Laryngoscope. 2001; 111: 399-403.
- Sengupta RP, Kacker SK. Otomycosis. Ind Jn Med Sci. 1978; 32: 5-7.
- Guo R, Mao YP, Tang LL, Chen L, Sun Y, Ma J. The evolution of nasopharyngeal carcinoma staging. Br J Radiol. 2019; 92(1102): 20190244.