Background
Chronic subdural hematoma (CSDH) is a neurological disease
resulting from brain compression, caused by an abnormal collection of liquefied blood degradation underneath the dura mater,
with an overall annual incidence of 1.7-20.6 per 100,000 persons per year, greater in the elderly population [1]. In facts, elderly individuals are more commonly affected by CSDH, with a mortality
rate of 0.5% to 4% and known risk factors are advanced age, therapeutic anticoagulation and mild head injury [2]. The incidence
is expected to double by the year 2030, owing to the continuous
aging of the population [3].
Chronic SDH may be considered as an angiogenic disease
where inflammation plays an important role in hematoma formation.
Histological analysis demonstrates a modified layer of connective tissue cells named “dural border cells” in the dura mater,
which have two essential roles: phagocytosis and the development of a fibro-cellular connective tissue, which may lead to new
membranes as seen in CSDH [4]. A clinical classification, namely
the Markwalder grading score, might help to decide which therapy modality might be more appropriate. However, no consensus
exists about the best treatment for each grade and the treatment
modality [5].
Conservative medical treatment includes corticosteroids, ACEinhibitors, tranexamic acid, platelet activating factor receptor antagonist, and statins [3]. The most commonly practiced surgical
management is the burr hole evacuation procedure with closed
drainage system in the operating theater, however a recent metanalysis found astatistical evidence of similar efficacy and safety
compared to bedside twist-drill drainage of CSDH [6]. Some rare
but severe complications such as intracerebral hemorrhage (ICH)
and acute subdural hematoma (SDH); subarachnoid hemorrhage
(SAH) has recently been reported in some case reports, however
the pathophysiological process underneath its formations has
to be established yet [2,7,8]. Here we present a case report of
a patient with SAH following right fronto-temporo-parietal CSDH
evacuation.
Case presentation
An 86-year-old man was admitted to our emergency department after being found lying on the ground at his home. He had
a minor head trauma two weeks prior that event. His medical
history included an anxiety disorder and a hypokinetic disease.
At neurological examination he was confused and presented hyposthenia of his left upper limb, quantifiable 3/5 of Medical Research Council (MRC) grading system. The routine laboratory tests
and clotting profiles were normal, electrocardiography and chestabdomen-pelvis computed tomography (CT) showed normal
findings. A brain CT scan demonstrated a right fronto-temporoparietal CSDH with a shift of the midline structures and lateral
ventricle compression (Figure 1). The patient underwent a closedsystem drainage of the hematoma via one burr hole located at the
parietal bone protuberance area under local anesthesia in the operating room. After incision of the dura mater, the subdural space
was irrigated with warm physiological saline and closed system
drainage was carefully placed through the burr hole.
He was stable during the operation and the patient’s blood
pressure was well-controlled. However, after two days from the
procedure, the patient suddenly complained a diffuse strong
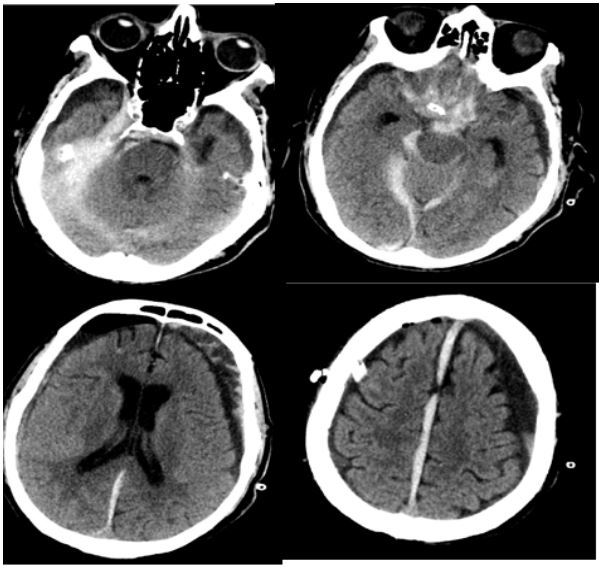
headache. The patient underwent a new head CT scan, which revealed signs of SAH located at the basal cisterns and at the right
sylvian fissure.
Compared to the preoperative image, a marked reduction of
the right lateral ventricle compression and a return to the correct
position by the midline structure occurred (Figure 2). Vascular
malformations were then excluded with a CT angiography (Figure
3).
Conservative treatments, such as osmotic diuretics, hypertonicsaline and hemostatic agents were adopted. Two days later, the
CT scan showed the partial reabsorption of the SAH.
Afterwards, no further symptoms, vasospasm or rebleeding
happened. The clinical course improved, and the patient was
admitted to the neurology unit for close observation. After one
month, the patient fully recovered and was discharged.
Right lateral ventricle compression was markedly reduced, and
the midline structure returned to original position.
Conclusions
Elderly population, due to brain atrophy, suffers frequently
from CSDH, which occurs with a minor head trauma: accumulation of blood clots between the dura mater and the brain surface results from tearing of fragile small blood vessels [7,9]. After
burr hole surgery, which remains a safe and effective treatment
[10]. Postoperative hemorrhagic complications, such as SAH, are
rare but severe. Ogasawara et al. [11] showed that rupture of a
weak subarachnoid vessels and hyperemia take place from rapid
decompression of CSDH and rapid decrease of intracranial pressure, after the drainage of the hematoma. Impaired vascular auto regulation, due to long-term compression by CSDH, and hyperperfusion are possible causes of bleeding [2]. It is possible that
SAH of unknown origin following surgery for CSDH is the result of
sudden cerebral blood flow variation after cerebral decompression, rupture of weaker subarachnoid vessels and perforating arteries, brain shift (12) related to prompt expansion of brain [8].
Diffuse cerebral atrophy, advanced age and consequent cerebral
vascular failure of autoregulation, therapeutic anticoagulation
and other pathologic conditions or individual factors can contribute to development of SAH after CSDH operation [2,7,8]. In our
86-year-old patient, with brain atrophy, a CT scan after surgery
showed SAH; the movement of the hemisphere could have resulted in hemorrhage after the drainage because of sudden decompression. Immediate CT scan is mandatory in the suspect of
such complication. The patient with conservative treatment fully
recovered. Speed of drainage mostly influence on the occurrence
of this potentially devastating complication following evacuation
of CSDH, so we recommend a slow and gradual decompression of
this latter chronic extracerebral fluid collection. We believe, according to relevant literature, that in elderly patients, probably
due to cerebral atrophy, a slow and gradual drainage of CSDH is
needed to avoid a rare but severe complication such as SAH with
a view to minimize change in blood volume and pressure and to
prevent a too rapid or excessive postoperative drainage.
Declarations
Ethics approval and consent to participate: The patient accepted to participate in the following case report.
Consent for publication: Not applicable.
Availability of data and material: Data sharing is not applicable to this article as no datasets were generated or analysed
during the current study.
Competing interests: The authors declare that they have no
competing interests.
Funding: None.
Authors’ contributions: VL selected the case for this report.
DA supervised data collection. AI and OPP wrote the report. MD
performed draft review. All authors read and approved the final
manuscript.
Acknowledgements: Not applicable.
References
- Feghali J, Yang W, Huang J. Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg [Internet]. 2020; 141: 339-45. Available from: https://doi.org/10.1016/j.wneu.2020.06.140.
- Wang G, Yu J. Remote acute subarachnoid hemorrhage after drainage of chronic subdural hematoma: A case report and review of the literature. Int J Surg Case Rep [Internet]. 2018; 44: 202-6. Available from: https://doi.org/10.1016/j.ijscr.2018.02.044.
- Soleman J, Nocera F, Mariani L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med Wkly. 2017; 147(1).
- de Oliveira AJM, Solla DJF, de Oliveira KF, Amaral BS, Andrade AF, Kolias AG, et al. Postoperative neutrophil-to-lymphocyte ratio variation is associated with chronic subdural hematoma recurrence. Neurol Sci. 2021.
- Markwalder TM. The course of chronic subdural hematomas after burr-hole craniostomy with and without closed-system drainage. Neurosurg Clin N Am. 1981; 11(3): 541-6.
- Almenawer SA, Farrokhyar F, Hong C, Alhazzani W, Manoranjan B, Yarascavitch B, et al. Chronic subdural hematoma management: A systematic review and meta-analysis of 34829 patients. Ann Surg. 2014; 259(3): 449-57.
- Seung W-B, Jeong JH. Postoperative Subarachnoid Hemorrhage and Multipunctate Intracerebral Hemorrhages Following Evacuation of Bilateral Chronic Subdural Hematomas. Korean J Neurotrauma. 2017; 13(2): 149.
- Miyazaki T, Matsumoto Y, Ohta F, Daisu M, Moritake K. A case of unknown origin subarachnoid hemorrhage immediately following drainage for chronic subdural hematoma. Kurume Med J. 2004; 51(2): 163-7.
- V Adhiyaman, M Asghar, K N Ganeshram BKB. Chronic subdural haematoma in the elderly. Brain Spine Surg Elder. 2002; (3): 353-71.
- Jang K-M, Kwon J-T, Hwang S-N, Park Y-S, Nam T-K. Comparison of the Outcomes and Recurrence with Three Surgical Techniques for Chronic Subdural Hematoma: Single, Double Burr Hole, and Double Burr 55 Hole Drainage with Irrigation. Korean J Neurotrauma. 2015; 11(2): 75.
- Ogasawara K, Ogawa A, Okuguchi T, Kobayashi M, Suzuki M, Yoshimoto T, et al. Postoperativ hyperperfusion syndrome in elderly patients with chronic subdural hematoma. Surg Neurol. 2000; 54(2): 155-9.
- Morandi X, Haegelen C, Henaux PL, Riffaud L. Brain shift is central to the pathogenesis of intracerebral haemorrhage remote from the site of the initial neurosurgical procedure. Med Hypotheses. 2006; 67(4): 856-9.