Introduction
Mckittrick-Wheelock syndrome is a pathological entity that is
represented by the presence of a large rectal tumour with histopathological findings of tubular-villous adenoma that associates
important secretion of electrolyte-rich mucin. Thus, this syndrome
will inflect multiple diarrheic stools on the affected patients with
the secretion of electrolyte-rich mucin that will manifest as an
electrolyte imbalance with hypopotassaemia, hyponatremia, and
hypochloraemia, as well as with pre-renal chronic kidney injury
and severe dehydration syndrome. Initially described in 1954 by
Leland S. Mckittrick and Frank C. Wheelock, the medical literature
comprises only 257 such cases worldwide by the year 2018. We
can thus conclude that the debate regarding the diagnosis and
therapeutic management of Mckittrick-Wheelock syndrome is
still in its infancy. Usually, from a clinical standpoint, watery diarrheic stools with mucus discharge and subsequent metabolic issues, are the reason to blame for the generally altered state in
which the patients address the physician with nausea, vomiting,
fatigability, and even fainting.
The clinical finding characteristic of this disease is the prolonged time of symptomatology progress, usually about 24
months until the first presentation, patients having multiple admissions to the hospital or outpatient clinic in this timeframe with
diagnoses ranging from enterocolitis to ketoacidosis or infectious
colitis. This determined many authors to define Mckittrick-Wheelock syndrome as a rare cause of metabolic coma and to introduce
it in the differential diagnosis of prerenal chronic kidney injury. Nevertheless, this mandated the development of specific medical
conservative treatments to normalize altered kidney function and
to counteract sodium depletion, a fundamental element in the
preparation for surgical resection.
Thus, from a therapeutic standpoint, surgical success leans on
the efficacy of the preoperative medical treatment, which may be
the only line of treatment for patients that refuse surgical resection. In this case, treatment is going to be an association of indomethacin and octreotide that will reduce fluid loss. We further
state that surgical treatment remains the only option that can be
curative and radical for this affection and that literature studies
show the mortality from villous rectal adenomas specific to the
Mckittrick Wheelock syndrome to be 100%.
Material and method
We present the case of a patient diagnosed in 2019 with a rectal tumour, compatible from a clinical, paraclinical, and histopathological standpoint with Mckittrick Wheelock syndrome that was
operated minimally invasive, through laparoscopy, in the Surgery
Clinic of the Emergency County Hospital of Constanta.
Case report
A 65-year-old patient, with a rectal tumor discovered in 2019,
that was not diagnosed or followed up and was neglected therapeutically, with many admissions during the last couple of years
in the Nephrology department, where she was investigated and
treated for chronic kidney injury through a pre-renal mechanism. The patient was admitted in late 2020 through the Emergency
Care Unit of Constanta County Hospital, with a generally altered
state caused by multiple diarrheic stools at home. The lab workup revealed a severe dehydration syndrome with nitrous-oxide
retention and hyponatremia. After analysis of the biochemical results (creatinine = 3.26 mg/dl, urea = 176 mg/dl, K = 3.6 mmol/l,
Na=139 mmol/l, proteins = 6.2 g/dl) the patient was admitted to
the Nephrology department with the diagnosis of kidney injury
of pre-renal origin. The general state of the patient after starting
specific treatment got better, with partial normalization of biomarkers and partial symptom remission, which permitted further
investigations.
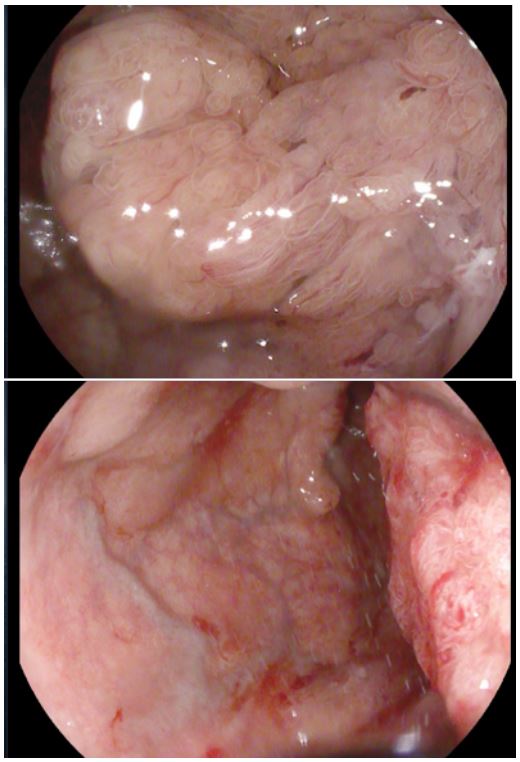
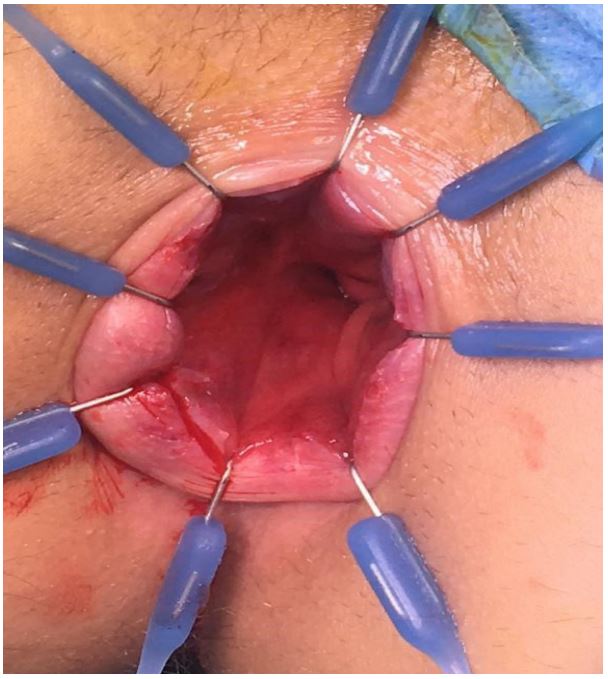
Considering the patient’s history, a rectoscopy is ordered that
shows internal hemorrhoids in the anal canal and a protrusive tumoral mass at 2 cm from the external anal edge, circumferential
but non-obstructive on a length of about 10 cm, covered by friable mucosa that is biopsied. The histopathological result shows
a tubule-villous adenoma with high-grade and low-grade intraepithelial dysplasia and metaplasia.
In this context, further investigations are considered, and a native CT scan of the abdomen and pelvis is performed that reveals
and confirms a protrusive, iodophilic, circumferential parietal
thickening, with imprecise edges, and irregular shape, of about
29 mm that associates the distension of the colon upstream; normal liver with homogenous structure, a suprarenal adenoma, and
a left cortical kidney cyst Bosniak, with no. other visible lesions.
The clinical data, biological and imagistic results, together with
the rectal biopsy, point to the diagnosis of Mckittrick-Wheelock
syndrome, mandating the patient’s transfer to the Surgery Department for specialized treatment. After a short preoperative
preparation with electrolyte rebalance and mechanical purging
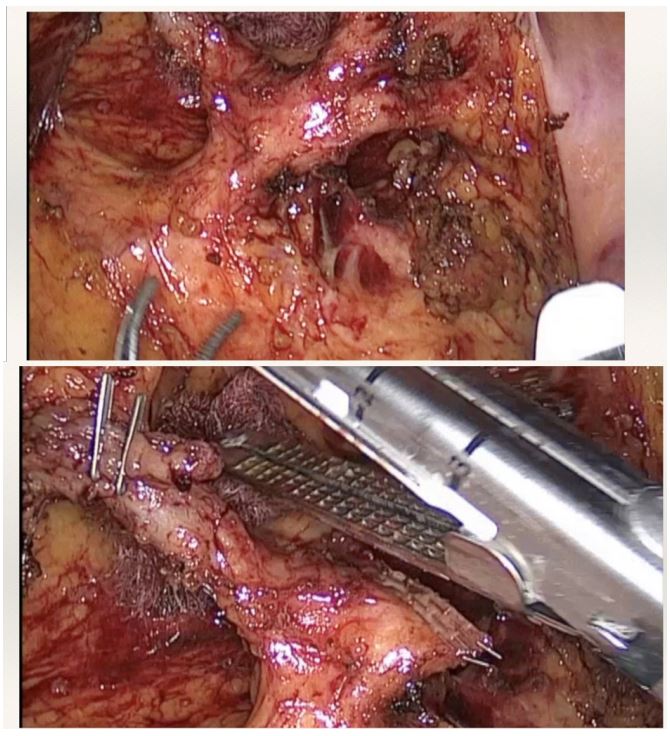
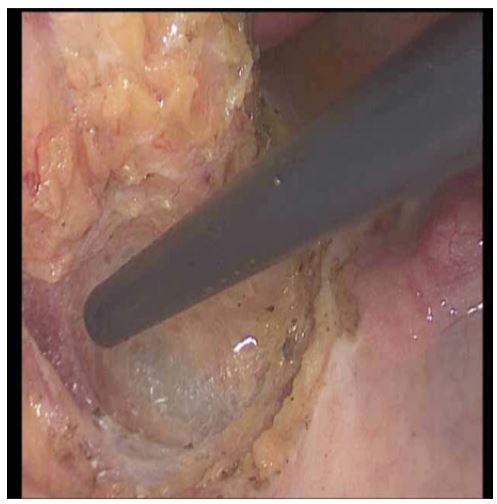
of the colon, the patient is scheduled for laparoscopic resection bearing in mind the advantages of this technique regarding postoperative evolution and the fact that this type of approach
is “sphincter-saving” Ultralow laparoscopic rectal resection with
complete mesorectal excision and mechanical terminal-terminal
colo-anal anastomosis is performed with a protective derivative
ileostomy is performed.
Results
From a surgical standpoint, the postoperative evolution of the
patient was favorable, having no abdominal pain, and minimal
peritoneal drainage that was subsequently removed one by one.
Intestinal transit restarted through the protective ileostomy that
had proper healing. Postoperative wound with good healing. No
signs of fever or other general imbalances with discharge on day
7 p.o. Ileostomy reversal was scheduled in 4 weeks’ time. Regardless of these favorable results from a pure surgical point of view,
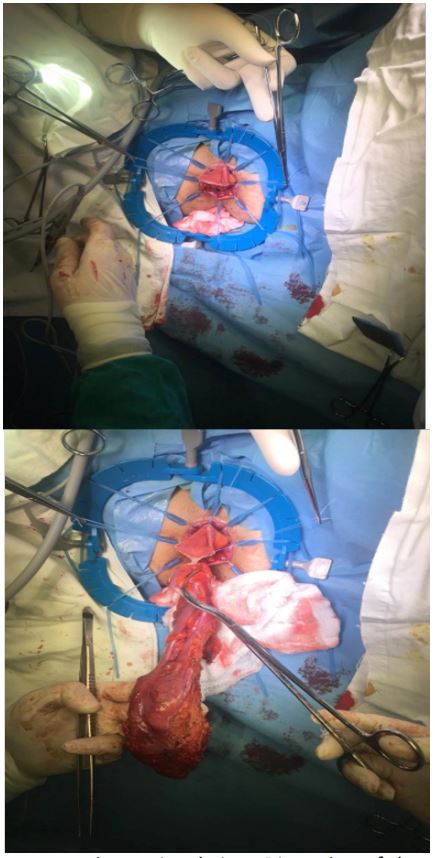
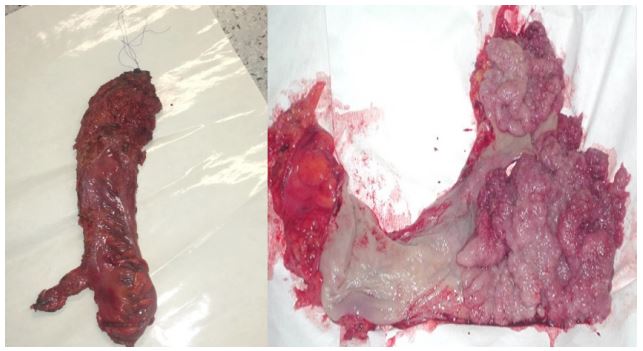
we consider the histopathological results on the final specimen to
be the definitive appreciation point. After a macroscopic examination of the specimen, it is noted to be 23 cm in length, circumferential, and with a protrusive vegetating tumor, 12/7/2 cm in size,
reddish color and friable mucosa.
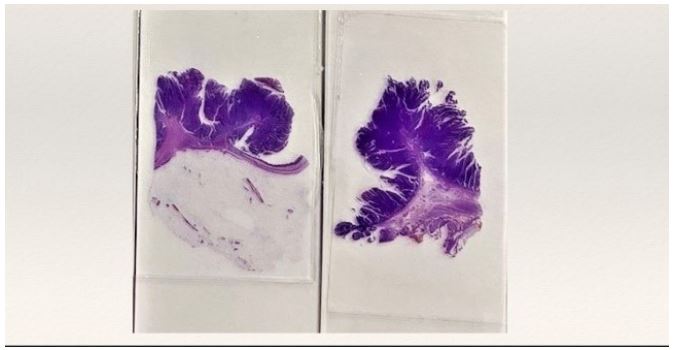
From a microscopic point of view, the rectal specimen had a
tumoral mass compatible with a tubulovillous adenoma with high
and low-grade intraepithelial dysplasia/neoplasia, laminae propria with chronic inflammation, and hyperemia. 4 regional lymph
nodes non-invaded and surgical margins as well, the closest being
the distal margin at about 1.5 mm.
Discussion
Mckittrick-Wheelock was first described by Mckittrick and
Wheelock in 1954. It is a rare disorder with fluid and electrolyte
depletion caused by a secretory colorectal tumor. In most cases,
a villous adenoma [3]. Most of the patients with this disorder can
present with chronic diarrhea and symptoms due to electrolyte
imbalances, such as lethargy, muscle cramps, ileus, and vomiting.
The incidence and prevalence of MWS are difficult to estimate as
some of the cases have also been reported as electrolyte depletion syndromes [4,8,9].
Recent studies have shown that in patients with this condition,
rectal secretions have higher concentrations of prostaglandin E2
(PGE2) and intracellular cyclic adenosine monophosphate (cAMP).
Additionally, a large surface area of the villous adenomas further
causes increased fluid secretion, which exceeds the reabsorption
ability of the remaining normal rectal mucosa [8,10,11]. As treatment methods, the surgical intervention aims to remove villous
adenoma after correcting fluid and electrolyte imbalances. Also,
brachytherapy and endoscopic tumor resection are feasible alternatives [8,11]. Most colon cancers develop from benign adenomas, but the risk is higher when adenomas are villous and large.
Secretory villous adenomas have 100% mortality if left without
any treatment [12].
Conclusions
McKittrick-Wheelock syndrome is a rare and life-threatening
disease due to the risk of severe complications caused by renal
function impairment and hydro electrolyte imbalance. The presence of the clinical triad of renal function impairment with hydro
electrolyte imbalance, giant recto-sigmoidal tumor, and chronic
mucous diarrhea should raise the suspicion of McKittrick-Wheelock syndrome. The large surface area of the villous adenoma and
increased levels of PGE2, which serve as a secretagogue, is responsible for secretory diarrhea and electrolyte disturbances in
MWS. The trial of PGE2 synthase inhibitors, such as indomethacin,
can be given to the patient while waiting for surgery to improve
the symptoms. The treatment of this disease is the removal of the
tumor, preferably by minimally invasive surgery by laparoscopic
approach, due to the multiple advantages of this technique which
will benefit the patient, after the correction of kidney function
and hydro electrolyte imbalance.
Acknowledgements: None to declare.
References
- Arasaradnam RP, Brown S, Forbes A, et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology. Gut. 2018; 67: 1380-1399. 10.1136/gutjnl-2017-315909.
- Schiller LR, Pardi DS, Spiller R. Gastro 2013 APDW/WCOG Shanghai working party report: chronic diarrhea: definition, classification, diagnosis. J Gastroenterol Hepatol. 2014; 29: 6-25.
- McKittrick LS, Wheelock FC. Carcinoma of the colon. Dis Colon Rectum. 1997; 40: 1494-1496. 10.1007/BF02070718.
- Choi WH, Ryuk J, Kim HJ, et al. A case of giant rectal villous tumor with severe fluid-electrolyte imbalance treated by laparoscopic low anterior resection. J Korean Surg Soc. 2012; 82: 325-329. 10.4174/jkss.2012.82.5.325.
- McCabe RE, Kane KK, Zintel HA, Pierson RN. Adenocarcinoma of the colon associated with severe hypoka-lemia: report of a case. Ann Surg. 1970; 172: 970-974. 10.1097/00000658-197012000-00007.
- Older J, Older P, Colker J, Brown R. Secretory villous adenomas that cause depletion syndrome. Arch Intern Med. 1999; 159: 879-880. 10.1001/archinte.159.8.879.
- Targarona E, Hernandez PM, Balague C, et al. McKittrick-Wheelock syndrome treated by laparoscopy: re-port of 3 cases. Surg Laparosc Endosc Percutan Tech. 2008; 18: 536-538. 10.1097/SLE.0b013e31818135ad.
- Mois EI, Graur F, Sechel R, Al-Hajjar N. McKittrick-Wheelock syndrome: a rare case report of acute renal failure. Clujul Med. 2016; 89: 301-303. 10.15386/cjmed-536.
- Orchard MR, Hooper J, Wright JA, McCarthy K. A systematic review of McKittrick-Wheelock syndrome. Ann R Coll Surg Engl. 2018; 100: 591-597. 10.1308/rcsann.2018.0184.
- Jacob H, Schlondorff D, St Onge G, Bernstein LH. Villous adenoma depletion syndrome. Evidence for a cyclic nucleotide-mediated diarrhea. Dig Dis Sci. 1985; 30: 637-641. 10.1007/BF01308412.
- Popescu A, Orban-Schiopu AM, Becheanu G, Diculescu M. McKittrick-Wheelock syndrome - a rare cause of acute renal failure. Rom J Gastroenterol. 2005; 14: 63-66.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 1000097.
- Langeron P, Prévost AG, Boudailliez C. Rectosigmoid villous tumors with hydroelectrolytic disorders. J Sci Med Lille.1969; 5-23.
- Emrich J, Niemeyer C. The secreting villous adenoma as a rare cause of acute renal failure. Med Klin. 2002; 619-623.
- Ashour N, Qassem JA, Al-Tourah W. Villous adenoma depletion syndrome: case report. Kuwait Med J. 2007; 358-360.
- Tuţă LA, Boşoteanu M, Deacu M, Dumitru E. McKittrick–Wheelock syndrome: a rare etiology of acute re-nal failure associated to well-differentiated adenocarcinoma (G1) arising within a villous adenoma. Rom J Mor-phol Embryol. 2011; 1: 1153-1,156.
- Rutter MD, Chattree A, Barbour JA et al. British Society of Gastroenterology/Association of Coloproctolo-gists of Great Britain and Ireland guidelines for the management of large non-pedunculated colorectal polyps. Gut 2015; 1,847–1,873.
- Fernández-López F, Paredes-Cotore JP. McKittrick–Wheelock syndrome – prolapsed giant villous adenoma of the rectum. Rev Esp Enferm Dig. 2013; 309-310.
- Nakhla SG, Murakami TT, Sundararajan S. Poorly differentiated neuroendocrine tumor of the rectum coex-istent with giant rectal villous adenoma presenting as McKittrick–Wheelock syndrome. Case Rep Oncol Med. 2015; 242760.
- Chen YH, Kang JC, Lai HJ. Rectal villous adenoma with McKittrick–Wheelock syndrome: report of a rare case. Visc Med. 2013; 55-58.
- Targarona EM, Hernandez PM, Balague C et al. McKittrick–Wheelock syndrome treated by laparoscopy: report of 3 cases. Surg Laparosc Endosc Percutan Tech. 2008; 536-538.