Introduction
Total thoracoscopy (TTS) for cardiac surgery has recently been
of great interest in contrast to the traditional median sternotomy
on account of advantageous minimal invasiveness, shorter period
of hospital stay as well as comparable long-term outcomes [1,2].
However, the limited surgical exposure and surgeons’ movement
resulting from the small incision raise concerns that augmented
aortic cross-clamp (ACC) time probably aggravates the cardiac
ischemic injury and therefore compromise the postoperative outcomes. To address these, tremendous efforts have been made
such as the minimization of crowded surgical fields and simplification of surgical procedures [3]. Additionally, the myocardial protection is particularly imperative in this setting. The frequently adopted cardioplegia solutions that enable a pharmacological myocardial arrest in diastole would reduce energy use and thereby
minimize the myocardial ischemic injury [4]. Buckberg Blood cardioplegic [BCP] solution in a (1:4) dilution with whole blood has
been the standard solution extensively applied in adult cardiac
surgery for decades because of its more oxygen-carrying capacity
and physiological properties [5,7]. But the multiple-dose administration may interrupt the operation flow. In contrast, Custodial
histidine-tryptophan-ketoglutarate (HTK) which is an intracellular
crystalloid cardioplegic solution, allows a single-dose administration. It also emerged as a promising cardioplegic agent in children
and adults since first fabricated by Bretschneider in the (1970)
s [8,9]. Both have been demonstrated with comparable safety
and effectiveness in isolated aortic valve replacement and elective mitral valve surgery [10,11]. However, the direct comparison
between these two cardioplegic solutions in a spectrum of TTS for
cardiac surgery is scanty. Therefore, this study was undertaken to
compare the myocardial protection performance in the context of
totally thoracoscopic cardiac surgery between BCP and HTK solutions.
Methods
Study design: A total of 101 patients undergoing thoracoscopic
cardiac surgery using either BCP or HTK solution between January
2021 to December 2021 at Guangdong Provincial People’s Hospital
were retrospectively enrolled. The demographic data, medical history, surgery information, anesthesia record, and perfusion record
were all reviewed and collected. The present study was approved
by the Guangdong Provincial People’s Hospital ethics committee.
Surgical technique: Conventional general anesthesia was applied to all patients. The route for TTS was established by the right
lateral 3rd to 4th intercostal space or right anterior 2nd to 3rd intercostal space. To achieve cardiopulmonary bypass (CPB), cannulation of the femoral artery and vein was first performed. The right internal jugular vein was directly cannulated for drainage of the
superior vena cava. All cardiac procedures were performed under mild hypothermia or normothermia. After CPB establishment
and ACC, cardioplegic solutions were infused in antegrade, retrograde, or both fashions. The details of cardioplegic solution administration varied individually. In general, the BCP in a 4:1 blood
dilution was administrated with an initial dose of 1200-1500 ml
and a maintained dose of approximately 500 ml given every 15-20
minutes thereafter. In contrast, HTK was administrated in a singledose manner with 2000 ml and most commonly in an antegrade
direction. If the ACC time is over 2 hours, an additional dose of
500-1000 ml would be used. The use of inotropes, insulin requirement, fluid administration, and intraoperative transfusion would
be carried out and decided by the whole surgical team following
the institutional protocols.
Study endpoints: The primary outcome reflecting postoperative myocardial injuries included postoperative levels of cardiac
Troponin T (cTnT) and creatine kinase-MB [CKMB] at different
periods, the capacity of return to spontaneous rhythm, postoperative left ventricle ejection fraction (LVEF) as well as vasoactiveinotropic score (VIS). Myocardial infarction (MI) was defined as
the postoperative CKMB of more than 100 ug/L as previously described [12]. The VIS was calculated according to the following
formula: VIS = 10,000 × vasopressin (mU/kg/min) + 10 × milrinone
(mg/kg/min) + 100 × norepinephrine (mg/kg/min) + 100 × epinephrine (mg/kg/min) + dobutamine (mg/kg/min) + dopamine
(mg/kg/min) [13]. The secondary endpoints included mechanical
ventilation time, intensive care unit (ICU) stay, hospital stay, mechanical circulatory support [MCS], and in-hospital mortality.
Statistical analyses: Continuous data were presented as mean
± standard deviation if normally distributed or median with interquartile range if non-normally distributed. Categorical data were
presented as the frequency with percentage. The results between
the two groups were compared using the Student t-test, MannWhitney U test, chi-square test, and Fisher exact test as appropriate. Multivariate logistic regression for postoperative outcomes
including MI and return to spontaneous rhythm was performed
with the following independent variables: age, female gender,
body mass index (BMI), atrial fibrillation, LVEF, HTK, ACC time,
and total volume. All statistical analysis were performed using the
IBM SPSS Statistics version 26.0 and R statistical software version
4.1.3. A p-value less than 0.05 were considered to be significant.
Results
Baseline characteristics: In the present study, 69 patients underwent totally thoracoscopic cardiac surgery with BCP perfusion
while 32 patients with HTK perfusion. The baseline characteristics were summarized in Table 1. The two groups were comparable as
a consequence of no significant difference in age, female gender,
BMI, atrial fibrillation, hypertension, diabetes, dyslipidemia, cerebrovascular event, creatine (Cr), cTnT, CKMB, LVEF, European System for Cardiac Operative Risk Evaluation (euroSCORE) (p>0.05).
Perioperative data: As shown in Table 2, the pre-perfusion
blood gas analysis (BGA) including the K+
, Hematocrit (Hct), and
Lactate were similar between the two groups. However, 98.55%
were delivered in an antegrade fashion in the BCP group, significantly higher than 84.38% in the HTK group (p<0.05). There were
significantly higher total doses but lower total volume in the BCP
group in contrast to the HTK group (p<0.05). No significant differences regarding the surgical procedures, CPB time, and ACC time
was observed between the two groups (p>0.05).
Outcomes: In Table 3, a significantly more proportion of patients perfused by BCP could return to spontaneous rhythm than
by HTK (84.58% for the BCP group vs 62.50% for the HTK group)
(p=0.025). The median level of both Hct and lactate was significantly lower in the BCP group than that in the HTK group (p<0.05).
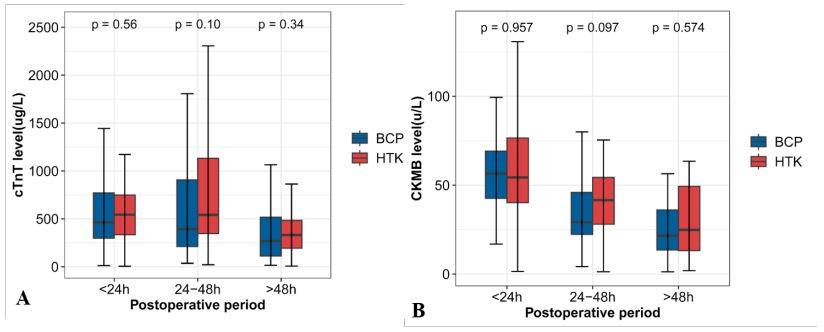
However, both the postoperative peak cTnT/CKMB (Table 3) and
the postoperative cTnT/CKMB levels at the period of <24h, 24-
48h, and >48h (Figure 1) were similar between the two groups.
There was no significant difference in the postoperative LVEF, VIS,
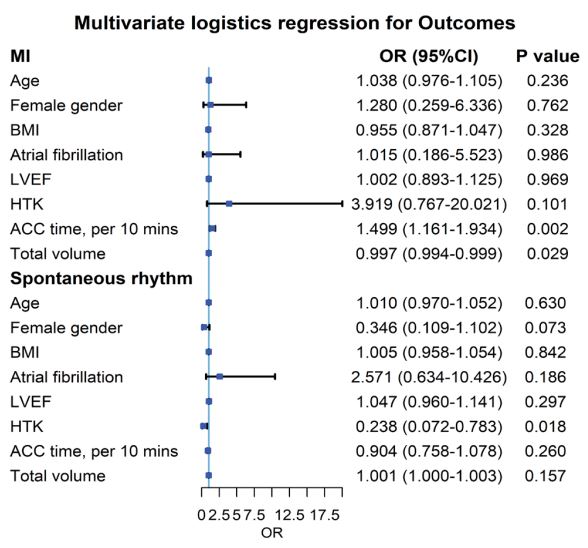
mechanical ventilation time, ICU stay, MI, need for MCS, and inhospital mortality (p>0.05). In (Figure 2), multivariate logistics
regression revealed that the type of cardioplegic solutions was
not associated with MI but associated with a return to spontaneous rhythm. Specifically, HTK perfusion was associated with
a lower possibility to return to spontaneous rhythm (odds ratio
(OR)=0.238; confidence interval (CI)=0.072-0.783; p=0.018). Additionally, increased ACC time (per 10 mins) was associated with
a higher risk of MI (OR=1.499; CI=1.161-1.934; p=0.002) while
increased total volume was associated with a lower risk of MI
(OR=0.997; CI=0.994-0.999; p=0.029).
Table 1: Baseline characteristics.
|
BCP (n=69) |
HTK (n=32) |
p |
| Age (y) |
50.44±14.52 |
51.63±12.79 |
0.693 |
| Female gender |
39 (56.52%) |
16 (50.00%) |
0.540 |
| BMI (kg/m2) |
22.77 (20.80-27.06) |
23.64 (20.05-25.29) |
0.737 |
| Atrial fibrillation |
21 (30.43%) |
9 (28.13%) |
0.813 |
| Hypertension |
8 (11.59%) |
4 (12.50%) |
>0.999 |
| Diabetes |
1 (1.45%) |
2 (6.25%) |
0.489 |
| Dyslipidemia |
3 (4.35%) |
2 (6.25%) |
1.000 |
| Cerebrovascular event |
5 (7.25%) |
0 (0) |
0.285 |
| Cr (mmol/L) |
70.80 (59.38-84.38) |
76.75 (61.04-81.22) |
0.867 |
| cTnT (ug/L) |
7.50 (2.50-11.75) |
8.60 (6.18-11.80) |
0.358 |
| CKMB (u/L) |
5.00 (5.00-11.07) |
5.44 (5.00-11.23) |
0.627 |
| LVEF (%) |
65.43±6.20 |
64.27±6.55 |
0.390 |
| euroSCORE |
4.00 (3.00-6.00) |
4.00 (3.00-6.15) |
|
BCP: Blood Cardioplegia; HTK: Histidine-Tryptophan-Ketoglutarate; BMI:
Body Mass Index; Cr: Creatine; cTnT: Cardiac Troponin T; CKMB: Creatine
Kinase-MB; LVEF: Left Ventricle Ejection Fraction; euroSCORE: European
System for Cardiac Operative Risk Evaluation.
Table 2: Operative profile.
|
BCP (n=69) |
HTK (n=32) |
p |
| Pre-BGA |
|
|
|
| K+ (mmol/L) |
3.60 (3.30-3.90) |
3.50 (3.33-3.98) |
0.798 |
| Hct (%) |
35.00 (29.00-37.50) |
36.50 (30.25-41.00) |
0.213 |
| Lactate (mmol/L) |
0.80 (0.70-1.10) |
0.80 (0.70-1.18) |
0.789 |
| Delivery |
|
|
0.016 |
| Antegrade |
68 (98.55%) |
27 (84.38%) |
|
| Retrograde |
1 (1.45%) |
3 (9.38%) |
|
|
Antegrade and retrograde
|
0 (0) |
2 (6.25%) |
|
| Cardioplegia |
|
|
|
| Total doses |
2 (1-2) |
1 (1-1) |
0.000 |
| Total volume (ml) |
1900 (1500-2100) |
2000 (2000-2000) |
0.004 |
| Surgical procedures |
|
|
0.262 |
| AV |
4 (5.80%) |
3 (9.37%) |
|
| MV |
35 (50.72%) |
17 (53.13%) |
|
| TV |
2 (2.90%) |
0 (0) |
|
| ASD |
1 (1.45%) |
0 (0) |
|
| AV+MV |
1 (1.45%) |
3 (9.37%) |
|
| MV+TV |
23 (33.33%) |
7 (21.88%) |
|
| AV+MV+TV |
1 (1.45%) |
2 (6.25%) |
|
| ASD+TV |
2 (2.90%) |
0 (0) |
|
| CPB time (min) |
150.79±44.18 |
154.00±50.44 |
0.746 |
| ACC time (min) |
88.57±34.19 |
95.84±33.73 |
0.320 |
BCP: Blood Cardioplegia; HTK: Histidine-Tryptophan-Ketoglutarate; BGA:
Blood Gas Analysis; Hct: Hematocrit; AV: Aortic Valve; MV: Mitral Valve;
TV: Tricuspid Valve; ASD: Atrial Septal Defect; CPB: Cardiopulmonary
Bypass; ACC: Aortic Cross-Clamp.
Table 3: Early postoperative outcomes.
|
BCP (n=69) |
HTK (n=32) |
p |
|
Return to spontaneous rhythm
|
58 (84.58%) |
20 (62.50%) |
0.025 |
| Post-BGA |
|
|
|
| K+ (mmol/L) |
5.10 (4.50-5.76) |
5.40 (4.90-5.85) |
0.155 |
| Hct (%) |
25.00 (24.00-28.50) |
28.00 (24.25-31.50) |
0.045 |
| Lactate (mmol/L) |
1.10 (1.00-1.50) |
1.40 (1.20-2.30) |
0.005 |
| LVEF (%) |
62.00 (56.29-65.00) |
60.00 (53.43-63.88) |
0.462 |
| Peak cTnT (ug/L) |
479.20 (315.10-1004.10) |
609.10 (323.25-1106.10) |
0.919 |
| Peak CKMB (u/L) |
56.00 (41.40-71.10) |
51.25 (32.17-76.50) |
0.414 |
| VIS |
5.00 (3.00-6.75) |
5.00 (2.00-8.75) |
0.878 |
|
Mechanical ventilation time
(h)
|
9.92 (4.17-18.75) |
7.50 (4.17-17.71) |
0.677 |
| ICU stay (h) |
44.58 (22.75-69.50) |
39.85 (21.10-67.98) |
0.348 |
| Hospital stay (d) |
6.00 (5.00-8.00) |
7.00 (5.00-8.00) |
0.415 |
| MI |
6 (8.70%) |
6 (18.75) |
0.262 |
| MCS |
2 (2.90%) |
0 (0) |
0.837 |
| In-hospital mortality |
2 (2.90%) |
0 (0) |
0.837 |
Discussion
The present study found that the myocardial protection performance was equivalent between HTK and BCP groups in the
context of cardiac surgery by TTS, as a consequence of the similar
level of myocardial enzymes at any postoperative time point, LVEF,
VIS, and incidence of MI. Additionally, the administration of HTK
resulted in comparable short-term clinical outcomes in terms of mechanical ventilation time, ICU stay, hospital stay, MCS, and inhospital mortality versus BCP. However, the HTK solution seems to compromise the capacity of postoperative return to spontaneous
rhythm. HTK is an intracellular crystalloid cardioplegic solution
with tryptophan to stabilize the cell membrane, ketoglutarate to
promote ATP energy generation during reperfusion, histidine as a
buffer, and mannitol to ameliorate the cellular edema [14,16]. It
can cause heart arrest by inhibiting the rapid phase of the action
potential, theoretically protecting the myocardial ischemia for
up to 120 minutes. Indeed, our study demonstrated comparable
myocardial protection as well as short-term outcomes on HTK administration in contrast to the standard BCP administration in a
spectrum of totally thoracoscopic cardiac surgery, which is consistent with the previous studies in other situations. Viana et al.
compared the use of HTK versus standard tepid blood cardioplegia in complex cardiac procedures, suggesting that the myocardial
protection was comparable between the two groups in this setting [9]. Hoyer et al. assessed the impact of BCP and HTK administration on short- and long-term outcomes in isolated aortic valve
replacement, also showing equivalent outcomes [10]. Therefore,
our findings verified the safety and efficacy of HTK as an alternative cardioplegic agent to BCP in cardiac procedures by TTS. Of
note, patients receiving HTK solutions were not prone to return
to spontaneous rhythm after cross-clamp removal in our study. In
other words, more proportional spontaneous ventricular fibrillation occurred in the HTK group, which was lined with the previous
study [11]. This may at least in part be attributed to the conduction disturbances of low adenosine triphosphate levels, electrolyte concentration alteration across the cell membranes, oxidative stress, and insufficient myocardial protection resulting from
heterogeneous reperfusion. Regardless, the increased spontaneous ventricular fibrillation in the HTK group seems not adversely
impact the myocardial enzyme release and short-term outcomes.
The total volume of cardioplegic solution was significantly higher
in the HTK group than that in the BCP group. HTK acting as singledose formula requires more volume to ensure relatively myocardial homogenous distribution of cardioplegia as well as complete
cooling. In this study, the volumes were applied following the
recommendations from HTK manufactured company determined
by the experienced perfusionist. There were several inherent
limitations in this study. The retrospective and single institution
in nature limits its generalizability. A prospective multi-center investigation comparing HTK and BCP is warranted. Additionally, the
number of enrolled patients was not sufficient to verify any small
but significant difference in our primary endpoints such as LVEF
and VIS. What’s more, we did not capture perioperative serum
sodium levels since the administration of HTK was demonstrated
to be associated with an increased risk of hyponatremia and postoperative seizure [4]. Finally, continuous follow-up is required to
assess the long-term impact of the cardioplegic solution type.
Conclusion
HTK administration during the totally thoracoscopic cardiac
surgery provides comparable myocardial protection and shortterm outcomes to the BCP administration. But HTK seems to
compromise the capacity of postoperative return to spontaneous
rhythm. A randomized prospective study comparing safety and efficacy between these two groups is warranted.
Declarations
Funding: This study was supported by National Key Research
and Development Program of China (No. 2020YFC1107904, No.
2022YFC2407406), Science and Technology Planning Project
of Guangdong Province (2019B020230003; 2018B090944002;
2020B1111170011), Science and Technology Fundation for
Guangzhou Health (2023A031004), Science and Technology Program of Guangzhou (202206010049), Guangzhou Science and
Technology Planning Project (2023B03J0596), and Guangdong
peak project (DFJH201802; DFJH2020029).
Acknowledgments: We are thankful for the help and support
from each member of Zhuang’s Group and Chen’s Group.
Conflicts of interest: The authors declared no conflicts of interest.
References
- McClure RS, Athanasopoulos LV, McGurk S, Davidson MJ, Couper GS, Cohn LH. One thousand minimally invasive mitral valve operations: early outcomes, late outcomes, and echocardiographic follow-up. J Thorac Cardiovasc Surg. 2013; 5: 1199-206. doi:10.1016/j.jtcvs.2012.12.070.
- Dieberg G, Smart NA, King N. Minimally invasive cardiac surgery: A systematic review and meta-analysis. Int J Cardiol. 2016; 554-60. doi:10.1016/j.ijcard.2016.08.227.
- Lu S, Song K, Yao W, Xia L, Dong L, Sun Y, et al. Simplified, minimally invasive, beating-heart technique for redo isolated tricuspid valve surgery. J Cardiothorac Surg. 2020; 1: 146. doi:10.1186/s13019-020-01192-1.
- Turner, II, Ruzmetov M, Niu J, Bibevski S, Scholl FG. Scavenging right atrial Bretschneider histidine-tryptophan-ketoglutarate cardioplegia: Impact on hyponatremia and seizures in pediatric cardiac surgery patients. J Thorac Cardiovasc Surg. 2021; 1: 228-37. doi:10.1016/j.jtcvs.2020.08.098.
- Follette DM, Mulder DG, Maloney JV, Buckberg GD. Advantages of blood cardioplegia over continuous coronary perfusion or intermittent ischemia. Experimental and clinical study. J Thorac Cardiovasc Surg. 1978; 5: 604-19.
- Follette DM, Fey K, Buckberg GD, Helly JJ, Jr., Steed DL, Foglia RP, et al. Reducing postischemic damage by temporary modification of reperfusate calcium, potassium, pH, and osmolarity. J Thorac Cardiovasc Surg. 1981; 2: 221-38.
- Follette DM, Steed DL, Foglia R, Fey K, Buckberg GD. Advantages of intermittent blood cardioplegia over intermittent ischemia during prolonged hypothermic aortic clamping. Circulation. 1978; 3(2): 200-9.
- Schaper J, Scheld HH, Schmidt U, Hehrlein F. Ultrastructural study comparing the efficacy of five different methods of intraoperative myocardial protection in the human heart. J Thorac Cardiovasc Surg. 1986; 1: 47-55.
- Viana FF, Shi WY, Hayward PA, Larobina ME, Liskaser F, Matalanis G. Custodiol versus blood cardioplegia in complex cardiac operations: an Australian experience. Eur J Cardiothorac Surg. 2013; 3: 526-31. doi:10.1093/ejcts/ezs319.
- Hoyer A, Lehmann S, Mende M, Noack T, Kiefer P, Misfeld M, et al. Custodiol versus cold Calafiore for elective cardiac arrest in isolated aortic valve replacement: a propensity-matched analysis of 7263 patients. Eur J Cardiothorac Surg. 2017; 2: 303-9. doi:10.1093/ejcts/ezx052.
- Braathen B, Jeppsson A, Schersten H, Hagen OM, Vengen O, Rexius H, et al. One single dose of histidine-tryptophan-ketoglutarate solution gives equally good myocardial protection in elective mitral valve surgery as repetitive cold blood cardioplegia: a prospective randomized study. J Thorac Cardiovasc Surg. 2011; 4: 995-1001. doi:10.1016/j.jtcvs.2010.07.011.
- Lenoir M, Bouhout I, Jelassi A, Cartier R, Poirier N, El-Hamamsy I, et al. Del Nido cardioplegia versus blood cardioplegia in adult aortic root surgery. J Thorac Cardiovasc Surg. 2021; 2: 514-22 e2. doi:10.1016/j.jtcvs.2020.01.022.
- Gaies MG, Gurney JG, Yen AH, Napoli ML, Gajarski RJ, Ohye RG, et al. Vasoactive-inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr Crit Care Med. 2010; 2:234-8. doi:10.1097/PCC.0b013e3181b806fc.
- Aarsaether E, Stenberg TA, Jakobsen O, Busund R. Mechanoenergetic function and troponin T release following cardioplegic arrest induced by St Thomas’ and histidine-tryptophan-ketoglutarate cardioplegia--an experimental comparative study in pigs. Interact Cardiovasc Thorac Surg. 2009; 4: 635-9. doi:10.1510/icvts.2009.208231.
- Preusse CJ, Gebhard MM, Bretschneider HJ. Myocardial “equilibration processes” and myocardial energy turnover during initiation of artificial cardiac arrest with cardioplegic solution - reasons for a sufficiently long cardioplegic perfusion. Thorac Cardiovasc Surg. 1981; 2: 71-6. doi:10.1055/s-2007-1023446.
- Preusse CJ, Winter J, Schulte HD, Bircks W. Energy demand of cardioplegically perfused human hearts. J Cardiovasc Surg (Torino). 1985; 6: 558-63.