Introduction
The most widely used anesthesia technique for cesarean delivery is the spinal anesthesia (SA). In Bnai-Zion Medical Center over
than 90% of the elective cesarean sections performed under SA.
However, this type of anesthesia frequently associated with side
effects that primarily affect the parturient and the fetal health [1].
Nearly, 70-80% of obstetric patients experience spinal anesthesiainduced hypotension (SAIH) without pharmacological prophylaxis
[2]. This hypotension is commonly accompanied with reflex tachycardia, nausea and vomiting, and in rare occasions bradycardia
can be observed. Most authors agree that hypotension presents
when systolic blood pressure (SBP) reduced from baseline of more
than 20% [3]. The main mechanism of SAIH is decreased systemic
vascular resistance resulting from arterial vasodilation [4].
In addition, sympathetic nervous system blockade can decrease venous return to the right heart and can reduce the preload. In response, stimulation of cardiac sensory receptors in the
left ventricle leads to vasodilation, bradycardia and hypotension,
and this is the Bezold Jarish Reflex (BJR) [5]. Augmentation of the
intravascular volume with crystalloids and vasopressors is the
cornerstone of the treatment of SAIH [2]. Among vasopressors,
the pure α-adrenergic receptor agonist phenylephrine has become the first-line treatment in the last years because of its efficacy to maintain the umbilical cord blood PH and the Apgar score
in the neonates [6]. Ondansetron, a 5-HT3 receptor antagonist
that used generally for prophylaxis and treatment of nausea and
vomiting may attenuate the SAIH [7,8]. Numerous studies were
performed to investigate the effect of ondansetron on SAIH, but
given the relatively large heterogeneity and small sample sizes in
the involved studies, further large and strict randomized clinical
trials are still needed, especially among obstetric patients [9]. We
hypothesized that prophylactic use of intravenous ondansetron
before SA in elective cesarean section can reduce SAIH and can
reduce the amount of vasopressor phenylephrine needed to control blood pressure. The primary outcome was to compare the
changes in maternal blood pressure and phenylephrine consumption between two groups of mothers undergoing cesarean section
under SA, the first received ondansetron and the second received
placebo. The secondary outcomes were to compare adverse effects such as bradycardia, nausea & vomiting and dizziness between the two groups, as well as the difference in umbilical cord
blood pH and the Apgar score between the two groups at the first
minute after delivery.
Materials and methods
This prospective double-blind study, conducted following institutional ethical committee approval (0053-19-BNZ).
Exclusion criteria: Mothers who has presented with hypertensive disorders of pregnancy or unstable hemodynamics and
coagulation abnormality before surgery, mothers presented with
cardiovascular disease or hypersensitivity to ondansetron, mothers on drugs that may cause hypotension, were excluded also
mothers who converted SA to GA were also excluded.
Group O: The Ondansetron group, fifty parturient who received 4 mg of Ondansetron intravenously diluted in 10 ml of
0.9% sodium chloride over one minute, five minutes before performing the SA.
Group P: The Placebo group, fifty parturient who received 10
ml of pure 0.9% sodium chloride.
All the mothers were in fasting for 8 hours at least before surgery. Intravenous (IV) access was established in all patients with
an 18-20-gauge peripheral intravenous catheter. Premedication
with IV ranitidine 50 mg and IV metoclopramide 10 mg were
given one hour before surgery. Upon patient arrival to the operating room, standard ASA monitoring was connected, baseline
values of pulse oximetry (SpO2
), non-invasive Blood Pressure (BP)
and electrocardiogram (ECG) were recorded. Pre-hydration with
Ringer’s lactate infusion 1000 ml started 30 min before surgery.
IV cephamycin 2 grams for antimicrobial prophylaxis was given 20
min before surgery.
SA was performed according to the institute protocol in the
sitting position, after sterile preparation and skin infiltration with
local anesthetic, Lumbar puncture was performed at L3-L4, L4-
L5 intervertebral space, using Whitacre pencil point 25, 27-gauge
needle. After identification of the subarachnoid space by cerebral
fluid outflow, 10 mg of hyperbaric Marcaine 0.5% and Fentanyl
0.02 mg were administered in the subarachnoid space. Following the subarachnoid injection patient positioned in a 15°-20°
left side position. The extent of the sensory block was evaluated
by pinprick test, surgery allowed to start after obtaining sensory
block higher than T6 dermatomes.
Vital signs (Systolic Blood Pressure-SBP, Diastolic Blood Pressure-DBP, Mean Blood Pressure-MBP, Heart Rate-HR) were recorded at the baseline, every 1 min for the first 5 minute after SA
induction and then every 5 minutes until the end of the operation
(to 35 min after SA for this study). Hypotension, defined as reduction in BP from baseline of more than 20%, which treated with
repeated doses of (50 mcg) intravenous phenylephrine and the
total requirements of phenylephrine consumption after SA were
recorded. Bradycardia, defined as heart rate drop less than 50
beats per minute which treated with single doses of IV Atropine
sulfate 0.5 mg was recorded.
Episodes of nausea, vomiting and dizziness were recorded.
Umbilical venous blood gas PH and Apgar score assessed by
pediatrician at the first minute after delivery for all the neonates
were also recorded.
Power analysis: For this study with a primary outcome defined
as changes in maternal blood pressure. The power analysis was
performed using the G*Power version 3.0.10 freeware (Franz
Faul, University of Kiel, Germany) http://www.gpower.hhu.de/.
To calculate sample size with a power of 0.8 that demonstrate
a difference of 20% or more in blood pressure as statistically significant (β=0.2, α=0.05), we took a sample size of 45 women per
group. Considering 10% unexpected exclusion we recruited 50
women in each group.
Statistical analysis: Statistical analysis was performed using
the STATA 12.0 software, (Stata Corp. 2011. Stata Statistical Software: Release 12. College Station, TX: Stata Corp LP.USA)
Vital signs variables (SPB, DBP, MBP, and HR) repeated measurements in eight time periods every 5 minutes (baseline, 5, 10,
15, 20, 25, 30, 35 minutes post SA), means, standard deviations
and 95% of C.I. (Confidence Interval) were calculated. The results
at each period of time between the two study groups were analyzed by the 2 sample T-test for differences of mean. The comparisons of results in each of the two study groups between the
eight time periods were analyzed by the repeated measurements
anova model with the Greenhouse-Geisser correction factor.
The results of the frequencies of women who received at least
one dose of phenylephrine post SA between the two study groups
were analyzed by chi square test. The results of total amount of
phenylephrine received by patients post SA, between the two
study groups were analyzed by the rank sum test (a non-parametric test).
For the results of intraoperative complications of bradycardia,
nausea & vomiting and dizziness, numbers and percentages were
calculated. The distributions for the categorical variables between
the two study groups were compared and analyzed by the Chi
square test or by Fisher-Irwin exact test (a non-parametric test for
small numbers).
For demographic and clinical data of age and fetal pH, means
and standard deviations were calculated. The results between the
two study groups were analyzed by the 2 sample T-test for differences of mean.
For the results of ASA and Apgar levels, numbers and percentages were calculated. The distributions for the categorical variables between the two study groups were compared and analyzed by Fisher-Irwin exact test.
All statistical tests were analyzed to a significance level of 0.05.
Table 1: Demographic data.
|
Group O (n=50) |
Group P (n=50) |
P value |
| Age (years) |
31.6±6.0 [17-55] |
31.7±4.5 [24-44] |
†0.9253 |
| ASA |
|
|
|
| 1 |
32 (64.0) |
33 (66.0) |
┴0.8330 |
| 2 |
18 (36.0) |
16 (32.0) |
| Not Determined |
|
1 (2.0) |
Data are mean SD and [range] or numbers (%). †2- sample T-test.
┴ Fisher- exact test
Results
The demographic data (Age, ASA) are presented in Table 1.
There were no significant differences between the two study
groups (p>0.05).
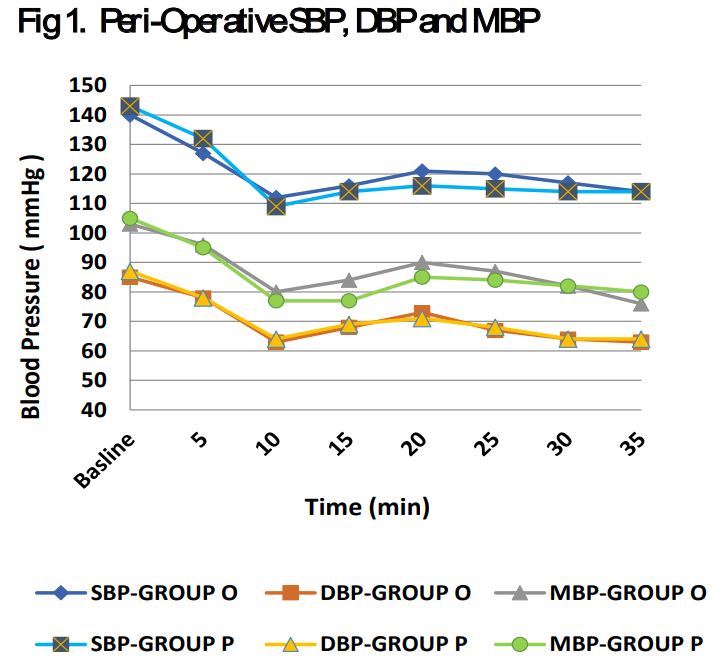
There was no statistical difference in maternal blood pressure
(SBP, DBP, MBP) between the two study groups at the eighth time
periods of the study (P>0.05), however there was statistically difference within each group between the eight time periods and
between baseline and minute 35 in the same group (min 0 vs min
35) (P<0.05) (Figure 1).
Phenylephrine requirements, more doses of phenylephrine
were administered in the group P compared to group O. Quarter
of the mothers (12 women, 24%) in the group O compared to half
of the mothers (25 women, 50%) in the group P, received at least
one dose (50 mcg) of phenylephrine during the 35 minutes post
SA (P=0.007). From the other side, no difference was observed in
the total amount of phenylephrine dose between the two groups
(P>0.05), group O (mean ± SD 96±58 mcg/ median 100) VS group
P (mean ± SD 120±75 mcg/ median 100) (Table 2).
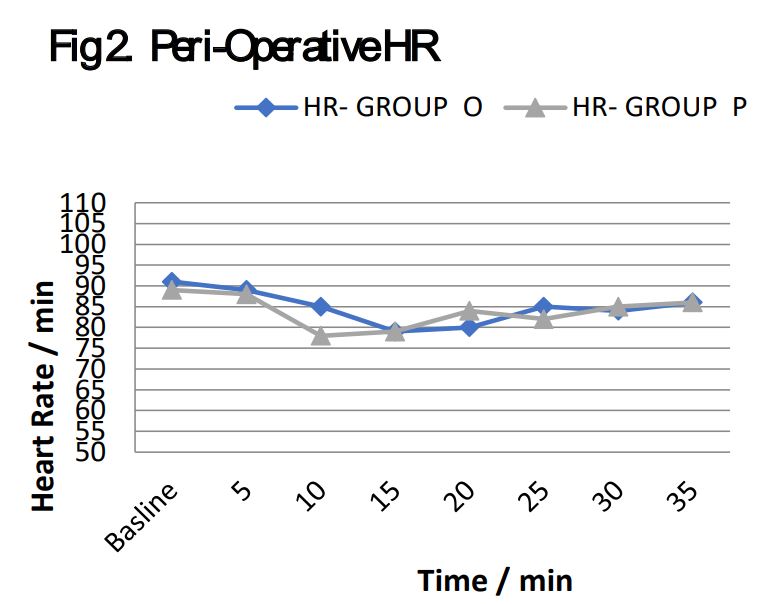
Heart Rate and Bradycardia, comparing the HR at the eight
time periods between the two study groups, there were no significant differences (P>0.05). In addition, the difference in HR between baseline and 35 minutes post SA in each one of the groups
was also not statistically significant (P>0.05) (Figure 2).
The incidence of bradycardia was similar between the two
study groups, 3 patients (6%) in group O and 5 (10%) in the group
P, received one dose (0.5 mg) of IV Atropine during the 35 minutes
post SA (P>0.05).
Table 2: Phenylephrine requirements by study group.
|
|
Group O N=50 |
Group P N=50 |
P value |
Parturient received
medication
Total
amount
(mcg)
|
number (%)
median
mean
SD
95% C.I.
|
12(24)
100
96±58
[59-133]
|
25(50)
100
120±75
[89-151]
|
├0.0070*
˧
0.4439**
|
*Data are numbers (%), P value by ├chi square test;
**P value between two study groups by ˧ Wilcoxon rank sum test
Table 3: Adverse events by study group during the 35 minutes
post SA induction.
|
Group O
(n=50) |
Group P
(n=50) |
├P value |
Nausea and vomiting
Number
of parturient with at least
one event
in 35 min
|
9 (18) |
23 (46) |
0.0060 |
Dizziness
Number of
parturient with at least one
event
in 35 min
|
14 (28) |
20 (40) |
0.2050 |
Data are numbers (%). P value between the two study groups by ├chi square test
Table 4: Fetal health data by study group.
|
Group O (n=50) |
Group O (n=50) |
P value |
| APGAR |
| 10 |
36 (72.0) |
33 (66.0) |
┴0.3310 |
| 9 |
14 (28.0) |
14 (28.0) |
|
| 8 |
|
3 (6.00) |
|
| Umbilical cord blood pH |
7.31±0.04 [7.2-7.4] |
7.27±0.06 [7.1-7.4] |
†0.0006 |
Data are mean SD and [range] or numbers (%); P value between the two study
groups by †2- sample T-test for differences of mean or ┴Fisher exact test
Adverse events analysis
During the 35 minutes post SA, in group P there were more
events of nausea and vomiting (46%) of the mothers compared
to only about a sixth (18%) in the group O. Incidence of dizziness
during the 35 minutes post SA induction between the two groups
was almost similar (P>0.05) (Table 3).
Fetal health outcome, a significantly higher mean of umbilical
cord blood pH was recorded in group O. Mean pH of umbilical
cord blood was 7.31 in group O and 7.27 in group P (P<0.05).
Similar APGAR score was observed at the first minute after delivery in the two study groups (P>0.05) (Table 4).
Discussion
This prospective study, detected the effect of prophylactic ondansetron on SAIH incidences and phenylephrine consumption in
mothers gave birth under SA indicates that prophylactic ondansetron does not decrease the incidence of SAIH directly after SA,
however, it decreases the need for vasopressor (reduction in the
number of mothers who required phenylephrine for the treating
SAIH) and that means clearly but indirectly that prophylactic ondansetron may mitigate the risks of SAIH.
Prophylactic ondansetron administration before SA in obstetric
patients to prevent SAIH is still conflicting. Previous studies have
demonstrated its efficacy in prevention SAIH in obstetric patients
but those studies were with small samples size [7,8]. Gao et al.
meta-analysis suggests that prophylactic ondansetron reduces
both the incidence of SAIH and vasopressor consumption in both
obstetric and non-obstetric patients, but there was a large heterogeneity and small samples size in the involved studies [9]. Another
meta-analysis of Heesen et al. also showed moderate effect in reducing the incidence of SAIH and bradycardia in obstetric patients
but in that analysis, studies with different types of 5-HT3 antagonists were involved [10]. In contrast, other studies showed that
prophylactic ondansetron may had very little effect, if any, on the
incidence of SAIH in healthy mothers undergoing SA [11]. Terkawi
et al. showed that ondansetron premedication does not attenuate hemodynamic changes after SA nor does it reduce the amount
of vasopressor use, pruritus, or nausea and vomiting [12]. Tubog
et al. conducted a systematic review and found that intravenous
ondansetron may mitigate the risks of SAIH and bradycardia following SA [13].
In this context, our study has a larger sample size (100 mothers
records) that detected the effect of prophylactic ondansetron on
attenuation of SAIH and phenylephrine consumption in mothers
gave birth under SA. We suggest our results indicate that ondansetron may attenuate BJR, produced by left ventricular mechanoreceptors stimulated by 5-HT, and can inhibit further expansion
of peripheral blood vessels, augment venous return to the heart
and result in less consumption requirement of vasopressor phenylephrine which means clearly but indirectly that prophylactic ondansetron may mitigate the risks of SAIH.
Prophylactic ondansetron that might cause BJR inhibition has
been proposed to explain the reduction in perioperative bradycardia accompanied with hypotension after SA [3,14]. In the present study, we did not observe a significant difference in the incidence of bradycardia between the two study groups. The possible
reasons may include the study design, doses of ondansetron, anesthetics (local and opioid) used for SA, or the vasopressor used
(phenylephrine), which approximately affecting bradycardia in
10% of the mothers receiving this vasopressor [15]. Further studies still needed to evaluate this relation
It is well known that ondansetron can reduce incidence and
severity of post-operative nausea and vomiting (PONV) after SA
[16,17], but there is restricted data on the intraoperative nausea
and vomiting (IONV). In this study, we noted that mothers received ondansetron had significantly less incidence of IONV. One
possible explanation for IONV attenuation may be that ondansetron can block part of the hemodynamic depression of SA by
inhibition of BJR, that augment venous return to the heart, and
can result to less reduction in cerebral hypo perfusion, and it is
well known that cerebral hypo perfusion may activate vomiting
centers in the medulla [18].
In this study, umbilical artery pH values were higher in group
O, however no statistical difference was observed in APGAR score
at the first minute after delivery. Trabelsi et al. [19] showed that
ondansetron can be helpful in improving metabolic acidosis, however, the exact reason is yet unknown for this result. Further studies still be needed to establish this assumption.
Limitations: There are some limitations to the study, subgroup
analysis on different ondansetron doses, was not included, neither other factor such as anesthetic drugs and doses, and fluid
type and volume. No safety data with respect to the side effects
of ondansetron such as shivering, headache, electrocardiographic
changes or acute myocardial ischemia, and no comparison analysis of the risk-benefit balance between the possible benefits of
ondansetron versus its potential side effects.
Conclusion
The study illustrates that prophylactic ondansetron 4 mg, administered IV, five minutes before SA, although it did not attenuate SAIH directly, but it decreased significantly the need for the
vasopressor phenylephrine, which means clearly but indirectly
that prophylactic ondansetron can mitigate the risks of SAIH.
References
- Butwick AJ, Columb MO, Carvalho B. Preventing spinal hypotension during caesarean delivery: what is the latest? Br J Anaesth. 2015; 114: 183-6.
- Mercier FJ, Auge M, Hoffmann C, Fischer C, Le Gouez A. Maternal hypotension during spinal anesthesia for caesarean delivery. Minerva Anestesiol 2013; 79: 62-73.
- Cheryl Chooi, Julia J Cox, Richard S Lumb, Philippa Middleton, Mark Chemali, Richard S Emmett, Scott W Simmons, Allan M Cyna.Technique for preventing hypotension during spinal anesthesia for caesarean section. Cochrane Systematic Review - Intervention Version published. 2017.
- Taufik MM, Hayes SM, Jacoub FY, Badran BA, Gohar FM, Shabana AM, Abdelhalek M, Emara MM. Comparison between colloid preload and crystalloid co-load in cesarean section under spinal anesthesia: a randomized controlled trial. Int J Obs. 2014; 23(4): P317-323.
- Campagna JA, Carter C. Clinical relevance of the Bezold–Jarisch reflex. Anesthesiology. 2003; 98: 1250-60.
- Lin FQ, Qiu MT, Ding XX, Fu SK, Li Q. Ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean section: an updated meta-analysis. CNS Neursci Ther. 2012; 18(7): 591-7.
- Sahoo T, SenDasgupta C, Goswami A, Hazra A. Reduction in spinalinduced hypotension with ondansetron in parturients undergoing caesarean section: A double-blind randomized, placebo-controlled study. Intern J of Obstet Anest. 2012; 21: 24-28.
- Owczuk R, Wenski W, Polak-Krzeminska A, et al. Ondansetron given intravenously attenuates arterial blood pressure drop due to spinal anesthesia: a double-blind, placebo-controlled study. Reg Anesth Pain Med. 2008; 33: 332-9.
- Gao L, Zheng G, Han J, Wang Y, Zheng J. Effect of prophylactic ondansetron on spinal anesthesia-induced hypotension: a metaanalysis. Intern J Obstet Anesth. 2015; 24(4): 335-43.
- Heesen M, Klimek M, Hoeks SE, Rossaint R. Prevention of spinal anesthesia-induced hypotension during cesarean delivery by 5-hydroxytryptamine-3 receptor antagonists: a systematic review and meta-analysis and meta-regression. Anesth Analg. 2016; 123: 977-88.
- Ortiz-Gomez JR, Palacio-Abizanda FJ, Morillas-Ramirez F, FornetRuiz I, Lorenzo-Jimיnez A, Bermejo-Albares ML. The effect of intravenous ondansetron on maternal haemodynamics during elective caesarean delivery under spinal anaesthesia: a doubleblind, randomised, placebo-controlled trial. Int J Obstet Anesth. 2014; 23: 138-43.
- Terkawi AS, Tiouririne M, Mehta SH, Hackworth JM, Tsang S, Durieux ME. Ondansetron does not attenuate hemodynamic changes in patients undergoing elective cesarean delivery using subarachnoid anesthesia: a double-blind, placebo-controlled, randomized trial. Reg Anesth Pain Med. 2015; 40: 344-8.
- Tubog TD, Kane TD, Pugh MA. Effects of ondansetron on attenuating spinal anesthesia-induced hypotension and bradycardia in obstetric and non obstetric subjects: a systematic review and metanalysis. AANA J. 2017; 85: 113-22.
- Somboonviboon W, Kyokong O, Charuluxananan S, et al. Incidence and risk factors of hypotension and bradycardia after spinal anesthesia for cesarean section. J Med Assoc Thai. 2008; 91: 181-7.
- Veeser M, Hofmann T, Roth R, Klöhr S, Rossaint R, Heesen M. Vasopressors for the management of hypotension after spinal anesthesia for elective caesarean section. Systematic review and cumulative meta-analysis. Acta Anaesthesiol Scand. 2012; 56: 810-816.
- George RB, Allen TK, Habib AS. Serotonin receptor antagonists for the prevention and treatment of pruritus, nausea, and vomiting in women undergoing cesarean delivery with intrathecal morphine: a systematic review and meta-analysis. Anesth Analg. 2009; 109: 174-182.
- Bonnet MP, Marret E, Josserand J, Mercier FJ. Effect of prophylactic 5-HT3 receptor antagonists on pruritus induced by neuraxial opioids: a quantitative systematic review. Br J Anaesth. 2008; 101: 311-319.
- M Balki, JCA Carvalho. Intraoperative nausea and vomiting during cesarean section under regional anesthesia. International Journal of Obstetric Anesthesia. 2005; 14: 230-241.
- Trabelsi W, Romdhani C, Elaskri H, et al. Effect of ondansetron on the occurrence of hypotension and on neonatal parameters during spinal anesthesia for elective caesarean section: a prospective, randomized, controlled, double-blind study. Anesthesiol Res Pract. 015; 2015: 158061.