Introduction
Basilar thumb arthritis is a common and debilitating condition affecting over 30% of postmenopausal women [1]. Patients
experience significant pain and reduction in thumb strength,
particularly thumb abduction and key-pinch [2,3]. Nonoperative
management consisting of splinting, physical therapy, pain medication, and joint injection do not correct underlying pathology
and generally do not provide satisfactory long-term outcomes
[4]. Operative management includes joint arthrodesis, arthroplasty, and trapeziectomy with or without suspension of the first
metacarpal via ligament reconstruction and tendon interposition
(LRTI). While trapeziectomy with LRTI is the most prevalent [5,6],
high-quality evidence has not demonstrated any technique to be
definitively superior [7].
Carpometacarpal (CMC) joint fusion can provide symptomatic
relief but may accelerate arthritis in the adjacent scaphotrapeziotrapezoidal and metacarpophalangeal (MCP) joints and is associated with a 13% risk of nonunion [8]. Trapeziectomy with LRTI
for treatment of CMC arthritis was first described over 70 years
ago and provides a good balance of symptomatic pain relief and
maintenance of functional status [9]. However, patients generally report decreases in strength, including thumb abduction and
key-pinch motions postoperatively [7]. Additionally, the removal
of the trapezium results in a loss of height that invariably progresses in the following decade [10]. Short-term follow-up studies
have not indicated clinical sequlae [11,12];however, longer- term
studies (greater than 7 years) have shown a negative correlation
between degree of subsidence and functional outcomes [13].
Basilar thumb implants were first described in the early 1970s
and included silicone implants, such as those utilized by Swanson
[14,15], as well as metal-on-polyethylene designs described by de
la Caffiniere and Aucouturier in 1973 [16]. While initially promising, various barriers limited widespread adoption. Appropriate
sizing of the implant could be technically challenging, particularly
in the case of monoblock systems, and complications such as CMC
subluxation, silicone synovitis, or aseptic loosening frequently
necessitated revision surgery [17-20]. Although there have been
numerous advances in material science, implant design, and technique since then, various challenges persist, with patients reporting varying degrees of functional improvement postoperatively.
The BioPro® Modular Thumb Implant (BioPro, Port Huron, MI)
is a more recent basilar thumb hemiarthroplasty system that has
seen growing use. Advantages over previous systems include its
material composition, modularity, and geometry that better approximates native thumb anatomy. The implant is composed of
cobalt-chrome, although an all-titanium version is also available.
It has modularity of both the metacarpal stem and head components. Modular heads permit better fit to the patient’s trapezium
to facilitate force distribution and socket congruency, while the
ability to adjust stem length enables more precise soft-tissue tensioning. The stem component has two additional features: varus
angulation and titanium spray coating. Increased varus angulation better approximates native thumb anatomy and biomechanics. This, in turn, theoretically reduces subluxation risk. The titanium plasma spray coating allows for cementless fixation of the
component with associated bony ingrowth. This may have the
benefit of mitigating implant subsidence and loosening. The goal
of this study is to evaluate the efficacy of the BioPro® implant in the treatment of CMC arthritis. Outcomes of particular interest
include pain reduction, postoperative gains or losses in functional
status, and device survivorship.
Materials and methods
This is a retrospective single-cohort study of 95 patients (110
thumbs, 15 bilateral implants) with Eaton-Littler Stage II or III
osteoarthritis of the trapeziometacarpal joint who were treated
with a basilar thumb hemiarthroplasty using the BioPro® Modular Thumb Implant between the years 2008 and 2016. The study
adhered to the Strengthening the Reporting of Observational
Studies in Epidemiology (STROBE) guidelines. Exclusion criteria included prior infection of the operative hand, presence of
Eaton-Littler Stage IV osteoarthritis (for which other treatments
are indicated), or prior diagnosis of inflammatory-type arthritis.
Prior to surgery, patients were requested to voluntarily complete
a preoperative qualitative assessment of their functional status
utilizing the QuickDASH (Disabilities of the Arm, Shoulder and
Hand) survey, as well undergo bilateral strength measurements
of the hands. These measurements included grip strength, tip
pinch, three-jaw-chuck, and key pinch. Strength measurements
were obtained utilizing a calibrated dynamometer set consisting
of 2 separate devices for hand and pinch strength, respectively.
At the first follow-up visit more than 6 weeks postoperatively, patients were again requested to complete a QuickDASH form and
repeat strength measurements using the same dynamometer
set. For patients that recorded multiple sets of data over serial
follow-up appointments, the most recent data set was used in
the final analysis. Pre- and postoperative QuickDASH scores were
compared using a 2-tailed paired t test with statistical significance
considered at P<0.05.
Results
Of the 95 total patients (110 thumbs) who elected to undergo
thumb arthroplasty, 31 patients were male (37 thumbs, 33.6%)
and 64 female (73 thumbs). Average patient age at date of service was 61 years (standard deviation [SD]=9.1). Average duration between surgery and final recorded follow-up was 3.8 years
(SD=2.5). Relevant data are summarized in Table of the original
110 thumbs, 40 thumbs (17 male, 42.5%; 23 female) recorded
both a pre- and postoperative QuickDASH. This subpopulation
was comparable to the general study population in terms of age
(59 years, SD=9.0) and average final follow-up (4.0 years, SD=1.9).
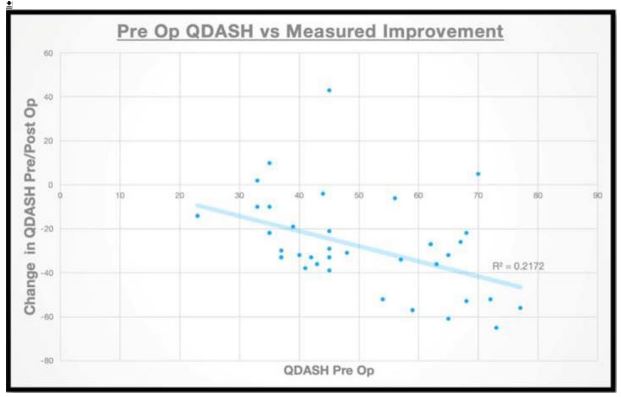
The average QuickDASH scores were 49.55 (SD=14.6) preoperatively and 20.8 (SD=22.7) postoperatively. This decrease was statistically significant (P<0.00001). Higher preoperative QuickDASH
score was correlated with increased improvement (R2=-0.212)
across the entire study population (Figure 1). Women on average
reported slightly higher preoperative QuickDASH scores (49.84)
and slightly greater postoperative improvement (-29.2) compared
to men (52.17 and -25.53). A further subpopulation of 9 thumbs
had at least 2 postoperative QuickDASH scores that could be
trended. In this subpopulation, average preoperative QuickDASH
was 54.11 (SD=9.4). Average initial QuickDASH measurement occurred 2.0 years postoperatively, with an average score of 19.33
(SD=17.9). Average final QuickDASH was measured 6.2 years
postoperatively (SD=1.3), with average QuickDASH score of 14.44
(SD=14.2), representing an additional decrease of 4.89 points.
While 43 thumbs had postoperative assessment, only 10 (5 male, 5 female) of these had corresponding preoperative data
and were thus considered in the analysis. None of these thumbs
represented bilateral implants. Additionally, 7 thumbs were left
thumbs and 3 thumbs were right thumbs; hand dominance was
not available. Average age at surgery was 57 years (SD=10). Average final follow-up was 5.0 years (SD=1.5). The relevant data are
summarized in Table 2. Of the original 110 thumbs, there were
13 postoperative complications requiring revision. The most common cause was titanium metal allergy (5 thumbs), followed by
postoperative trapezium fracture (2 thumbs), persistent pain with
revision to LRTI (2 thumbs), infection (1 thumb), and instability
resolved with head upsizing (1 thumb). Two thumbs were revised
without a documented reason. Four thumbs with titanium allergy
were revised to a NuGrip (LMT Surgical, Milton QLD, Australia)
pyrocarbon implant and the fifth thumb was revised to LRTI. None
of the 110 thumbs dislocated at any point postoperatively. These
results are summarized in Table 3.
Table 1:Participants’ demographics, clinical characteristics and statistics of differences between groups.
|
DCD |
TD |
p |
| N |
21 |
20 |
|
| Gender (Male:Female) |
16:5 |
11:9 |
.15 |
| Age (mean years ± SD |
7y9m ± 1.5 |
7y8m ± 1 |
.75 |
|
IQ (mean standard score ±
SD)
|
99.9 ± 14 |
- |
|
|
mABC2 Me percentile (IQR)
|
5 (2.7-5) |
63 (50-77.2) |
<.001 |
|
mABC2 manual dexterity Me
percentile (IQR)
|
5 (2-9) |
50 (25-75) |
<.001 |
|
DCDQ’07 Me total score (IQR)
|
39 (35-42) |
66 (60-69) |
<.001 |
|
Co-occuring diagnosis (N(%))
|
| Pure DCD |
3 (14%) |
- |
|
| Language Disorders |
6 (29%) |
- |
|
| Learning Disorders |
2 (10%) |
- |
|
|
ADHD, language disorders,
behavioural problems,
learning disorders or ASD
|
19 (90%) |
- |
|
DCD: children with Developmental Coordination Disorder; TD: typically developing children; M, male; F: female; Me:
median; IQR: interval quartile range; IQ: intelligence quotient; mABC-2: Movement ABC-2 test; ADHD: attention deficit
hyperactivity disorder; ASD: autism spectrum disorder.
Table 2: Prevalence of intestinal parasitic infections and infection rate among immunocompromised and control groups.
| Parasite |
Hemodialysis N (%) |
Chemotherapy N (%) |
Total of immunocompromised N
(%)
|
Control N (%) |
P value |
| Blastocystis hominis |
28 (10.1%) |
29 (8%) |
57 (8.9%) |
16 (4%) |
|
| Entamoeba coli |
7 (2.5%) |
3 (0.8%) |
10 (1.6%) |
1 (0.25%) |
|
| Endolimax nana |
2 (0.7%) |
2 (0.6%) |
4 (0.6%) |
1 (0.25%) |
|
| Iodamoeba butschlii |
2 (0.7%) |
3 (0.8%) |
5 (0.8%) |
2 (0.5%) |
|
| Chilomastix mesnili |
2 (0.7%) |
1 (0.3%) |
3 (0.5%) |
1 (0.25%) |
|
| Giardia lamblia |
0 (0%) |
0 (0%) |
0 (0%) |
8 (2%) |
|
| Cryptosporidium spp. |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
|
Strongyloides stercoralis
|
1 (0.36%) |
2 (0.55%) |
3 (0.5%) |
0 (0%) |
|
| Taenia spp. |
0 (0%) |
1 (0.28%) |
1 (0.15) |
0 (0%) |
|
| Infected |
42 (15%) |
41 (11.3%) |
83 (13%) |
29 (7.3%) |
0.008 |
| Non-infected |
237 (85%) |
321 (88.7%) |
558 (87%) |
370 (92.7%) |
|
Table 3: Multivariate analysis.
| Variables |
PFS |
OS |
STFS* |
|
HR |
p-value |
HR |
p-value |
HR |
p-value |
| Age (per year) |
- |
- |
1.01 (0.99-1.02) |
0.23 |
- |
- |
|
Karnofsky index (per 10%)
|
0.93 (0.81-1.07) |
0.3 |
0.96 (0.82-1.12) |
0.75 |
0.88 (0.69-1.12) |
0.3 |
| FNCLCC grade (3 vs 1-2) |
2.64 (1.87-3.73) |
<0.001 |
2.47 (1.72-3.55) |
<0.001 |
2.88 (1.54-5.4) |
0.001 |
|
AJCC T stage (T3-4 vs T1-2)
|
2.47 (1.48-4.12) |
<0.001 |
3.63 (2.05-6.43) |
<0.001 |
5.11 (1.86-13.99) |
0.002 |
| EQD2 (≥64 vs <64 Gy) |
- |
- |
0.47 (0.28-0.81) |
0.007 |
0.53 (0.20-1.41) |
0.2 |
| Presentation |
|
|
|
|
|
|
| Unresected 1° tumor |
- |
Ref |
- |
Ref |
- |
Ref |
| R2 resected 1° tumor |
0.61 (0.29-1.25) |
0.18 |
0.35 (0.15-0.82) |
0.016 |
0.47 (0.08-2.75) |
0.4 |
| Unresected recurrence |
1.42 (0.82-2.44) |
0.21 |
1.24 (0.71-2.17) |
0.44 |
3.85 (1.41-10.48) |
0.008 |
*In patients who had not received prior systemic treatment.
AJCC: American Joint Committee On Cancer; EQD2: Equivalent Dose In 2 Gy Fractions; LF: Local Failure; OS: Overall
Survival; PFS: Progression-Free Survival; STFS: Systemic Treatment-Free Survival.
Discussion
Trapeziectomy with LRTI has a proven effective history in the
surgical management of CMC arthritis. It provides good pain relief
while maintaining acceptable thumb mobility and strength. Surveys of current practice show that it remains the dominant treatment modality [5,6]. CMC arthroplasty represents an alternative
intervention with the ability to provide comparable, or even superior outcomes. While still performed by a minority of surgeons, it
has grown in popularity, aided by advancements in surgical techniques, material science, and implant design [5]. However, there
remains a paucity of data regarding outcomes, especially with
newer implant designs.
In this study, qualitative data from pre- and postoperative
QuickDASH scores demonstrated a dramatic reduction in our
patients’ pain and associated improvement in functional status.
For patients with a completepre- and postoperative QuickDASH
assessment, average improvement was 34.78 points at initial
average 1.99 year follow-up, and this further improved an additional 4.89 points at secondary 6.16 year follow-up. These results
are comparable to other QuickDASH outcomes in the literature
regarding CMC arthroplasty. For example, [21] demonstrated a
21.2 QuickDASH point decrease at mean 4.1 year follow-up with
a Stryker Ivory prosthesis. While no LRTI data has been currently
collected by the authors for direct comparison, other meta-analyses have shown CMC arthroplasty to outperform LRTI with regard to short-term functional outcomes [22]. Found an average
4.8 point greater improvement in patients treated with joint
replacement, found an average 4.3 point greater improvement;
the follow-up intervals of the studies were highly varied [23]. Proposed minimum clinically important difference (MCID) values for
QuickDASH range from 6.8 to 15,24,25. Depending on the methods and sample population used to anchor. This suggests that the
aforementioned difference is not clinically realized. However, it is
worth investigating this conclusion in more detail. As noted earlier, a greater degree of improvement in our patients was seen
in those with greater preoperative impairment. While this is not
surprising, it would be interesting to examine the strength of this
trend in an LRTI population. Patients of varying preoperative disability may realize differing benefits of LRTI vs joint replacementtype procedures, and the relative differences seen in these subpopulations may exceed MCID. Quantitative strength data using
a dynamometer was statistically underpowered. No statistically
significant differences in pre- and postoperative strength were
found. However, the available data suggests a trend of superior
outcomes in the operative hand compared to the nonoperative
hand. This aspect of the study represents a potential avenue for
additional study, with additional effort taken to capture preoperative data for future comparisons. The currently available data can
be used to augment further analysis.
Total survivorship of the original implants was 88.18% at the
mean follow-up of 3.8 years. The most common reason for revision was titanium metal allergy. Four of these cases were successfully resolved with revision to a non-titanium joint replacement
implant and a fifth underwent revision to LRTI without sequelae.
A complication with similar presentation was observed in the experience of Thorkildsen and Røkkum [26]with the Electra implant,
which features a titanium stem, and warrants future investigation.
A total of 5 thumbs underwent revision to LRTI for trapezium fragmentation (n=2), persistent pain (n=2), and allergy (n=1).
Notably, none of the implants loosened nor dislocated, which
represent the most common complications of CMC arthroplasty
necessitating revision as documented in the literature [27].A single thumb was revised to a larger head due to subjective instability without dislocation, with subsequent resolution of symptoms.
Overall, these results represent a complication rate comparable
to or lower than multiple other prostheses [27,28], though still
higher than LRTI [27].
Pritchett and Habrylhave previously published on their experiences with the BioPro® implant in a population of 159 thumbs
[29]. In their study, the implant had a 6-year survivorship of
94% and no dislocations, again suggesting its inherent resilience
against this particular complication. The authors posited this was
due to the varus stem angulation and modular nature of the implant’s head permitting more accurate filling of the trapezium.
Their surgical technique is well-documented, and we concur that
appropriate operative technique is vital to optimizing component
positioning and achieving satisfactory outcome.
As the understanding of CMC arthritis and its treatment continues to advance, the viability of CMC arthroplasty continues to be
validated. This paper represents another large-population cohort
of thumbs that have obtained excellent short- to intermediateterm outcomes with the BioPro® implant. While complications
with the implant are higher than LRTI, joint replacement surgery
never precluded successful revision to satisfactory outcome. As
the studied patient population matures, further functional outcome trends will be of particular interest. A long-term sequelae of
the LRTI procedure is metacarpal subsidence with resulting biomechanical disadvantage [12]. It is possible that a relative advantage of arthroplasty to LRTI is only realized in the long term, after
the impacts of metacarpal subsidence become apparent.
Declarations
Conflicts of interest: John J. Faillace has received payments in
the form of royalty/license from Extremity Medical and BioPro,
travel/lodging and honoraria from BioPro, current or prospective
ownership interest from Tyber Medical LLC, and food and beverage from Stryker Corporation, BioPro, Sanara MedTech, Endo
Pharmaceuticals, and AXOGEN in the last 5 years. The other authors have no conflicts of interest to declare.
Source of funding: None.
References
- Armstrong AL, Hunter JB, Davis TR. The prevalence of degenerative arthritis of the base of the thumb in post-menopausal women. J Hand Surg Br. 1994; 19(3): 340-341. 10.1016/02667681(94)90085-x
- Gottschalk MB, Patel NN, Boden AL, Kakar S. Treatment of basilar thumb arthritis: a critical analysis review. JBJS Rev. 2018; 6(7): e4. 10.2106/jbjs.Rvw.17.00156
- Garfjeld Roberts P, Riley N. Basal thumb arthritis. Orthop Trauma. 2023; 37(2): 104-110. https: //doi.org/10.1016/j.mporth.2023.01.003
- Bakri K, Moran SL. Thumb carpometacarpal arthritis. Plast Reconstr Surg. 2015; 135(2): 508520. 10.1097/prs.0000000000000916
- Yuan F, Aliu O, Chung KC, Mahmoudi E. Evidence-based practice in the surgical treatment of thumb carpometacarpal joint arthritis. J Hand Surg Am. 2017; 42(2): 104- 112.e101. 10.1016/j.jhsa.2016.11.029
- Deutch Z, Niedermeier SR, Awan HM. Surgeon preference, influence, and treatment of thumb carpometacarpal arthritis. Hand (N Y). 2018; 13(4): 403-411. 10.1177/1558944717717506
- Challoumas D, Murray E, Ng N, Putti A, Millar N. A meta-analysis of surgical interventions for base of thumb arthritis. J Wrist Surg. 2022; 11(6): 550-560. 10.1055/s- 0042-1743117
- Bamberger HB, Stern PJ, Kiefhaber TR, McDonough JJ, Cantor RM. Trapeziometacarpal joint arthrodesis: a functional evaluation. J Hand Surg Am. 1992; 17(4): 605-611. 10.1016/03635023(92)90302-6
- Newton A, Talwalkar S. Arthroplasty in thumb trapeziometacarpal (CMC joint) osteoarthritis: An alternative to excision arthroplasty. J Orthop. 2023; 35: 134-139. 10.1016/j.jor.2022.11.011
- Tomaino MM, Pellegrini VD, Jr., Burton RI. Arthroplasty of the basal joint of the thumb. Longterm follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am. 1995; 77(3): 346-355. 10.2106/00004623-199503000-00003
- Yang SS, Weiland AJ. First metacarpal subsidence during pinch after ligament reconstruction and tendon interposition basal joint arthroplasty of the thumb. J Hand Surg Am. 1998; 23(5): 879-883. 10.1016/s0363-5023(98)80167-6
- Downing ND, Davis TR. Trapezial space height after trapeziectomy: mechanism of formation and benefits. J Hand Surg Am. 2001; 26(5): 862-868. 10.1053/jhsu.2001.27761
- Moineau G, Richou J, Liot M, Le Nen D. Prognostic factors for the recovery of hand function following trapeziectomy with ligamentoplasty stabilisation. Orthop Traumatol Surg Res. 2009; 95(5): 352358. 10.1016/j.otsr.2009.03.015
- Swanson AB. Flexible implant arthroplasty for arthritic finger joints: rationale, technique, and results of treatment. J Bone Joint Surg Am. 1972; 54(3): 435-455.
- Swanson AB. Disabling arthritis at the base of the thumb: treatment by resection of the trapezium and flexible (silicone) implant arthroplasty. J Bone Joint Surg Am. 1972; 54(3): 456471.
- de la Caffiniere JY, Aucouturier P. Trapezio-metacarpal arthroplasty by total prosthesis. Hand. 1979; 11(1): 41-46. 10.1016/s0072-968x(79)80007-8
- Tägil M, Kopylov P. Swanson versus APL arthroplasty in the treatment of osteoarthritis of the trapeziometacarpal joint: a prospective and randomized study in 26 patients. J Hand Surg Br. 2002; 27(5): 452-456. 10.1054/jhsb.2002.0836
- van Cappelle HG, Deutman R, van Horn JR. Use of the Swanson silicone trapezium implant for treatment of primary osteoarthritis : long-term results. J Bone Joint Surg Am. 2001; 83(7): 9991004. 10.2106/00004623-200107000-00004
- August AC, Coupland RM, Sandifer JP. Short term review of the De La Caffiniere trapeziometacarpal arthroplasty. J Hand Surg Br. 1984; 9(2): 185-188.
- Chakrabarti AJ, Robinson AH, Gallagher P. De la Caffinière thumb carpometacarpal replacements. 93 cases at 6 to 16 years follow-up. J Hand Surg Br. 1997; 22(6): 695-698. 10.1016/s0266-7681(97)80427-5
- Cebrian-Gomez R, Lizaur-Utrilla A, Sebastia-Forcada E, LopezPrats FA. Outcomes of cementless joint prosthesis versus tendon interposition for trapeziometacarpal osteoarthritis: a prospective study. J Hand Surg Eur Vol. 2019; 44(2): 151-158. 10.1177/1753193418787151
- Raj S, Clay R, Ramji S, Shaunak R, Dadrewalla A, Sinha V, et al. Trapeziectomy versus joint replacement for first carpometacarpal (CMC 1) joint osteoarthritis: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol. 2022; 32(6): 1001-1021. 10.1007/s00590-02103070-5
- Qureshi MK, Halim UA, Khaled AS, Roche SJ, Arshad MS. Trapeziectomy with ligament reconstruction and tendon interposition versus trapeziometacarpal joint replacement for thumb carpometacarpal osteoarthritis: a systematic review and meta- analysis. J Wrist Surg. 2022; 11(3): 272-278. 10.1055/s-0041-1731818
- Franchignoni F, Vercelli S, Giordano A, Sartorio F, Bravini E, Ferriero G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J Orthop Sports Phys Ther. 2014; 44(1): 30-39. 10.2519/jospt.2014.4893
- Kazmers NH, Qiu Y, Yoo M, Stephens AR, Tyser AR, Zhang Y. The minimal clinically important difference of the PROMIS and QuickDASH instruments in a nonshoulder hand and upper extremity patient population. J Hand Surg Am. 2020; 45(5): 399-407.e396. 10.1016/j.jhsa.2019.12.002
- Thorkildsen RD, Røkkum M. Trapeziectomy with LRTI or joint replacement for CMC1 arthritis, a randomised controlled trial. J Plast Surg Hand Surg. 2019; 53(6): 361-369. 10.1080/2000656x.2019.1635490
- Ganhewa AD, Wu R, Chae MP, Tobin V, Miller GS, Smith JA, et al. Failure rates of base of thumb arthritis surgery: a systematic review. J Hand Surg Am. 2019; 44(9): 728- 741.e710. 10.1016/j.jhsa.2019.05.003
- Holme TJ, Karbowiak M, Clements J, Sharma R, Craik J, Ellahee N. Thumb CMCJ prosthetic total joint replacement: a systematic review. EFORT Open Rev. 2021; 6(5): 316- 330. 10.1302/2058-5241.6.200152
- Pritchett JW, Habryl LS. A promising thumb basal joint hemiarthroplasty for treatment of trapeziometacarpal osteoarthritis. Clin Orthop Relat Res. 2012; 470(10): 2756-2763. 10.1007/s11999-012-2367-7.