Introduction
Hidradenitis Suppurativa (HS) or Acne Inversa is a chronic,
inflammatory, skin disease with periods of exacerbations or relapses. Poorly understood and debilitating, the disease presents
varying degrees of refractoriness to conventional dermatological
treatments [2]; It affects men and women of different age groups,
reduces the quality of life, well-being and mental health of patients, in addition to being frequently associated with low levels
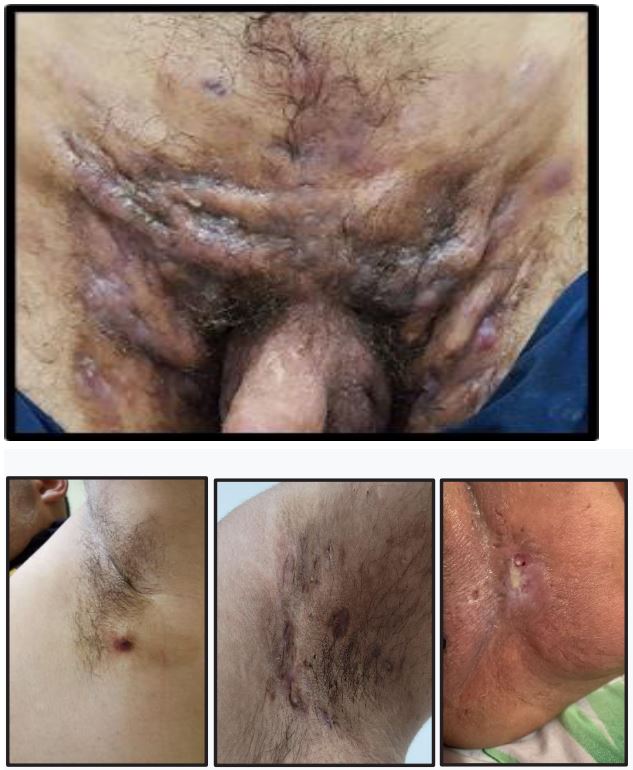
of human development [3]. Clinically, it manifests as multiple papules, nodules and abscesses in flexural areas of the body such as
armpits, inguinal and perigenital regions and perineum [4], as well
as in non-flexural areas such as legs, dorsal and pectoral regions,
ears and penis [5]. HS can also manifest in unusual locations such
as the abdomen, amputation stump, cesarean scar, chest, dorsal
region of the foot, eyelids, knees, post-auricular region and scalp
[6]. There are reports of involvement of the follicular portion of
the pilosebaceous units [7] and genetic predisposition [8], and associations with significant comorbidities such as smoking, obesity,
metabolic syndrome and diabetes mellitus [9,10].
Theoretical foundation
It is believed that acne conglobata, hidradenitis suppurativa
and perifolliculitis capitis are due to follicular occlusion resulting
from hyperkeratinization of the intradermal follicular portion of
the hair follicle [11].
Anatomically, the hair follicle is found in the surface regions
of the skin, except lips, palms and soles; It is made up of three
segments (upper or infundibulum, middle or isthmus, lower or
bulb), and performs thermoregulation and wound healing functions [12]. Although its intrinsic mechanism of pathogenicity has
not yet been completely elucidated, it is inferred that the formation of the lesion is related to follicular hyperkeratosis within the
pilosebaceous unit, characterizing HS as a hair follicle disease [13]
associated with secondary inflammation of the apocrine glands
[14].
The pathophysiology is not yet fully understood, the histopathological findings show that the initial lesion of HS is an occlusive
infundibulitis with a predominance of T cells in the lymphocytic
cell population [15]. The disease is multifactorial, recurrent and
scarring, and keratotic occlusion of the hair follicle may be the initiating event [16]. Follicular hyperkeratosis and perifollicular lymphocytic and subepidermal inflammation appear to be the initial
patterns favoring cyst formation [17]. Such events, driven by factors such as genetic predisposition (changes in genes that encode
essential elements of the y-secretase complex – PSENEN, PSEN1
or NCSTN) [18] or external factors such as skin microbiome, obesity, smoking and mechanical friction. The microbiome of damaged
skin differs significantly when compared to normal skin, and an
altered microbiome plays a relevant role in the onset of HS [18].
Furthermore, intrinsic defects in keratinocyte function favor inflammation in HS. Keratinocytes recruit high concentrations of immune cells to the injured epidermis and the interaction between
chemokines (CCL2, CCL3 and CXCL3), neutrophils, CD8 T cells and
natural killer cells favors the inflammatory condition in the epidermis [20]. Add to this the changes undergone by the stem cells
of the hair follicles and mainly by the cells of the external root
sheath, culminating in the activation of the ATR/CHK1 pathway
and the consequent increase in the number of micronodules and the presence of cytoplasmic ssDNA and finally the activation of
the IFI16/STING pathway and production of type I IFNs [21].
The rupture of the diseased follicle favors the release of its contents, that is, keratin fibers, dermal debris and molecular patterns
associated with damage and pathogens (DAMP, PAMP), attracting
more inflammatory cells. It is known that the cycles repeat themselves, the inflammation becomes chronic, favoring the formation
of scars and tunnels as well as the formation of cavities that unite
or deepen, creating conditions for infections and accumulation of
materials that result in suppurative and foul-smelling secretions.
It is possible that a bidirectional communication between the skin
microbiome and the patient’s immune response in skin damaged
by HS favors a positive diet that accounts for the chronicity of inflammation, tissue destruction and exacerbation of the disease
[22].
Regarding etiology, it is believed that HS may be the result of
an association of causes such as genetic predisposition, environmental, hormonal and microbiological factors that act as risk factors. Numerous scientific studies associate HS with mutations in
y-secretase genes and changes in the Notch signaling pathway [8];
changes in the skin microbiome [23]: elevations in pro-inflammatory cytokines [24]; changes in the innate immunity system [25];
the influence of hormonal factors, especially androgens [26];
physical factors such as mechanical stress [27] or environmental
factors such as obesity and smoking [28]. Recent work has sought
to establish, albeit broadly, a relationship between the disease
and social and economic factors [29].
The exact prevalence of HS is unknown. HS is a disease of
young adults with a predominance of females [30]; typically occurs after puberty [31]; it is more common in the second and third
decades of life, rare before the beginning of adolescence, and the prevalence is lower in elderly people [14]. It is rarely observed in
younger children and when it occurs, it is more common in children with a positive family history [32], and tends to be more severe in men.
It is estimated that HS has an estimated prevalence of 1% of
the world population. Prevalence estimates in North Hemisphere
range from <1 to 4% [10]. In the US, HS disproportionately affects
women, young adults and African Americans [33]. In Australia, the
prevalence of HS has been estimated at 0.67%. The individuals
were predominantly female, young, obese, smokers, unemployed
or with lower purchasing power [3]. In the Brazilian population,
the prevalence of HS was estimated at 0.41%. The age group from
13 to 24 years of age was the most affected, and females were the
most affected. Cross-sectional descriptive study with retrospective analysis of 194 patients, between 2005 and 2015, in, 74% of
the cases were female [34].
Age at the time of diagnosis varied between 10 and 67 years.
33% were diabetic; 55% were obese; and 61% were smokers. Hurley stage II was the most common at the time of diagnosis; and
the average time between the onset of the disease and diagnosis
was 9 years [35].
The scientific literature contains conflicting data on the epidemiology of HS. The prevalence disease depends on a variety
of factors. Taking into account where and how data is collected,
an extremely significant bias can be observed, highlighting a difficulty in collecting and extrapolating data [36].
The overall expression of the disease is disproportionate to
the estimated prevalence. The severity of the disease is described
according to Hurley’s three categories with the majority of cases
meeting criteria for mild or moderate disease [31].
Materials and methods
To assess the degree of impact HS of bio-psycho-socio-economic risk factors, the present Qualitative Systematic Review was
planned. The study in question aims to analyze the influence of
socioeconomic markers on the occurrence, severity and chronification of HS, as well as the relationship between such risk factors and the occurrence of the disease, in addition to innovative
aspects on the topic such as the impact of HS on women’s health
and correlation with oral health levels.
To evaluate the methodological quality of the included studies, the Higgins Bias Risk Analysis Tool for Randomized Clinical
Trials (Higgins 2011) and the AMSTAR Scale 2 (A Measurement
Tool to Assess Systematic Reviews 2) were applied [37], created
to evaluate the methodological quality of Quantitative Systematic
Reviews retrieved by search strategies.
The study in question aimed to analyze the influence of socioeconomic markers on the occurrence, severity and chronification
of HS, as well as the correlation between such risk factors and the
occurrence of the disease, in addition to evaluating new aspects
on the topic such as the impact of the disease on women’s health,
as well as the correlation with patients’ oral health levels. To this
end, a basic research question of a PICOT question (Problem, Intervention, Control, Result and Time) was organized. To this end,
MsSH (Medical Subjects Headings) were selected and included Hidradenitis Suppurativa, Acne Inversa and Verneuil’s Disease.
PICOT question: Which are the Bio-Psycho-Socioeconomic risk
factors that most interfere in the Evolution and Quality of Life of
Individuals with Hidradenitis Suppurativa?.
Submitted via Webliography in the electronic databases
Pubmed, Google Scholar and Cochrane Library, using specific
search strategies, in association with the Boolean operators OR,
AND and NOT. The following primary studies were selected (CaseControl Studies, Observational Studies and Randomized Clinical
Trials). Searches for qualitative and quantitative secondary clinical studies were also carried out in specific electronic databases.
Only articles in English published between 1990 and 2023 were
included in this study. Studies published in non-scientific newspapers and magazines, narrative reviews, theses, and monographs
were excluded. Among the selected articles, preference was given
to those with clearer analyzes related to the topic in question,
that is, articles that established some relationship between socioeconomic level and HA and/or comorbidities, seeking to clarify
the interrelationships between lifestyle of people and the diseases that affect them and how these diseases can be interconnected as causes or consequences of each other in a relationship
of interdependence.
Results
According to the review protocol, only one secondary clinical
research was retrieved from COCHRANE LIBRARY. A Quantitative
Systematic Review that fully completed the items of the AMSTAR
2 Scale, however two unfavorable aspects were observed (outdated review and not analyzing in detail the bio-psycho-socioeconomic aspects of the participants) and thus not meeting the
project inclusion criteria. Also in COCHRANE LIBRARY, 3 ongoing
randomized clinical trials were retrieved, with results that have
not yet been conclusive or published:
1. Etude de l’efficacité et de la tolérance du L35 versus placebo
dans le traitement de l’hidradénite suppurée (Maladie de Verneuil) - Hidradénite suppurée. EUCTR2006‐005405‐67‐FR. https://
trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2006-005405-67-
FR, 2007 | added to CENTRAL: 31 March 2019 | 2019 Issue 3.
2. Etude comparative randomisee intra-individuelle de
l’efficacite du traitement d’hidradenite suppuree ou maladie de
verneuil par injections sous cutanee de toxine botulinique versus
placebo - verneuil2006. EUCTR2007‐000534‐39‐FR. https://trialsearch.who.int/Trial2.aspx? TrialID=EUCTR2007-000534-39-FR,
2007 | added to CENTRAL: 31 March 2019 | 2019 Issue 3.
3. The effect of Botulinum Toxin type A in patients with axillary
Suppurative Hidradenitis. RBR‐4sp5w6. https://trialsearch.who.
int/Trial2.aspx?TrialID=RBR-4sp5w6, 2020 | added to CENTRAL:
31 October 2020 | 20 20 Issue 10.
The result is due to the scarcity and low quality of current scientific production on the subject. Therefore, it was decided to
carry out this review using a multifactorial analysis of bio-psychosocioeconomic risks, with 12 observational studies, with more
than 100 participants, in addition to 6 observational studies with
less than 100 participants.
The latter were chosen randomly, which resulted in 20 studies
in total, with a total of 3712 participants with those related to the
epidemiology of HS, and subjected to a pre-established research protocol. 18 studies were listed in the tables, except the study
on Oral and Systemic Health and Women’s Health. The extracted
data such as age, gender, race/color/ethnicity, education, income
and degree of severity of HS, according to the Hurley Classification, 1989 (Table 1) were stratified with the participation of two
more examiners, and later arranged in tables. Among the main
comorbidities and/or triggering or aggravating factors, smoking
and obesity were given greater importance. The study on Oral and
Systemic health totaled 102 participants [38]. The women’s health
study did not calculate the total number of participants [39].
Table 1: Hurley classification stage characteristics.
| Stage |
Characteristics |
| Stage I |
Formation of abscesses,
single or multiple, absence
of fistulas and
scars.
|
| Stage II |
Recurrent abscesses, single
or multiple, sparsely
separated, with the
presence
of fistulas or scars.
|
| Stage III |
Presence of multiple
abscesses, diffuse
involvement between them,
and
interconnected fistulas
throughout the affected
area.
|
Table 2: Study, participantes and soci aspectos socioeconômicos.
| Study |
Participants |
Gender |
Etnics |
Scholarity |
Job |
|
Lorite-Fuentes, I. et al.
2022 [40].
|
221 |
Male: 59 (26.30%)
Fem:
162 (73,30%)
|
|
|
|
|
Andrade, et al. 2015 [35].
|
123 |
Male: 32 (26%)
Fem: 91
(74%)
|
Caucasian: 94 (76%)
No-caucasian:
22 (18%)
Unknown: 7
(6%)
|
|
|
|
Katoulis, et al. 2017 [41].
|
152 |
Masc: 60 (39.5%)
Fem:
92 (60.5%).
|
|
|
Public Job: 13, Privat Job:
55
Liberal job: 29,
House wives:
15,
Students: 16, Pupils: 5,
Retirement:
4, Jobless: 15
|
Kluger, N; Ranta, M;
Serlachius,
M. 2017
[42].
|
26 |
Male: 10 (38.5%)
Fem:
16 ((61,5%)
|
Caucasian: 25/26 (96,2%)
African
descendent: 1 (3,8%)
|
High School or College:
57,5%
|
Annual Earnings between €
25.000
e 59.999: 58,3%;
Jobless:
16 (61,5%)
|
|
Delany, et al. 2017 [43].
|
150 |
Male: 45 (30,0%)
Fem:
105 (70,0%)
|
Caucasian: 143 (95,3%)
Black:
1 (0,7%)
Asian:
1(0,7%)
Others: 5
(3,5%)
|
|
Students: 16, Working: 76
Jobless:
32, Temporarely Inc: 4
Permanent
Inc: 10, Others: 12
|
|
Schultheis, M. et al. 2023
[44].
|
553 |
Male: 120 (21,7%)
Fem:
433 (78,3%)
|
|
N= 508:
Hig School:
35,2%
Professional
Qualification:
40,0%
College: 24,8%
|
Employment
relationship:
68,7% Jobess:
31,3%
|
| Loo, et al. 2018 [45] |
62 |
Male: 52 (83,9%)
Fem:
10 (16.1%)
|
Malaysian: 44 (71,0%)
Chinese:
7 (11,3%)
Hindu: 10
(16,1%)
Others: 1
(1,6%)
|
Primary: 1 (1,6%)
Secondary:
35 (56,5%)
Diploma: 12
(19,4%)
Degree: 11
(17,7%)
Masters/PhD: 3
(4,8%)
|
|
Hammud, A; Avitan-Hersh,
E;
Khamaysi, Z. 2023
[46].
|
164 |
Male: 96 (58,5%)
Fem:
68 (41,5%)
|
Jewish: 93 (57%)
Arab:
71 (43%)
|
|
|
Choi, E; Cook, A; Chandran,
N S.
2018 [47].
|
58 |
Male: 34 (58.6%)
Fem:
24 (41,4%)
|
Chinese: 24 (41,4%)
Malaysian:
7 (12,1%)
Hindu: 17
(29,3%)
Others: 10
(17,2%)
|
|
|
|
Yuksel, M; Basim, P. 2019
[48].
|
208 |
Male: 142 (68,3%)
Fem:
66 (31,75)
|
|
0 to 8 yo: 70 (33,7%)
8
to 16 yo: 138 (66,3%)
|
|
|
Alsadhan, H. et al. 2022
[49].
|
183 |
Male: 101
Fem: 82 |
|
|
|
|
Hayama, K. et al. 2020 [50].
|
300 |
Male: 219 (73%)
Fem: 81
(27%)
|
|
|
|
|
Chu, CB; et al. 2021 [12].
|
161 |
Male: 110 (68,3%)
Fem:
51 (31,7%)
|
Caucasian: 02 (1,24%)
Taiwanese:
159 (98,76%)
|
|
|
|
Vazquez, et al. 2013 [51].
|
268 |
Male: 79 (29,5%)
Fem:
189 (70,5%)
|
Caucasian: 241 (90,3%)
No
Caucasian: 26 (9,7%)
Unknown:
1
|
>12 yo: 139 (57.9%)
12
to 57 yo (23,8%)
<12
yo: 44 (18,3%)
Unknown:
28
|
|
Kamat, D; Gaba, S; Kumaran,
M S.
2021 [52].
|
22 |
Male: 10 (45,4%)
Fem:
12 (54,4%)
|
|
|
|
|
Schrader, A. M. R. et al.
2014 [53].
|
846 |
Male: 232 (27,4%)
Fem:
614 (72,6%)
|
|
|
|
|
Wang, Z S. et al 2022 [54].
|
87 |
Male: 67 (77,0%)
Fem:
20 (23,0%)
|
Chinese: 75 (86,2%)
Outros:
12 (13,8%)
|
|
|
|
Fabrocini, G. et al., 2016
[55].
|
27 |
Male: 8 (29.6%)
Fem: 19
(70.4%)
|
|
|
|
Table 3: Study, sample, main triggering/aggravating factors and HS severity.
| Estudo |
Amostra |
Smoking |
Obesity |
HS Severity |
|
Lorite-Fuentes, I. et al.
2022 [40].
|
221 |
Smokers: 127 (57,46%) |
BMI (Kg/m²) : 29,65 |
Hurley I: 65 (29,41%)
Hurley
II: 86 (38,91%)
Hurley
III: 70 (31,67)
|
|
Andrade, et al. 2015 [35].
|
123 |
Smokers: 75 (61%)
No-Smokers:
42 (34%)
Unknown: 6
(5%)
|
Yes: 55%
No: 12%
Unknown:
33%
|
Hurley I: 26 (21%)
Hurley
II: 59 (48%)
Hurley
III: 38 (31%)
|
|
Katoulis, et al. 2017 [41].
|
152 |
Smokers: 110 (72,4%)
Ex-Smokers:
11 (7,2%)
No-Smokers:
31 (20,4%)
|
BMI <20: 3
BMI
20-<25: 35
BMI
25-<30: 35
BMI
30-<35: 44
BMI
35-<40: 22
BMI ≥ 13
|
Hurley I: 40 (26,3%)
Hurley
II: 68 (44,7%)
Hurley
III: 44 (29,0%)
|
|
Kluger, N; Ranta, M;
Serlachius, M. 2017 [42].
|
26 |
Active Smokers: 10 (385%)
Ex-Smokers:
10 (38,5%)
No-Smokers:
6 (23,1%)
|
BMI < 25: 4 (15,4%)
BMI
> 30: 13 (50%)
|
Hurley I: 13 (50%);
Hurley
II: 11 42,3%)
Hurley
III: 2 (7,7%)
|
|
Delany, et al. 2017 [43].
|
150 |
Active Smokers: 84
(56,0%)
Ex-Smokers: 33
(22,0%)
No Smokers: 33
(22,0%
|
BMI ≥ 25 kg/m2: 81,8% |
Hurley II: 50,4% |
|
Schultheis, M. et al. 2023
[44].
|
553 |
Active Smokers: 353
(63,83%)
Ex-Smokers: 97
(17,54%)
No Smokers:
103 (18,62%)
|
BMI: 32,2 ±7,27 |
Hurley I: 72 (13,0%);
Hurley
II: 343 (62,0%);
Hurley
III: 138 (25,0%)
|
|
Loo, C H. et al. 2018 [45].
|
62 |
Yes (Smokers /
Ex-Smokers
): 29 (46,8%)
No (Never
Smoked): 33 (53,2%)
|
BMI ≥ 27,5: 30 (48,4%);
BMI
23 – 27.4: 15 (24,2%)
BMI
18,5-22,9: 9 (14,5%)
BMI
< 18.5: 8 (12,9%).
|
Hurley I: 15 (24,2%)
Hurley
II: 38 (61,3%)
Hurley
III: 9 (14,5%).
|
Hammud, A; Avitan-Hersh, E;
Khamaysi, Z. 2023
[46].
|
164 |
Smokers: 90 (55%) |
Overweights: 46 (28%). |
Hurley I: 33 (20,0%)
Hurley
II: 83 (51,0%)
Hurley
III: 48 (29,0%)
|
|
Choi, E; Cook, A R;
Chandran, N S. 2018 [47].
|
58 |
Yes: 19 (35) |
BMI < 25: 10 (38)
BMI
25-30: 9 (38)
BMI >
30: 19 (38)
|
Hurley I: 22 (37,9%)
Hurley
II: 30 (57,1%)
Hurley
III: 6 (10,3%).
|
|
Yüksel,M; Basim.2019 [48].
|
208 |
Smokers: 126 (60.6%)
No
Smokers: 82 (39,4%)
|
BMI < 18,5: 1 (0,5%)
BMI
18,5-25: 59 (28,4%)
BMI
25-29: 92 (44,2%)
BMI ≥
30: 56 (26,9%).
|
Hurley I: 67 (32,2%)
Hurley
II: 118 (56,7%)
Hurley
III: 23 (11,1%).
|
|
Alsadhan, H. et al. 2022
[49].
|
183 |
Smokers: 43 |
Overweights: 46
Obese:
48
Morbid Obesety: 63
|
Hurley I – Moderada:
98
Hurley
II e III – Grave:
85
|
|
Hayama, K; et al. 2020 [50].
|
300 |
No: 85 (28,3%);
Yes:
123 (41,0%)
Unknown: 92
(30,7%).
|
Yes: 48 (16,0%) |
Hurley I: 69 (23%)
Hurley
II: 109 (36,3%)
Hurley
III: 121 (40,3%)
Não
informado: 1.
|
|
Chu, CB. et al. 2021 [12]
|
161 |
Active Smokers: 54
(36,0%)
Ex-Smokers: 4
(2,7%)
No Smokers: 92
(61,3%)
Uninformed: 11
|
Normal weight: 51 (38,1%)
Over
weight: 42 (31,3%)
Obese:
41 (30,6%)
Uninformed:
27
|
Hurley I: 69 (42,9%)
Hurley
II: 68 (42,2%)
Hurley
III: 24 (14,9%).
|
|
Vazquez, et al. 2013 [51].
|
268 |
No Smokers: 79 (29,8%)
Active
Smokers: 153 (57,7%)
Ex-smokers:
33 (12,5%)
|
BMI < 25: 49 (19,2%)
BMI
25,0-29,9: 66 (25,9%)
BMI
30,0-34.9: 49 (19,2%)
BMI
35.0-39,9: 49 (19,2%)
BMI
40,0-49,9: 33 (12,9%)
|
Hurley I: 160 (59,7%);
Hurley
II: 102 (38,1%)
Hurley
III: 6 (2,2%)
|
|
Kamat, D; Gaba, S; Kumaran,
M. 2021 [52].
|
22 |
Active Smokers: 3 (13,6%)
|
BMI 19-25: 8 (36,3%)
BMI
25-29,9: 10 (45,4%)
BMI
≥ 30: 4 (18,1%)
|
Hurley I: 3 (13,6%)
Hurley
II: 7 (31,8%)
Hurley
III: 12 (54,4%0.
|
|
Schrader, A. M. R. et al.
2014 [53].
|
846 |
Active Smokers: 595
(70,7%)
Ex-Smokers: 119
(14,2%)
No Smokers: 127
(15,1%)
Uninformed: 5
|
BMI ≥30.0: 263 (32,3%)
BMI
> 25.0-29,9: 256 (31,5%)
|
Hurley I: 385 (45,5%)
Hurley
II: 351 (41,5%)
Hurley
III: 110 (13,0%)
|
| Wang, et al. 2022 [54]. |
87 |
Smokers: 30 (34,48%)
Ex-Smokers:
13 (14,94%)
No
Smorkers: 44 (50,6%)
|
BMI < 18,5: 3 (3,4%)
BMI
18,5-23,9: 31 (35,6%)
BMI
24,0-27,9: 24 (27,6%)
BMI
> 28: 29 (33,3%)
|
Hurley I: 22 (25,3%)
Hurley
II: 52 (59,8%)
Hurley
III: 13 (14,9%)
|
|
Fabbrocini, D. et al., 2016
[55].
|
27 |
Current Smoker: 14 (51.8%)
|
|
|
Discussion
Thus, given the scarcity of epidemiological data on HS, and
high heterogeneity among the studies retrieved, some studies
clearly pointed out the demographic aspects of the disease. Then,
subgroup analyzes were carried out as detailed below:
Gender and race or ethnicity were the most discussed data.
Individual or family income and education do not appear in the
protocols or in clinical trials, and there is a lack of establishing correlations between the factors causing or aggravating the disease
and the outcomes observed.
A total of 3,611 patients with hidradenitis suppurativa were
included in the 18 studies analyzed. The studies revealed demographic data for 1,476 (40.88%) men and 2,135 (59.12%) women.
Only 1,099 patients had data related to race, color or ethnicity
mentioned.
Data gaps allowed the following distribution: 505 were identified as white; 50 were identified as non-white, Afro-descendant
or black; 36 were classified as unknown or other; 344 were identified as Asian, Malayan, Chinese, Indian and Taiwanese, and 164
were mentioned as Arab and Jewish.
Regarding Education, of the 18 articles, only 5 studies dealt
with the subject, but the way the data were placed makes a more
precise analysis difficult. Only 4 articles dealt with the subject of
work/occupation, referring to 881 patients with HS, of whom 236
were clearly defined as unemployed.
Regarding smoking, all 18 articles make reference. 3,115
patients had their data clearly informed while 496 had, for unidentified reasons, their information neglected. Smokers and exsmokers totaled 2,358 patients, while non-smokers totaled 757.
Among the 17 articles that emphasize the issue of obesity, some
provided only average data.
The way the data was placed, considering the unknown and
uninformed, only 614 patients were clearly identified as having a
BMI>30 kg/m
. 17 articles used the Hurley Classification to assess
disease severity. Of these, 2 articles generated ambiguity in their
interpretation. 15 articles provided clearer information allowing
the following distribution: 1,061 patients were classified as Hurley
I; 1,525 with Hurley II, and 664 patients were referred with Hurley III.
Hidradenitis suppurativa and socioeconomic status
The Organic Health Law (Law 8,080/90) in force in Brazil provides for the conditions for the promotion, protection and recovery of health, the organization and operation of the corresponding services and other provisions. The law sets out the determining and conditioning factors for health as food, housing, basic
sanitation, the environment, work, income, education, transport,
leisure and access to essential goods and services for health.
The National Commission on Health Determinants establishes
social determinants as the social, economic, cultural, ethnic/racial, psychological and behavioral factors that influence the occurrence of health problems and their risk factors in the population;
while the World Health Organization (WHO), in relation to social
determinants of health, classifies them as conditions in which
people are born, grow, live, work and age, including the health
system.
Socioeconomic level (SES) refers to an individual’s social position in relation to other members of society [56]; plays a significant role in determining an individual’s quality of life, health,
social position, and class [57]; it is one of the main factors that
influence the health status of a nation [58]. NSE can be classified
into two types: objective NSE and subjective NSE. This can be assessed using methods such as the MacArthur Scale.
Objective SES refers to three different aspects, namely income,
education and occupation, while subjective SES refers to the perception that people have regarding their position in the social
hierarchy in relation to other individuals. The level of education
is one of the indicators of socioeconomic level. People with low
knowledge are more prone to poor health, have less understanding of their health problems and treatment, and are at greater risk
of hospital admissions [59].
The relationships between socioeconomic status and health,
social and financial inequalities are current issues. The socioeconomic link and health, whether individual or collective, has
already been widely debated. However, among the 18 scientific
works listed in this study, only three mention the profession,
employment relationship and/or income of patients affected by
Hidradenitis suppurativa. A descriptive epidemiological study
of HS involving 152 cases emphasizes occupation: thirteen patients (8.5%) worked in the public sector; 29(19.0%) were selfemployed, 35(36.2% worked in the private sector; 15(9.9%) were
housewives; 16(10.6% were students; 5(3.3%) were students; 4
(2.6% were retired; and 15(9.9%) were unemployed [41]. A review of medical records involving 26 patients emphasizes income,
limiting itself to mentioning that “58.3% had an annual income
between 25,000 and 59,999 euros” and that “in total, 16 patients
(61.5%) were unemployed” [42]; while a cross-sectional epidemiological study with 150 patients, showing that, of the 143 patients who filled out the questionnaires, 49.7% were employed at
the time of the survey; 21.3% were unemployed, while 9.4% were
unemployed due to temporary or permanent disability [43]. Both
studies, in their conclusions, did not establish a direct relationship
between socioeconomic status and HS.
Although controversial, socioeconomic level is a critical determinant of health outcomes. A study involving 27,614 patients
with HS observed that low socioeconomic status was found in
6,195 patients (22.4%).
HS was associated with lower socioeconomic status, in crude
analysis (Odds Ratio 85, 95 CI: 1%, 80.1-90.1). The association,
in multivariate analysis, proved to be more modest (Odds ratio
13.95; CI: 1%, 9.1-16), and concludes that the modest association
between SH and low socioeconomic status may not be a determining factor for the development of the disease [29]. In contrast,
a self-reported population-based cohort of 56,084 respondents
found a general prevalence for HS of 2.1% (CI: 95%, 2.0-2.2) and
highlights that patients with HS had a lower socioeconomic status lower than controls (P<0.001) [40]. Low socioeconomic status
may be a risk factor for the development of HS as it may be associated with an unhealthy lifestyle such as smoking and obesity,
factors that have been widely studied and related to the development and chronicity of the disease [61]; while differences in
socioeconomic status between racial groups constitute one of the
main factors contributing to racial disparities in health [62].
Cause or consequence of HS, low socioeconomic status may
be associated with worse results in physical and mental health,
and in people’s quality of life. Groups of low socioeconomic status
may, on the one hand, face increased levels of health impairment,
and on the other, face lower levels of health-related quality of life
[63].
A cross-sectional study based on a registry of 13,538 patients
diagnosed with HS showed a mean age of 44 years, more frequently in women, single people, lower education and lower income, and a high prevalence of overweight, obesity and smoking
in pregnant women [64].
Low socioeconomic level can translate into increased financial
expenses for patients who require routine medical consultations,
more expensive medications, hospitalizations, more intensive
post-operative care and/or higher costs with dressings and return
consultations for follow-up. Furthermore, the higher costs can
also be passed on to health plans, and to public health policies,
that is, States or nations, both through expenses resulting from
surgical claims or loss of life in the full working age range.
Another expression of socioeconomic level is elevations in
inflammatory factors. Cytokines such as TNF-α, IL-1B and IL-10,
among others, are involved in the pathogenesis of HS [65]. IL-6 is a cytokine with a molecular weight between 21 and 30 kDa, little
reported in studies related to HS, however the upregulation of
IL-6 appears to be involved in some inflammatory diseases such as
rheumatoid arthritis and Crohn’s disease [66]. On the other hand,
IL-6 appears to be related to socioeconomic status. Aging itself
may be related to an increase in inflammatory cytokines. Unfavorable social and economic conditions are associated with the
increase in these substances, and in particular, with the increase
in IL-6 [67]. Parents’ low level of education is associated with their
children’s state of inflammation during adolescence, a fact that is
partly explained by adiposity. Parental education is inversely associated with increased levels of IL-6 [68].
Social inequalities can translate into health inequalities. Socioeconomic level and inflammation levels (CRP and IL-6) are associated. Smoking and obesity as behavioral processes explain this
association. People with low socioeconomic status exhibit higher
levels of inflammatory markers, leading to the conclusion that
socioeconomic inequalities can be translated into inequalities in
physical and mental health [69]. In obesity (BMI>30 kg/m2
) an average increase in ESR, CRP and IL-6 levels can be observed [70]
while serum IL-6 levels are increased in patients with HS Hurley
II and III, which suggests that IL-6 may play a role in the development of HS [71] and that serum IL-6, CRP and ESR may be considered effective markers in assessing the severity of HS [72].
Hidradenitis suppurativa and gender
Does HS have a predilection for the female sex? Does sexual
gender determine which regions of the body are affected by the
disease? Epidemiological studies, the most diverse, attempt to
clarify the geographic distribution of HS between countries and
highlight the distribution of the disease between men and women. A controversial subject, the prevalence of HS varies greatly
between different geographic regions as well as between sexes.
In American and European populations, where epidemiological
studies are most carried out, evidence points to a higher prevalence in females, that is, for every three women, only one man
is affected by the disease [73]. The opposite can be observed in
East Asia, where HS was found to be more common in men and
few with a positive family history [74], more precisely in Korea,
where a predominance of male patients was observed reaching
a relationship male/female ratio of 2.5:1 [75] and in peninsular
Malaysia, where a male predominance was found among patients
with an earlier age of onset and more severe disease [45].
The onset time of the disease differs between men and women.
The prevalence is higher in the fourth and fifth decades of life, but
the onset of the disease can date back to puberty or the immediate post-puberty period. HS is rare in children and pre-pubertal
children, and when it occurs, it may be due to hormonal disorders
and genetic susceptibility [76] or unknown etiology [77].
Women have an earlier onset of the disease compared to men,
and are less likely to have the more severe form of the disease
[78], while men develop the disease later, but are more likely to
have the more severe form. compared to women [75]. Regarding
distribution, men develop lesions more frequently in the glutes,
perianal and atypical regions and a history of severe acne, while
women develop predominantly inguinal and breast lesions and a
more frequent family history of HS [53]. The severity of the disease appears to be associated with male sex, duration of the disease, obesity and smoking [53]. The two environmental factors
most involved in the development of HS are also factors implicated in the severity and possibly in the distribution of the disease
between the sexes. Obesity and smoking appear to be associated
with more severe disease [75].
HS has a negative impact on the exercise of sexuality in both
men and women. In a systematic review, the prevalence of sexual
dysfunction varied between 51 and 62% and, considering erectile dysfunction, a specific type of sexual dysfunction that impairs
penile erection, the prevalence varied between 52 and 60%, in
a universe of 42,729 patients with HS, with women being most
affected by sexual suffering [79]. HS affects the sexuality of both
patients and their sexual partners.
A cross-sectional study including 34 single patients and 28
patients in stable relationships and their partners showed that
women with Hidradenitis suppurativa had a high prevalence of
sexual dysfunction (13/32, 40.6%) while men had a high prevalence of erectile dysfunction (19/30, 63.3%). Male partners had a
high prevalence of erectile dysfunction (10/17, 58.8%) while only
one female partner had sexual dysfunction (1/11, 9.1%) [80]. Multicenter study involving 13 European countries, 23.1% of 3,485
patients with various skin conditions reported sexual problems.
Impairment was higher in patients with HS, prurigo, bullous diseases, psoriasis, urticaria, eczema, skin infections or pruritus, and
sexual impact was more widely related to depression, anxiety and
suicidal ideation [81]. Therefore, HS is strongly associated with
sexual problems such as sexual dysfunction in women and erectile
dysfunction in men [82].
Hidradenitis suppurativa and ethnicity
Epidemiological studies related to HS generally originate in
developed, Western, predominantly white/Caucasian countries.
Demographic information, such as education and occupation, is
scarce, and epidemiological data from developing and underdeveloped countries are very limited.
There is racial and ethnic underrepresentation in research and
clinical trials. 246 clinical trials were analyzed. 215(87.4%) reported racial data. Hispanics and Latinos were underrepresented,
and Black/African Americans were underrepresented even when
accounting for prevalence rates [83]. Patients from ethnic-racial
minorities with chronic inflammatory skin diseases, more precisely black and Hispanic people, are disproportionately affected by
numerous obstacles to care [84]. As previously stated, social determinants have important influences on health and favor health
disparities in different ways. Health disparities are understood as
differences in the incidence, prevalence, severity and number of
diseases experienced by less privileged populations [85].
Considering the influence of race on HS, African Americans
face significant disparities in disease severity, emergency room
visits, hospitalizations, and surgeries [86]. Mean HS prevalence
rates were highest among African-American populations (1.3%),
lowest among Hispanic/Latinos (0.07%), and intermediate among
Caucasian populations (0.75%) [87].
There is a paucity of data exploring the distribution of race
and ethnicity in randomized controlled clinical trials for HS [88].
African Americans had a prevalence up to 3.1 times higher than
whites/Caucasians [89].
Evidence demonstrates a higher prevalence of HS in darkskinned patients, a higher prevalence of comorbidities, greater
severity, and greater difficulties in accessing effective medical
care [90]. Considering health disparities, a targeted review focusing on race and ethnicity concluded that for black/African Americans, 29 of 38 health disorders revealed a considerable excess in
incidence, prevalence or severity. After sickle cell anemia, multiple myeloma and hidradenitis suppurativa showed the highest
excesses in frequency [91].
The cytokines TNF-α, IL-22, IL-23, IL-17, IL-27 and IL-10, in subgroup analysis by race, showed higher concentrations in AfricanAmerican patients [92]. A greater delay in diagnosis is observed
in non-white patients. Another fact to be observed among these
patients is the fact that medical consultations are more frequent
with surgeons than with dermatologists [93]. Black patients with
HS may use health services more frequently and have a greater
severity of the disease [94].
African Americans are more likely to have clinical visits for HS
than whites [95]. Differences were observed in the medical care
and procedures provided to black patients when compared to
white patients.
Blacks received more Metformin and nonsteroidal anti-inflammatory drugs during HS-associated visits and were more likely
to undergo complex surgical excision [96]. A greater number of
hospitalizations due to HS was observed in black patients [97]. A
retrospective cohort study recorded a total of 3,079,332 hospital
admissions of patients with Inflammatory Bowel Disease (IBD), including 4,369 patients with concomitant HS. IBD-HS patients were
significantly younger, mostly African American women, more
prone to smoking, obesity, diabetes mellitus, depression, and
anemia [98]. Obesity and metabolic syndrome are predisposing
and/or aggravating factors for HS. They are also a problem commonly faced by African-Americans, which may partly explain the
higher prevalence of HS in this racial group.
When talking about race and HS, it is known that there is an
extensive gap of ethnic and racial heterogeneity in epidemiological research data, just as it is common knowledge that racism is
a reality in our environment and an important determining factor
of health. Racism, whether structural, cultural, institutional or individual, affects health through different paths. Systematic review
of empirical research on racism and health showed an association
between self-reported racism and health problems in oppressed
racial groups with negative results in the areas of mental health
and health-related behaviors [99].
The analysis of 62 empirical articles, focusing on racial discrimination and health among Asian-Americans, showed that racial
discrimination was related to worse health status, more precisely
to mental health [100]. In a systematic review involving 121 studies in which African-American, Latino and Asian populations were
most frequently included, strongly significant associations were
found between racial discrimination and mental health (depression and anxiety) [101]. Perceived discrimination can be translated into significant stress responses and/or unhealthy behaviors
or even the absence of participation in healthy behaviors [102].
Internalized racism (in which people internalize racist attitudes, beliefs, stereotypes, ideologies about an ethnic-racial group or someone) is negatively associated with health through
decreases in self-evaluation of the positive core, increases the relationship between stressors and health problems, mediates between discrimination and health, or can be a protective strategy
against health problems [103]. Racism proves to be an extremely
stressful factor in the lives of the less privileged, bringing with it
negative consequences for physical and mental health. Intergroup
and intragroup racism play a role in morbidity and mortality rates
in African American populations [104]. Stress, by stimulating the
hypothalamic-pituitary-adrenal axis, stimulates the production of
cortisol and consequently changes in the immune system.
It is known that dysregulation of the immune system is one of
the elements involved in the onset and chronicity of hidradenitis
suppurativa.
A dearth of research addressing disparities and the role of
social determinants of health remains a constant even as data
suggests that people of color have a higher risk of developing HS
compared to white people.
Hidradenitis suppurativa and education
Epidemiological studies that establish a relationship between
HS and education are practically non-existent. A population-based
study, seeking to determine the incidence of HS and associated
factors, observed that 18.3% (44 of 268 patients with HS) had less
than 12 years of education, and 28 patients had their education
level declared as unknown, possibly due to are not included in the
analyzed census data [51]. Another cross-sectional study, involving 26 patients, shows that only 57.5% of them had secondary or
higher education, leading to the conclusion that 42.5% had only
primary education [42]. A cross-sectional, multicenter study with
62 patients describes that 36 (58.1%) of them had only completed
primary and secondary education [45]. While another, when evaluating the clinical and demographic characteristics of HS cases,
highlights that 70(33.7%) of the 208 patients listed in the work,
had only 0 to 8 years of school studies [48].
When characterizing the heterogeneity of comorbidities
among 13,667 HS patients, another study highlights that the highest level of education achieved by 83% (11,338) of these patients
was less than a bachelor’s degree [105] and more, in a cross-sectional study involving 1,301 individuals, 206 were officially diagnosed with HS, among which, 23 patients with severe HS and 24
patients with mild HS, had only primary and/or secondary education [106].
It is known that the level of education is related to socioeconomic position. This, in turn, is an indicator of physical and mental health in modern societies. Low education can translate into
lower positions in socioeconomic hierarchies, and can be related
to situations of inferiority, generating physical and mental consequences directly related to health status, in addition to deprivation of material goods [107]. Furthermore, when it comes to
HS, the level of education can be observed from two aspects: on
the one hand, people with greater knowledge may have an earlier
perception of the disease and thus seek medical services earlier,
and in a more efficient way it is clearer to adopt care and treatment measures for HS; which may, on the other hand, not occur
with people with a lower level of education.
The functional incapacity, taboo, stigma, low self-esteem and social isolation generated by the disease can be better managed,
avoiding greater negative impacts on their academic activities
and/or individual work. It should be noted that in a cross-sectional
study involving 206 patients with HS, only 17 patients had a master’s/doctorate degree, and that, in this context, only 6 of them
had progressed to the severe form of the disease, while 11 had
mild HS [106] leading to the conclusion that the level of education
can directly influence the diagnosis, treatment and control of HS.
An early diagnosis interferes with the progression of the disease.
Hidradenitis suppurativa and work/occupation
Hidradenitis suppurativa is a chronic disease that directly affects the patient’s quality of life in all its aspects. Patients with
HS often suffer from anxiety disorders, depression, social isolation, sexual dysfunctions and difficulties in performing their work
functions. The severity of the disease, the number of decompensations, the locations and the number of skin areas affected are
factors that influence the patient’s well-being. Stigma, common
among HS patients, exerts a strong psychosocial influence. Pain,
itching, bad odor, disfiguring scars as well as the public’s lack of
knowledge about HS contribute to stigmatization [108]. Chronic
pain, whether mild or moderate, and quality of life are factors associated with loss of productivity at work [109].
HS is a disease that has a major impact on the patient’s professional life. A substantial loss of work capacity and productivity is
observed. HS is a debilitating disease that affects individuals of
working age [110]. The severity of the disease, depressed mood
and intense pain cause a decrease in work capacity and productivity [111]. Presenteeism, reduced overall productivity at work and
impaired activity correlate positively with greater disease severity
and low quality of life [112]. Newly diagnosed patients with HS
had significantly slower income growth and greater risk of leaving
work compared to controls, while patients with HS, in general,
had more total days lost from work, higher total annual indirect
costs, and lower annual income when compared to controls [113].
Hidradenitis suppurativa negatively impacts productivity as well
as professional career progression. Other facts already known on
the subject are that patients with HS have high rates of unemployment, low annual income, decreased ability to work and losses
in work productivity. This compromise in production leads to indirect socioeconomic costs caused by lower employability rates,
absenteeism and decreased productivity [111].
In addition to the losses related to the reduction of the workforce, another negative aspect of HS can be observed in the high
costs and/or expenses for patients with the disease. The use of
healthcare resources associated with the management of patients
with HS is high. The average annual cost of HS was €6,791 per patient. Loss of productivity, biological treatment and informal care
accounted for 53.3%, 21.5% and 9.2% respectively. There were 26
days of absence from work due to absenteeism and 63 days due
to presenteeism. Male gender, more severe HS, gluteal involvement and associated inflammatory bowel disease accounted for
higher direct medical costs while lower education and worse quality of life accounted for higher indirect costs [114].
Regarding expenses related to HS, considering limited and
non-homogeneous data, the average total cost caused by the disease per patient/year ranged from $258 to $8,078. Increase was
observed in case of surgical intervention, disease progression, failure of antibiotic efficacy and comorbidities. Higher costs were
noted for hospital care, followed by outpatient care and emergency services [115]. Regarding the use of emergency services
and hospitalizations, patients with HS made more use of these
resources when compared to patients with Psoriasis [116], and
in the HS-IBD association, they were more likely to develop sepsis, greater length of stay and higher total hospital costs [98]. HS
is associated with large costs related to hospital care for young
patients, of full working age, and high costs of National Health
Service resources [117].
Hidradenitis suppurativa and smoking
Smoking is one of the main preventable risks to general health.
It is a condition, in itself, very important for the development of
many health problems with the most varied outcomes and dimensions, and when enhanced by conditions such as obesity and
depression, there is a greater risk of illness. Tobacco use can affect all organs and systems in the human body. Tobacco and its
constituents affect the skin through external and internal exposure, which can be evidenced by a list of skin and mucous signs
resulting from its use as well as the increased incidence and/or
exacerbation of numerous skin diseases [118]. Skin aging, contact
dermatitis, psoriasis, hair and hair follicle diseases are on this list,
and some of them may characterize a dose-dependent pattern.
Smoking, even light and intermittent smoking, brings substantial
health risks, lower health-related quality of life compared to nonsmokers, and a variable list of signs and symptoms [119].
Tobacco smoking has substantial local and systemic adverse effects on the immune system, respiratory system, skin, and soft
tissues [120].
The systemic effect of chronic smoking (>40 cigarettes/day; >5
years) on the cutaneous elastic fiber system can account for wrinkling and loss of skin elasticity, that is, chronic smoking significantly increases the hardening of the dermis and of the epidermis due
to the significant remodeling of the elastic fiber network [121].
Several studies associate smoking with Hidradenitis suppurativa.
Up to 98% of HS patients are active smokers, and these tend to
have higher scores and, consequently, greater severity of the disease [122]. There is a much higher prevalence of smoking, up to
90%, among patients with HS [123]. Current (active) smoking favors a greater number of body areas affected by HS compared
to patients with HS who are non-smokers or who have stopped
smoking [124].
Smoking may also be related to the risk of injury due to pressure. Active (current) smokers and ex-smokers have approximately 1.5 times greater risk of developing lions resulting from pressure compared to non-smokers [125].
Regarding socioeconomic status, patients with Hidradenitis
suppurativa are more likely to have a low social and economic status compared to patients without HS [29]. Regarding educational
level, poor health perception and early initiation of smoking in
groups with less education were the main predictors of educational differences in smoking maintenance [126].
The prevalence of smoking is higher among less favored
groups, and less favored smokers may face greater exposure to
the harm caused by cigarettes, that is, among individuals with low
socioeconomic status, acceptance of smoking is greater and attempts to quit smoking have increased. greater probability of failure [127]. Regarding social and economic disparities in intentions
to quit, attempts to quit smoking and abstinence, it is observed
that smokers with lower education or income are less likely to report the intention to quit smoking compared to those with higher
education or income [128]. In Brazil, considering socioeconomic
inequalities, there is a higher prevalence of current (active) smoking among those with less education, in the non-white population
and among those who did not have health insurance, and an unhealthy behavior score was higher in the extracts of lower education, in the non-white population, among those who did not have
health insurance, and higher smoking rates among males [129].
Relating socioeconomic level, smoking cessation services and
smoking cessation behavior in Brazil, it is highlighted that smokers with a higher socioeconomic level visit a medical service 1.54
times more often than those with a lower socioeconomic level,
and had 1.65 more opportunities to receive guidance on quitting
smoking [130].
The social and economic characteristics of the areas in which
they live seem to influence the behavior of smokers in attempts
to quit smoking. It is possible that there is a relationship between
the deprivation of the place where one lives and the smoker’s status. Some attributes of living in a deprived area can contribute to
worse smoking profiles and a lower prevalence of smoking cessation [131].
Smoking is shown to be one of the main contributing factors to
socioeconomic disparities in health. The opposite can also be observed. In a succinct analysis, considering the gaps in knowledge,
factors involved in the development of HS such as smoking, obesity, depression and socioeconomic status seem interconnected.
Cross-sectional study involving 212 patients diagnosed with HS
between 1981 and 2001, analyzed after a 22-year segment (range
12-32) demonstrates that smoking and obesity were significantly
associated with a lower self-reported remission rate of Hidradenitis suppurativa [132], while advanced age and non-active (current) smoking were important factors associated with a positive
response when starting HS treatment with first-line measures
such as topical and oral antibiotics, intralesional corticosteroids
and antiseptics [133].
The mechanism by which smoking triggers Hidradenitis suppurativa is unclear. It is known that nicotine appears to influence
genetic predisposition, favoring the formation of follicular plugs
through an inflammatory process mediated by neutrophils [34].
Nicotine stimulates the sweat gland, favoring the engorgement of
the glandular ducts [134], modifying their activity as they begin to
produce pro-inflammatory cytokines such as Interleukin (IL)-8 and
TNF-α [124] and consequent inflammatory reaction. Nicotine also
negatively influences by suppressing the notch signaling pathway,
and thus, mechanisms such as intercellular communication, regulation and cell differentiation, which allows the emergence of inflammatory diseases such as HS [124]. Smoking interferes with
innate and adaptive immunity and plays dual roles in regulating
immunity, exacerbating pathogenic immune responses or attenuating defensive immunity, and thereby exerting effects on chronic
inflammation and autoimmunity [135].
Hidradenitis suppurativa and obesity
Obesity has been characterized as a global public health problem in recent decades. It has been showing an increasing prevalence in the last two decades [136], substantially among children
and adolescents in both developed and developing countries,
even taking into account a slowdown in the increase in obesity in
so-called first world countries [137].
This prevalence has increased globally in the last 40 years,
from less than 1% to 6-8% among children of both sexes, from 3
to 11% among men, and from 6 to 15% among women considering the time elapsed between 1975 and 2016 [138].
Obesity, also recognized for its association with a wide variety
of skin and systemic diseases as well as for its association with
psychiatric illnesses such as anxiety and depression [139], constitutes a broad threat to national or global public health considering the incidence, prevalence and economic burden it entails
[140]. Excessive healthcare spending, loss of productivity, loss of
economic growth resulting from reduced number of days worked,
lower productivity, higher mortality and permanent disability
must be considered [140]. Approximately 60-70% of individuals
who suffer from obesity can exhibit a variety of skin changes. Such
changes have been related to mechanical friction, infections and
hypertrophic conditions of the skin [141] and it should be noted
that obesity is a disease and a risk factor for the occurrence of
several other diseases, whether as a causal factor or as an aggravating factor [142]. Changes in skin barrier function, sebaceous
glands and sebum production, sweat glands, lymphatic system,
collagen structure and function, wound healing, as well as changes in microcirculation and macrocirculation and subcutaneous fat
can be observed in obesity [139].
As a result of an increase in adipokines, chemokines and cytokines, obesity is characterized by metabolic changes with subsequent accumulation of adipose tissue and an inflammatory
state, thus affecting skin homeostasis and activating immune cells
and consequently favoring chronic inflammatory diseases [143].
Genetic and environmental factors are widely implicated in the
origin of obesity. The types of food ingested, the socioeconomic
level added to behavioral factors such as sedentary lifestyle are
important environmental factors, while leptin, a hormone produced by adipocytes, and Pro-Opiomelanocortin (POMC) are the
genetic factors most involved in obesity [139]. Leptin’s function is
to carry information about the body’s fat reserves to the neurons
of the hypothalamic arcuate nucleus. These, in turn, stimulate the
POMC gene, which responds with the production of the prohormone pro-opiomelanocortin, involved in energy homeostasis. It is
known that changes in the POMC gene, generally caused by Single
Nucleotide Polymorphisms (SNPs), cause changes in the signaling
pathway and thus, causing a negative impact on the regulation
of energy expenditure and food intake, that is, favoring energy
consumption excess, hypertrophy and inflammation of adipose
tissue.
Obesity favors an increase in the intertriginous surface area
of the skin, skin-to-skin friction, increased sweat production and
retention and consequently skin maceration, as well as hormonal changes expressed by the relative excess of androgens [144].
Excess androgens contribute to thickening of the hair shaft and
consequently to follicular obstruction. Thus, obesity acts on the genesis and chronicity of HS either through mechanical factors
such as friction and/or through hormonal influences as observed
in Polycystic Ovary Syndrome and Insulin Resistance [34].
In the association between obesity and socioeconomic status,
it is stated that socioeconomic status is a determining factor in
the prevalence of obesity. In developed societies, socioeconomic
level is largely related to the prevalence of obesity: the lower the
social class, the greater the obesity, while in developing societies,
the higher the socioeconomic level, the greater the obesity [145].
Both obesity and socioeconomic status are negatively associated
in high-income countries, and positively associated in middle- and
low-income countries. Factors such as the introduction of solid
foods and family behaviors may explain the link between socioeconomic status and obesity. Parental education and early pediatric nutrition appear to explain the relationship between socioeconomic status and obesity [146].
The highest rates of obesity occur among population groups
with higher rates of poverty and lower education.
The link between poverty and obesity may be a consequence
of the low cost of high-calorie foods and the high palatability of
foods rich in sugar or fat [147]. Educational level, higher financial earnings and consumption of certain food groups can reduce
the risk of obesity [148]. A high level of education can promote
knowledge about the benefits of physical activity and the consumption of balanced meals and their impact on the quality of
health. A higher income favors greater access to resources for
better health, such as purchasing healthier foods, more time for
leisure and sports, as well as greater access to health services
[148]. Lower education level and income, lower property values
in the region of residence, and shopping at low-cost stores were
consistently associated with a higher risk of obesity, while higher
socioeconomic status, living in wealthier neighborhoods, shopping in Higher-cost stores have been linked to a protective effect
on obesity risk [149].
Other elements, within the spectrum of socioeconomic level,
that influence obesity are sex and age. Increasing age increases
the risk of obesity.
Weight gain is expected in men and women until the age group
of 50-60 years. But after the age of 50, women have a higher prevalence of obesity when compared to men [148].
The epidemiological relationships between SH and obesity
are evident. Cross-sectional study included 396 participants (339
women and 57 men), of whom 241(60.9%) were overweight or
obese, and 227(57.3%) were active smokers. The majority of patients had Hurley stages II (263, 66.4%) and III (76, 20.3%) HS, and
the increase in HS stage was related to obesity and some disease
locations such as genitals, pubis, gluteal fold and inguinal regions
[150]. Retrospective cohort included 102 patients (38 women
and 64 men). 68.4% had BMI≥25; 76.5% were active smokers;
and Hurley stages II and III were found in 53.1 and 33.3% of patients respectively [151]. And a retrospective review of medical
records including 149 patients (113 women and 36 men) showed
that 80.9% of them were overweight or obese, 39.5% were active
smokers or ex-smokers and Hurley stages II and III were diagnosed
in 36.5 and 33.9% of cases [152].
Hidradenitis suppurativa and chronic inflammatory diseases
HS is defined as a chronic inflammatory disease, often associated with other inflammatory diseases or factors that cause and/
or chronify inflammation. Smoking is an important triggering factor for HS [153]. Cigarette smoke, with its most varied chemical
substances, activates pro-inflammatory cytokines found in tissues
damaged by HS, activates nicotinic Acetylcholine (nAChRs) and
Aryl Hydrocarbon (AHRS) receptors and suppresses the Notch signaling pathway [124].
An increase in TNF-α, IL-1, IL-6, IL-8, GM-CSF is observed; a reduction in the levels of anti-inflammatory cytokines such as IL-10;
an increase in IgE levels; an activation of the activity of macrophages and dendritic cells; and an increase in the production of
antibodies such as citrulated proteins observed in Rheumatoid
Arthritis, and increased anti-dsDNA titers in Systemic Lupus Erythematosus [154]. Smoking tobacco causes systemic immunomodulatory effects as it releases reactive oxygen species from
the smoke responsible for a chain of harmful effects on normal
inflammatory function, reducing phagocytosis and bactericidal
activities, and increasing the release of proteolytic enzymes, thus
interfering with the process of renewal of connective tissue and
promoting its degradation [123].
Exposure to air pollutants is associated with damage to various organs of the body and a variety of skin diseases. The inflammatory state is a common feature in many skin diseases [155]. A
cytosolic multiprotein complex, the inflammasome, promotes the
maturation of pro-inflammatory cytokines IL-B and IL-18, reinforcing pollution-induced skin damage, and damaging the skin barrier appears to facilitate an increase in the production of reactive
oxygen species, promoting oxidative stress and activate the Aryl
Hydrocarbon Receptor (AhR) and inflammatory cytokines [156].
An increasing number of comorbidities are observed in patients with Hidradenitis suppurativa. Rheumatoid Arthritis (RA),
collagen vascular diseases, Psoriasis, Pyoderma gangrenosum and
Crohn’s Disease (CD) are some of the inflammatory conditions listed [157]. The association between HS and Crohn’s disease is well
known. In a cross-sectional analysis of 51,340 patients with HS,
the prevalence of Crohn’s disease was 2.0% (1025/51,340) compared with 0.6% (113,360/18,404,260) among those without HS.
(P<001). The prevalence was higher among white patients (2.3%),
aged between 45 and 64 years (2.4%), non-obese (2.8%) and
smokers (2.3%) [158]. An increased prevalence and risk of Crohn’s
disease and ulcerative colitis was observed in patients with Hidradenitis suppurativa, possibly due to the sharing of a common
immunopathogenesis in CD and HS [159]. Patients with a history
of inflammatory bowel diseases have a nine times greater risk of
developing HS than the general population [160].
Evidence suggests that common inflammatory pathways, such
as IL-1 and TNF-α, may be dysregulated in both HS and Spondylitis. The prevalence of inflammatory arthritis appears to be increased in patients with HS, especially in severe cases [161].
Psoriasis as a comorbidity of HS has been discussed, but the
association between the two diseases is not yet entirely clear.
Psoriasis and HS appear to result from the existence of a common inflammatory pathway manifested by increased expression
of IL-12/23 and TNF-α [162]. Positively regulated cytokines such as TNF-α, Interferon-γ, IL-1α/B, IL-6, IL-8 and IL-17 can cause an
inflammatory process in both diseases, and HS-Psoriasis coexistence can favor a greater prevalence of concomitant psychiatric
and cardiovascular diseases [163,164] and greatly increase the
severity of the disease, requiring more aggressive treatment
[165]. Analysis of health insurance data from about 7 million individuals concluded that the prevalence and incidence of HS were
68/100,000 and 10.1/100,000 respectively, and about 6% of patients with HS had Psoriasis as a concomitant disease [164]. A
study involving 68,836 patients with psoriasis and 68,836 control
cases showed that the prevalence of HS was higher in patients
with psoriasis compared to controls. Patients with concomitant
psoriasis and HS were, for the most part, younger, with a higher
prevalence of obesity and smoking when compared to patients
with psoriasis alone [166].
The association between HS and Arthritis is rare and most frequently affects peripheral joints [167]. Despite the low risk of the
association, when compared to patients without HS, patients with
HS have an increased risk of developing rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis [168].
The epidemiological association between HS and Rheumatoid
Arthritis does not seem to be firmly established despite the observation of the existence of common points in the interaction of
T and B cells and in the activation of pro-inflammatory cytokines
in both diseases, such as TNF-α, IL-6 and IL -1 [169]. Although the
exact underlying mechanisms of this association remain unclear,
patients with Hidradenitis suppurativa have a three-fold increased
risk of developing inflammatory arthritis, whether ankylosing
spondylitis or rheumatoid arthritis [170].
Hidradenitis suppurativa and mental health (Psychiatric Diseases)
Socioeconomic level (SES) or social class is an important factor in determining psychological outcomes [171]. Having a low
socioeconomic status in childhood appears to contribute to the
development of depression in adulthood. Low SES in childhood
may influence depressive symptom burden in midlife through a
combination of economic stress, restricted social resources, and
physical symptoms seen in adulthood [172]. The consequences of
financial difficulties accumulated over time constitute risk factors
for physical and mental health evident in youth and continuing
into adulthood and senility through chronic diseases such as depression, obesity and diabetes mellitus [173].
In developed countries, the prevalence and impact of depressive disorders are associated with certain characteristics, including socioeconomic level. Adopting health measures is effective in
reducing depressive disorders in low-SES populations in the short
and long term [174].
But when compared to higher SES, low SES was associated with
less promising outcomes in depression treatments. Cognitive Behavioral Therapy, interpersonal psychotherapy and pharmacotherapy demonstrated lower rates of improvement in patients
with low SES compared to patients of medium SES treated under
the same conditions [175].
Low socioeconomic status and negative complications are
risk factors for prenatal anxiety and depression, preterm birth
and birth weight. Low SES increases the adverse impact of previous negative events on anxiety and depressive symptoms during
pregnancy, and measures against anxiety and depression during
pregnancy should be targeted with greater particularity towards
unemployed pregnant women, with less education and low income [176].
Lower education and lower family income have an important
impact on psychiatric status, favoring a worsening in sleep quality.
The mental health of individuals with low socioeconomic status
is important in maintaining physical health. Low socioeconomic
status implies more vulnerable mental health and, consequently, more harmful effects on sleep quality. Less education can be
translated into fewer economic and social resources, favoring
stressful life experiences and culminating in anxiety and depression. Insomnia is perceived as a comorbidity of depression, and
individuals who suffer from insomnia have elevated levels of psychiatric distress or somatic anxiety [177].
Low socioeconomic status and mental illness (depression and
anxiety) have a bidirectional cause and effect relationship. Psychiatric illnesses can reduce employment and consequently income,
while psychological interventions can generate economic gains.
Negative economic patterns favor mental illness, but combating
poverty improves mental health [178].
Parents’ education and family income are important factors in
children’s lives. Children from highly educated and high-income
families are exposed to a lower level of childhood trauma [179],
while children from lower-SES families may meet more criteria for
mental disorder when compared to children from high-SES families [180]. Adverse childhood experiences may be associated with
lower education, and greater risks of depression, smoking and
drug use [181].
SES can determine people’s behavior and lifestyle. Individuals of low socioeconomic status are more likely to choose health
risk behaviors or ignore health prevention behaviors [182]. Social
conditions subsequent to low education seem to increase the
risk of prevalence of disorders among non-Latino whites and of
persistent mood and substance use disorders among ethnic-racial
minorities [183].
And morbidity resulting from chronic diseases and early mortality are more evident in individuals of low SES when compared
to people of higher SES [184].
The effect of SES and/or social inequalities on public health is
evident, whether physical or mental health. SES is associated with
a significant impact of diseases in the general population [185].
Defined as education level, income level or even neighborhood
level, SES may reflect the incapacity for work commonly observed
in chronic diseases such as Hidradenitis suppurativa. Inability to
work, however, can translate into limited income and resources,
and therefore into deprivation, regardless of the level of education.
HS is a polysymptomatic inflammatory condition with a negative effect on the physical, social and emotional well-being of patients [186]. The recurrent and debilitating aspect of the disease
negatively influences their physical and psychological aspects as
well as their quality of life. The involvement of anogenital regions
seems to be more related to compromised quality of life, while the involvement of exposed areas of the skin by HS seems to be
more related to stigmatization [187]. The bad smell causes significant damage to the quality of life in patients with HS [188]. Fear of
stigmatization favors social isolation. The bad smell, scars, itching
and pain encourage shame and irritability [189].
HS is always referred to as chronic painful follicular disease.
Chronic pain, of varying intensity, is the most bothersome symptom of HS. Pain, whether chronic or acute, possibly the most
impactful symptom of the disease, is associated with physical
limitations such as reduced mobility and sleep, and psychological changes such as irritability, depression, loss of control and the
ability to communicate painful experiences, as well as such as
changes in social relationships such as social isolation, intimacy
problems and compromising social responsibilities [190]. Pain,
itching, bad odor, stigmatization, and sleep disorders have an
important effect on the quality of life and mental health status
of people with HS [191]. Physical pain and feelings of shame are
strongly associated with psychological distress in HS and a feeling of powerlessness over one’s own body [192]. Cross-sectional
study involving 1,795 patients, in which pain was assessed using
a numerical scale, 83.6% of patients reported the presence of
pain. 77.6% of patients reported mild pain. Women and smokers reported more intense pain, and pain intensity was greater
in those patients with multiple areas of skin affected by HS [193].
The vicious circle characteristic of HS is identified as the factor responsible for pain, purulence, tissue destruction and scars [194].
Pain in HS is a mixture of acute pain (nociceptive) and chronic
pain (neuropathic) possibly resulting from inflammation of the affected tissues (injured areas) and damage caused directly to the
nerves, and the perception of pain can be associated with depression, anxiety and disease severity [195].
HS, like other inflammatory dermatoses, is associated with
mental comorbidities, mainly Depression and Anxiety. Metaanalysis involving 28 studies related to Depression and HS, and 12
studies related to Anxiety, showed a prevalence of 21% (95% CI
[17-25] in relation to Depression, and 12% (95% CI [6-17] in relation to Anxiety in patients with HS with wide variations in both
cases, demonstrating that patients with HS have a high impact of
Depression and Anxiety [196]. In a prospective study with 51 patients with HS, 29.4% presented mental symptoms, mainly symptoms of depressive disorder. HS patients were predominantly
young, female, with a history of high incidence of nicotine and
alcohol use, a positive family history of paternal alcohol dependence, and with more serious psychosocial impairments such as
less education [197]. In a cross-sectional study involving 1,795
patients, pain was reported in 83.6% of cases. 77.6% of cases
reported mild pain; women and smokers reported more intense
pain; pain was more severe in patients with multiple affected areas, and worse in those patients with the most severe form of
the disease [198]. Chronic pain is associated with a significantly
higher prevalence of Depression (20.2%) when compared to the
general population (9.3%) [199].
Psychiatric disorders are more observed in patients with immune-mediated chronic inflammatory diseases when compared
to the general population [200]. Systematic review and metaanalysis including 40,307 patients with HS, showed an overall
prevalence of Depression of 16.9% (95% CI: 9.9%-27.2%), and a
prevalence of Anxiety of 4.9% (95% CI: 1.7%-13.2%) [201]. It is estimated that one in four adults with HS has depression, and one
in five has anxiety [202]. A higher proportion of bipolar disorders
was found in patients with HS, and a tenfold increase in the prevalence of Schizophrenia [203].
In a cross-sectional study with 114 patients with HS, symptoms
suggestive of Depression were found in 47 of them (41.2%), with
no significant difference in the incidence of Depression in female
and male distribution, and without correlation between the incidence and severity of Depression and Anxiety about the severity
of the disease [204]. Cross-sectional analysis of 38,140 adult patients and 1,162 pediatric patients with HS, showed a prevalence
of depression among adults with HS equivalent to 30.0% (95% CI
[29.6-30.5] compared to 16.9% (CI: 95, 16.7-17.1) among the controls. Among children and adolescents with HS, the prevalence
of depression was equivalent to 11.7% (95% CI: 10.0-13.7) compared with 4.1% (95% CI: 3.6-4.7) among controls [205].
Mental illnesses or comorbidities negatively affect clinical illnesses while stimulating other psychiatric illnesses, consequently
worsening patients’ quality of life. The interactions between the
body and mind are relevant. Many skin diseases have a psychosomatic aspect. Evidence suggests the existence of biological
mechanisms underlying a bidirectional link between mood disorders and many clinical illnesses [206]. The nervous system and the
skin derive from the ectoderm and remain intertwined throughout life. Neural receptors in the skin may constitute the largest
sense organ in the body [207]. Tissues of the same embryonic
origin, once stimulated, react in a similar way. Skin and brain are
in permanent interaction through psychoneuroimmunoendocrine
mechanisms and behaviors [207]. Skin deficiencies and disorders
are often an early sign of a psychiatric disorder [208].
Psychiatric and dermatological disorders therefore have a complex relationship. Psychosomatic disorders summarize dermatological diseases stimulated or aggravated by emotional stress,
while secondary psychiatric disorders can be a consequence of
certain disfiguring skin diseases with subsequent psychological
suffering. Primary psychiatric disorders induce the appearance of
certain skin changes such as trichotillomania, factitious dermatitis,
neurotic excoriations, parasitic disorders and dysmorphophobia.
In this interrelationship, psychological factors such as stress and
negative emotions can influence the emergence and worsening
of skin disorders, and on the other hand, psychological disorders
can be the result of some skin diseases [209]. Skin, mental health
and the central nervous system are interconnected. Individuals
with HS often suffer from Depression and anxiety. Other associated psychiatric disorders include substance abuse, psychotic and
bipolar disorders, and suicide risk [191].
Hidradenitis suppurativa and oral and systemic health
Oral manifestations are found with high frequency in cases of
concomitant autoimmune, autoinflammatory, systemic chronic
diseases. General dysregulation of IL-17 may thus contribute to
host changes that lead to oral microbial dysbiosis. Interestingly,
a key role for the IL-17 pathway in the pathogenesis of HS has recently emerged, strengthening the possible relationship between
HS and oral lesions. Furthermore, HS shares etiopathogenetic
similarities with oral lesions, as genetic susceptibility, environmental factors, and immunopathological mechanisms can lead to
a dysregulation of the inflammatory response [38].
Common immune-mediated oral diseases include rheumatic
disorders, ulcerated and erythematous lesions such as recurrent
aphthous stomatitis, erythema multiform and drug-related ulcerations, lichenoid lesions, vesiculobullous lesions, benign migratory glossitis, desquamative gingivitis, and orofacial granulomatosis.
Most of these lesions, as well as HS, which is characteristically
relapsing, persist and recur frequently, and may be the first clinical signs or symptoms of the general disease [38].
Dental prophylaxis and dental consultations are extremely
important to maintain quality of life and good digestion, two parameters that are particularly important in patients with chronic
diseases. Dental-dermatological cooperation must be improved
to create ad hoc in-hospital integrated care pathways for HS patients, especially those who are biologic candidates who have to
undergo a mandatory oral health assessment. Dental prophylaxis
should be promoted every 3 months in patients with HS and further studies are needed to understand the impact of HS therapies
on oral comorbidities (i.e., epigenetics [31-33] and resistome)
[38].
As results a total of 102 patients (44.0±0.9 years, body mass
index 27.0±2.2 kg/m2
) were enrolled. Remarkably, 48% and 43%
did not undergo at least an oral hygiene or a dental visit each year,
respectively. Oral disorders were found in 55.9% of patients with
HS, in particular 39.2% had caries and 46.7% reported at least one
missing tooth. The main oral manifestations in patients with HS
were recurrent aphthous stomatitis (N=19, 19.2%), amalgam tattoo (N=14, 14.1%), leukoplakia (N=11, 11.1%), nicotinic stomatitis
(N=9, 9.1%), papilloma (N=8, 8.1%), and geographic tongue (N=8,
8.1%). Whilst the main predictor of oral pathological conditions
was Hurley staging (P=0.0276), multivariate regression analysis
indicated that gender and International Hidradenitis Suppurativa
Severity Score System (IHS4) were the main predictors for the
presence of caries and number of missing teeth [38].
Today we already have strong enough scientific evidence to affirm that risk factors such as smoking and neuropsychic disorders
affect oral and systemic health levels in different clinical scenarios
certified for psoriasis. Using the principles of specificity and sensitivity, we can state that there are great possibilities for HS to also
be subject to such complications, after all this is also an inflammatory dermatosis.
Hidradenitis suppurativa and the repercussions on women’s
health
HS is particularly prevalent in women of childbearing age and
can have diverse psychological and physical consequences. Paradoxically, studies point to cases of HS that showed significant improvements during pregnancy, presumably related to gestational
hormones, and that around 90 days after birth, the conditions
worsen again [210]. The chronic and debilitating nature of this disease can lead to significant impairments in patients’ sexual health
and overall quality of life. There are qualitative systematic reviews
that have examined gender differences in the impact of HS on
sexual health. Additionally, we review gaps in the sexual health
management of patients with HS and outline recommendations
to appropriately address sexual concerns and optimize care [82].
Sexual distress is defined as negative emotions about sex, such
as regret, frustration, guilt, and unhappiness [188,162,81]. On the other hand, sexual dysfunction refers to deficiencies in the physical aspects of sexual activity, such as lubrication, penetration,
maintenance, orgasm, and resolution. Impaired sexual health includes sexual distress and sexual dysfunction.
Patients with HS often report impairments in sexual health resulting from the psychological and physical consequences of having this disease [189]. Contributing psychological deficiencies include depression, embarrassment, fear of contagion, and shame.
Physical disabilities include pain, drainage, itching, scarring, and
bad odor [189].
Studies on other chronic dermatological diseases, such as psoriasis, have found that compromised sexual health is particularly
prominent in women [211]. Few studies have specifically investigated how women’s and men’s sexual health may be affected
differently by HS.
This review examines the existing literature on gender differences in sexual health in patients with HS, identifies gaps in practice, and provides strategies to improve sexual health care.
HS is a highly burdensome chronic disease that is significantly
associated with deficiencies in sexual health in several validated
instruments in male and female patients. The sexual health burden caused by HS appears to be greater for women. Additional
studies are needed to further elucidate the differential impact of
HE on sexual disability by gender. This may also shed light on specific interventions that may be beneficial for women or men. Impairments in quality of life due to sexual health can be mitigated
with proactive medical questioning and counseling about sexual
health in all patients with HS, regardless of the presence of genital lesions. Sexual health should be addressed when evaluating
the severity of HS and treatment outcome. Increasing awareness
about sexual disability in HS is essential to optimize care.
Hidradenitis suppurativa and Severity, treatment and quality
of life
According to the World Health Organization, quality of life refers to “an individual’s perception of their position in the world,
in the context of the culture and value systems in which they live
and in relation to their goals, expectations, standards and concerns”. Seeking a better quality of life implies seeking improvements, whether in physical, mental, and emotional well-being, in
health, education, purchasing power or in personal relationships
with friends or family.
The impact of Hidradenitis suppurativa on the quality of life
of patients, spouses, family members and/or caregivers is widely
discussed. Many aspects of the disease contribute to this reduction. Several instruments are being created to measure these
aspects, some better evaluated, others less so. The Dermatology
Life Quality Index (DLQI) is the most used and specific instrument
in Dermatology.
Other instruments include: HIDRAdisk, HSIA, HiSQoL,
HSQoL-24, Skindex, Euroqol 5-Dimensional Questionnaire (EQ5D) and Short Form 36 Questionnaire (SF-36), Hospital Anxiety
and Depression Scale (HADS), Hospital Depression Inventory Bek
(BDI), Major Depression Inventory (MDI), Female Sexual Function Index (FSFI-6), 5-Item International Index of Erectile Function
(IIEF-5), Visual Analogue Scale (VAS) and Numerical Scale (NRS). The latter assess the severity of symptoms [212]. The Harley classification, the HS-PGA and the Modified Sartorius Scale (MSS) are
widely used to assess disease severity [213].
HS is observed as one of the worst dermatoses as it causes
immense impairment of patients’ quality of life. It is characterized by debilitating pain, purulent secretion, unpleasant odor and
itching, factors associated with disastrous social and economic
consequences, higher rates of depression, stigmatization and suicide [214] as previously discussed. The severity of the disease, the
number of exacerbations and the location of the lesions are identified as the main factors responsible for the worsening of quality
of life. The greater the intensity of the signal or symptom, the
worse the general quality of life or specific dimensions of quality of life, whether sexual suffering, anxiety, depression or sleep
[212]. Female sex, less education and genital involvement are also
factors associated with worse health-related quality of life [215].
The mean Family Dermatology Life Quality Index Questionnaire
(FDLQI) for partners of 50 patients with HS was 8.7±6.8, indicating
a moderate impact of HS on their lives. The partners’ quality of life
was significantly correlated with the severity of the disease [216].
Both patients and cohabitants experience significant impairment
in quality of life. DLQI scores were associated with the presence
of negative affectivity, typical type D personality traits and cohabitants’ anxiety, while FDLQI scores were associated with patient
depression and cohabitant anxiety [217]. Patients with more severe HS tend to have a worse quality of life. The time dedicated
to care and the emotional suffering generated are two factors responsible for reducing the caregiver’s quality of life [218]. Women
are related to a high prevalence of sexual dysfunction, and men,
to a high prevalence of erectile dysfunction, as are male partners
[219].
Numerous treatment measures show a positive response in
the health-related quality of life of patients. Most of the assessment instruments developed so far aim to measure the response
to treatment.
As HS is a heterogeneous and multifactorial disease, it is important to establish different interventions that seek to improve
patients’ quality of life while at the same time being able to be
properly measured. Several clinical and surgical treatments have
been proposed in this regard.
Biological and immunomodulatory products have shown important reductions in DLQI scores. The anti-Interleukin (IL)-17
monoclonal antibody, Secukinumab, at a dose of 300 mg, subcutaneously, once a week for five weeks, and then every four
weeks for 24 weeks, favored a reduction in the DLQI score of 13
to 7 [211]. Ustekinumab, in an intravenous infusion adjusted for
weight, followed by a subcutaneous maintenance dose of 90 mg
every eight weeks, over a period of sixteen weeks, enabled an
improvement in DLQI in 71.42% of the 14 patients [220]. Moderate to marked improvement in the modified Sartorius score was
achieved at week 40 in 82% of the 12 patients who completed
the protocol with Ustekinumab 45 or 90 mg at weeks 0, 4, 16 and
28 [221]. With adalimumab, a TNF-α inactivator, 77% (n=78/101)
of patients reported improvement in PGA-HS scores and significant improvements in DLQI scores [222]. The count of the number of lesions, the International Hidradenitis Suppurativa Severity Score System (IHS4), the Visual Analogue Scale (VAS) of pain decreased throughout the study, and the DLQI was reduced from
11.9 at week 0 to 6.6 at week 0. week 96 [223]. A multicenter
cohort study involving 389 patients with HS treated with Adalimumab also showed an improvement in quality of life. HiSCR was
achieved in 43.7% and 53.9% of patients at weeks 16 and 52 respectively, and significant reductions in DLQI and Visual Analogue
Scale pain were observed between weeks 0 and weeks 16 and 52
[224].
Greater efficacy was observed in cases of HS treated with an increase in the dose of Adalimumab from 40 mg to 80 mg, subcutaneously, once a week [2]. The use of Adalimumab 160 mg, subcutaneously, at the beginning of the study, 80 mg in week 2, 40 mg
in week 4 and 40 mg in subsequent weeks provided a reduction
in the modified Sartorius score of 74.93, before the start of treatment, to 39.86 at week 10 (P<0.0001) as well as the Hidradisk
mean value from 77.3 at the beginning of treatment to 51.86 at
week 10 (P<0.0001) [225]. Hidradisk also showed significant improvements, but more evident in men (69.8±6.2-49.6±10.8) than
in women (80.7±6.0-72.3-6.7) with P<0.001 [226].
Apremilast, 30 mg twice daily demonstrated efficacy, but
showed no significant difference in DLQI between the treatment
and placebo groups at week 16 [227]. In contrast, Apremilast was
effective in improving pain and quality of life in patients with mild
to moderate HS. Significant improvement was observed in DLQI
scores (11.6 to 5.4, P<0.01) after 24 weeks of treatment [228].
Antibiotics remain the first line of treatment for HS. A comparative, retrospective study evaluated 52 patients with mild, moderate and severe HS divided into two groups. Group A (26) patients
received 300 mg of Limecycline per day and group B (26 patients)
received the Clindamycin/Rifampicin combination, 600 mg, twice
a day, for ten weeks. Both groups showed significant improvement
in IHS4, pain Visual Analogue Scale (VAS) and DLQI compared to
baseline, although the improvement was more evident in group
A [229]. In the comparison of Clindamycin versus the Clindamycin/Rifampicin association, 60 patients with mild, moderate and
severe HS were divided into two groups. Group A (Clindamycin/
Rifampicin) and group B (Clindamycin), evaluated after 8 weeks of
treatment. The two groups showed similar improvements in the
IHs4 score, while the DLQI and Visual Analogue Scale pain scores
showed a more significant improvement in group B [230].
In the treatment of HS, the combination of Intense Pulsed Light
(IPL) and Radio Frequency (RF), after 12 weeks, showed a greater
reduction in the number of lesions when compared to the groups
treated with LIP or RF alone. The improvement in DLQI was significantly greater in the group treated with the combination of
intense pulsed light and radiofrequency [231].
Botulinum Toxin type B, when compared to the placebo group,
provided an improvement in the DLQI from 17, at the beginning
of treatment to 8, in 3 months (P<0.05), possibly due to the reduction in the total number of lesions, thus improving, the quality of
life of patients with HS [232].
Treatments with intralesional corticosteroids, two intralesional injections of Triamcinolone and Leucomycin guided by Ultrasound, at the beginning and after 2 weeks, provided a significant
improvement from 36.2 at the beginning of the study to 53.9, on
the SF-36 scale (Bodily Pain Scale). Short-Form Health Survey) in the fourth week after intralesional therapy [233].
Regarding surgical treatment, in a study with one hundred and
forty-nine patients treated with surgical intervention, Sartorius
scores showed a significant improvement in relation to baseline
values (P<0.001). 83 patients achieved a DLQI MCID and 75 patients achieved an NRS for MCID; while in the 19 patients who
underwent combined clinical and surgical treatment, 9 achieved
significant improvement in pain scores, DLQI and NRS, MCIDs and
Sartorius [234].
Comparative study between the use of artificial dermis and
pedicled perforator flaps after radical surgery, evaluating quality of life using the SF-36 Scale, showed a significant increase in
quality of life both in the use of artificial dermis and in the use of
perforator flap , but the effect was considered greater when using
the perforator flap (P<0.001).
DLQI showed a reduction in the impact of HS on patients’ quality of life in both groups, but once again the reduction in the impact of HS was greater in the perforator flap group [235]. Wide
local excisions followed by reconstructions with pedicled perforator flaps, which 26 patients with HS Hurley III underwent, enabled
a reduction in DLQI from 21.31±4.79 before the first surgery to
5±2.95 after the last segment (P<0.0001) [236].
Considering surgical results and the impact of major surgery on
the quality of life, impairment of activity and sexual health of patients with HS, questionnaires answered by 39 patients with 171
survey responses concluded that patients with HS Hurley I and II
had lower wound closure time when compared with HS Hurley III
(P=0.005). DLQI and ASEX scores did not show significant improvement during the six months of study, but activity and general work
impairment improved considerably after surgical treatment [237].
The use of the HS Burden of Disease (HSBOD) score showed
that even with surgical intervention in HS, patients’ quality of life
continues to suffer impacts in the five domains evaluated, that is,
symptoms and feelings, daily activities, leisure, work and school,
and personal relationships [238]. However, surgical treatment has
revealed great potential in improving the quality of life of patients
with the severe form of HS. In a systematic review, 33 articles
were selected, including 286 patients and 387 flaps. 15.1% of
flaps presented at least one complication, but pedicled perforator
flaps proved to be reliable and reproducible in the reconstruction
of defects caused by HS, as they were associated with effective
reconstruction, with lower morbidity and faster recovery [239].
Surgical treatment effectively improves the quality of life related
to post-surgical health [240,241].
Final considerations: Practical and research implications
Analyzing the influence of social factors on health, the importance of time, place and people’s way of life is observed. Education, work, income and racial contextualization, shaping behaviors
and lifestyles, stand out as important factors determining health.
It is known that poverty and health have always been related, and
currently social and economic influences on health constitute an
important point of discussion.
Countless information has been accumulated; Knowledge gaps
have been highlighted and research priorities have been highlighted. Health in general goes far beyond medical care, and results from the interaction, complex or not, of multiple factors. It
is important to remember how the conditions in which they live,
reside or work can, directly or indirectly, influence people’s health
status, and how behaviors and choices, individual or collective,
political or not, can have a direct impact on health.
Education, work and income are important social factors. It is
known that the greater the social disadvantage, the greater the
precarious health. A higher educational level can translate into a
better occupation, a more profitable profession, greater employment opportunities, higher income, higher economic resources
(wealth) and consequently better health conditions, that is, better
housing and neighborhood conditions, better nutritional conditions and lower levels of stress factors. Living or not living in areas
with better infrastructure conditions or more favorable conditions
(schools, transport, piped/treated water, adequate medical care,
job offers) provide better health conditions, create and signal socioeconomic and ethnic-racial disparities.
Social relationships based on the exchange of trust favor security, lower rates of violence and social infractions and consequently, lower rates of chronic diseases such as anxiety and depression,
which provides improvements in health indicators in general,
even considering the particularities of each individual.
Work, in its physical and psychosocial aspects, has a great influence on health status. Work-related illnesses can result from
several factors: repetitive movements, inadequate posture or
conditions, psychological pressure or high-stress situations, excessive and excessive lifting of weight or strenuous work, sedentary lifestyle or physically inactive functions, pressure for results
or goals unattainable, harassment in the workplace, high-stress
situations; On the other hand, opportunities and resources arising
from work, such as lectures and training that reinforce the need
and correct use of Personal Protective Equipment (PPE), worker
training, periodic exams, paid leave or vacation, flexible schedules
or shifts, programs that provide well-being in the workplace, such
as workplace gymnastics, health plans and retirement benefits,
are extremely beneficial for health as a whole. A well-conducted
and/or paid job can translate into better benefits, greater financial
security and, consequently, better living conditions, while lower
remuneration or lower salaries can translate into fewer healthrelated benefits or unfavorable living conditions.
It is known that educational level creates employment opportunities. Higher education can translate into higher employment
rates, employment with better physical and psychosocial working conditions, better remuneration and greater benefits, greater
perceived personal control and, consequently, better health conditions and health-related behaviors. Unemployment, in turn, can
translate into worse health conditions and higher morbidity and
mortality rates. Greater education can translate into greater social support and, consequently, better physical and mental health
conditions. Knowledge about health, behaviors and adoption of
healthy habits in the daily routine provided by higher educational
levels enable more adequate management of medical care and
health promotion policies. Hidradenitis suppurativa, even though
it is not considered an occupational disease, can be aggravated by
the exercise of some professions. Just remember how much absenteeism, presenteeism at work or lack of opportunities at work
can harm people with HS.
In addition to educational level, greater economic resources
provide easier access to goods and services, which can translate
into better health conditions.
Race and ethnicity are other factors that can positively or negatively influence health. Racism and/or social structures associated
with it can often limit resources or opportunities for people or institutions. Blacks, Latinos, or people with less education are more
likely to live in less favored areas, where the lack of infrastructure
or better resources contributes to more unfavorable health outcomes. Fact to remember is how a person’s race or ethnicity can
determine their place in different social classes.
Chronic HS disease negatively influences the patient’s physical, social and psychological functions, often severely affecting
their quality of life in all its aspects. HS, depending on the classification, involves greater financial expenses, feelings of shame
and anguish, social isolation, loneliness, low self-esteem, anxiety
and depression. The HS-BNSE relationships are evident even if
the causal link is not entirely clear. The two main determining or
aggravating factors of HS, smoking and obesity, have a broad relationship with BNSE, as previously demonstrated. Limited social
and financial resources are directly related to HS. Such limitations
may be the result of the difficulty the patient had in achieving a
better level of education or employment or may be the result of
loss of ability to work or loss of employment due to the negative
effects of the disease.
HS can favor the loss of independence. The chronicity of the
disease or the lack of hope for a cure generates hopelessness, and
the feeling of dependence can generate dissatisfaction with life,
anxiety, depression, mood disorders, and even attempts against
one’s own life.
In addition to smoking and obesity, anxiety and depression,
frequently observed in HS patients, may also have their origins
or chronicity favored by BNSE, and lower socioeconomic position
implies a greater possibility of experiences with negative emotions. The BNSE can also affect the implementation of strategies
to combat the disease, whether due to the consequences of low
education and/or the lack of financial resources that provide adequate medical assistance, purchase of medicines and even the
assimilation and practice of prophylactic measures related to the
disease illness.
Furthermore, BNSE is generally associated with a maladaptive
coping style, that is, linked to feelings of denial, social isolation
and self-blame, which in turn favor more unfavorable health outcomes. In this context, it is important to remember the importance of strengthening resilience through which patients with HS
can adopt a more adaptive coping style, that is, a lifestyle where
even in the face of BNSE, the search for social support, help, acceptance and positive evaluation provide a better quality of life.
In conclusion, we sought to summarize how social factors influence HS, whether through triggering factors and/or aggravating
factors such as smoking, obesity, anxiety, depression and other
comorbidities such as chronic inflammatory diseases, observing
as a point, often common to these diseases, the direct influence
of BNSE. Despite the evidence, the causal link between BNSE and
HS still needs to be clarified, and the limitations of this study must
be considered.
With the aim of estimating the biopsychosocial impacts on patients’ lives, this qualitative systematic review was prepared, and
the results were compatible with the observed clinical reality and,
as implications for practice, it is strongly recommended to adopt
applied treatment modalities in a co-intervention regime, with
the aim of increasing the levels of efficacy, effectiveness and safety of services through Good Clinical Practices. As implications for
research, studies of better methodological quality are suggested,
such as randomized clinical trials.
References
- Monson CA, Monson ASC. Terapias Complementares para o Paciente Crônico na Perspectiva da Saúde Baseada em Evidências. 1ª ed. Ed. Appris. Curitiba. 2019.
- Zouboulis CC, Hansen H, Caposiena Caro RD, Damiani G, Delorme I, et al. Adalimumab Dose Intensification in Recalcitrant Hidradenitis Suppurativa/Acne Inversa. Dermatology. 2020; 236(1): 25-30. doi: 10.1159/000503606.
- Calao M, Wilson JL, Spelman L, Billot L, Rubel D, et al. Hidradenitis Suppurativa (HS) prevalence, demographics and management pathways in Australia: A population-based cross-sectional study. PLoS One. 2018; 13(7): e0200683.
- Ingram JR, Hadjieconomou S, Piguet V. Development of core outcome sets in hidradenitis suppurativa: Systematic review of outcome measure instruments to inform the process. Br J Dermatol. 2016; 175(2): 263-72.
- Scheinfeld N. Hidradenitis suppurativa: A practical review of possible medical treatments based on over 350 hidradenitis patients. Dermatol Online J. 2013; 19(4): 1.
- Gutierrez N, Cohen PR. Ectopic Hidradenitis Suppurativa: Case Report and Review of Literature. Cureus. 2021; 13(1): e12966.
- Cartron A, Driscoll MS. Comorbidities of hidradenitis suppurativa: A review of the literature. Int J Womens Dermatol. 2019; 5(5): 330-334. doi: 10.1016/j.ijwd.2019.06.026.
- Wang Z, Yan Y, Wang B. γ-Secretase Genetics of Hidradenitis Suppurativa: A Systematic Literature Review. Dermatology. 2021; 237(5): 698-704. doi: 10.1159/000512455.
- Matusiak L, Bieniek A, Szepietowski JC. Hidradenitis suppurativa and associated factors: still unsolved problems. J Am Acad Dermatol. 2009; 61(2): 362-5. doi: 10.1016/j.jaad.2009.03.043. PMID: 19615551.
- Saunte DML, Jemec GBE. Hidradenitis Suppurativa: Advances in Diagnosis and Treatment. JAMA. 2017; 318(20): 2019-2032. doi: 10.1001/jama.2017.16691.
- Heidenreich A, Lembrande RO, Villarroel A. Trilogy of follicular obstruction. ABCD Arq. Bras. Cir. Dig. 1990; 87-91.
- Chu CB, Yang CC, Tsai SJ. Hidradenitis suppurativa: Disease pathophysiology and sex hormones. Chin J Physiol. 2021; 64(6): 257-265. doi: 10.4103/cjp.cjp_67_21.
- Ingram JR. The epidemiology of hidradenitis suppurativa. Br J Dermatol. 2020; 183(6): 990-998. doi: 10.1111/bjd.19435.
- Micheletti RG. Hidradenitis suppurativa: current views on epidemiology, pathogenesis, and pathophysiology. Semin Cutan Med Surg. 2014; 33(3 Suppl): S48-50. doi: 10.12788/j.sder.0091.
- Boer J, Weltevreden EF. Hidradenitis suppurativa or acne inversa. A clinicopathological study of early lesions. Br J Dermatol. 1996; 135(5): 721-5.
- von Laffert M, Helmbold P, Wohlrab J, Fiedler E, Stadie V, et al. Hidradenitis suppurativa (acne inversa): early inflammatory events at terminal follicles and at interfollicular epidermis. Exp Dermatol. 2010; 19(6): 533-7. doi: 10.1111/j.1600-0625.2009.00915.x.
- Von Laffert M, Stadie V, Wohlrab J, Marsch WC. Hidradenitis suppurativa/acne inversa: bilocated epithelial hyperplasia with very different sequelae. Br J Dermatol. 2011; 164(2): 367-71. doi: 10.1111/j.1365-2133.2010.10034.x.
- Wang B, Yang W, Wen W, Sun J, Su B, et al. Gamma-secretase gene mutations in familial acne inversa. Science. 2010; 330(6007): 1065. doi: 10.1126/science.1196284.
- Ring HC, Bay L, Kallenbach K, Miller IM, Prens E, et al. Normal Skin Microbiota is Altered in Pre-clinical Hidradenitis Suppurativa. Acta Derm Venereol. 2017; 97(2): 208-213. doi: 10.2340/00015555-2503.
- Schell SL, Cong Z, Sennett ML, Gettle SL, Longenecker AL, et al. Keratinocytes and immune cells in the epidermis are key drivers of inflammation in hidradenitis suppurativa providing a rationale for novel topical therapies. Br J Dermatol. 2023; 188(3): 407-419. doi: 10.1093/bjd/ljac096.
- Orvain C, Lin YL, Jean-Louis F, Hocini H, Hersant B, et al. Hair follicle stem cell replication stress drives IFI16/STING-dependent inflammation in hidradenitis suppurativa. J Clin Invest. 2020; 130(7): 3777-3790. doi: 10.1172/JCI131180.
- Schell SL, Schneider AM, Nelson AM. Yin and Yang: A disrupted skin microbiome and an aberrant host immune response in hidradenitis suppurativa. Exp Dermatol. 2021; 30(10): 1453-1470. doi: 10.1111/exd.14398.
- Mintoff D, Borg I, Pace NP. The Clinical Relevance of the Microbiome in Hidradenitis Suppurativa: A Systematic Review. Vaccines (Basel). 2021; 9(10): 1076. doi: 10.3390/vaccines9101076.
- Frew JW, Hawkes JE, Krueger JG. A systematic review and critical evaluation of immunohistochemical associations in hidradenitis suppurativa. F1000Res. 2018; 7: 1923. doi: 10.12688/f1000research.17268.2.
- Hoffman LK, Ghias MH, Lowes MA. Pathophysiology of hidradenitis suppurativa. Semin Cutan Med Surg. 2017; 36(2): 47-54. doi: 10.12788/j.sder.2017.017.
- Riis PT, Ring HC, Themstrup L, Jemec GB. The Role of Androgens and Estrogens in Hidradenitis Suppurativa - A Systematic Review. Acta Dermatovenerol Croat. 2016; 24(4): 239-249.
- Boer J, Nazary M, Riis PT. The Role of Mechanical Stress in Hidradenitis Suppurativa. Dermatol Clin. 2016; 34(1): 37-43. doi: 10.1016/j.det.2015.08.011.
- Sartorius K, Emtestam L, Jemec GB, Lapins J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol. 2009; 161(4): 831-9. doi: 10.1111/j.1365-2133.2009.09198.x.
- Wertenteil S, Strunk A, Garg A. Association of Low Socioeconomic Status With Hidradenitis Suppurativa in the United States. JAMA Dermatol. 2018; 154(9): 1086-1088. doi: 10.1001/jamadermatol.2018.2117.
- Scuderi N, Monfrecola A, Dessy LA, Fabbrocini G, Megna M, et al. Medical and Surgical Treatment of Hidradenitis Suppurativa: A Review. Skin Appendage Disord. 2017; 3(2): 95-110. doi: 10.1159/000462979.
- Dufour DN, Emtestam L, Jemec GB. Hidradenitis suppurativa: a common and burdensome, yet under-recognised, inflammatory skin disease. Postgrad Med J. 2014; 90(1062): 216-21; quiz 220. doi: 10.1136/postgradmedj-2013-131994.
- Liy-Wong C, Pope E, Lara-Corrales I. Hidradenitis suppurativa in the pediatric population. J Am Acad Dermatol. 2015; 73(5 Suppl 1): S36-41. doi: 10.1016/j.jaad.2015.07.051.
- Garg A, Kirby JS, Lavian J, Lin G, Strunk A. Sex- and Age-Adjusted Population Analysis of Prevalence Estimates for Hidradenitis Suppurativa in the United States. JAMA Dermatol. 2017; 153(8): 760-764. doi: 10.1001/jamadermatol.2017.0201.
- Magalhães RF, Rivitti-Machado MC, Duarte GV, Souto R, Nunes DH, et al. Consensus on the treatment of hidradenitis suppurativa - Brazilian Society of Dermatology. An Bras Dermatol. 2019; 94(2 Suppl 1): 7-19. doi: 10.1590/abd1806-4841.20198607.
- Andrade TCPC, Vieira BC, Oliveira AMN, Martins TY, Santiago TM, et al. Hidradenitis suppurativa: Epidemiological study of cases diagnosed at a dermatological reference center in the city of Bauru, in the Brazilian southeast State of São Paulo, between 2005 and 2015. An Bras Dermatol. 2017; 92(2): 196-199. doi: 10.1590/abd1806-4841.20175588.
- Jemec GB, Kimball AB. Hidradenitis suppurativa: Epidemiology and scope of the problem. J Am Acad Dermatol. 2015; 73(5 Suppl 1): S4-7. doi: 10.1016/j.jaad.2015.07.052.
- Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017; 358: j4008.
- Giovanni Damiani, Pierpaolo Poli, Alessia Pacifico, Elia Rosi, Giovanni Allocca, et al. The Relevant Oral Burden with Hidradenitis Suppurativa. Dermatology and Therapy. 2023; 13: 2319-2329. https://doi.org/10.1007/s13555-023-01006-x
- Danielle Yee, Erin K Collier , Swetha Atluri , Joanna Jaros , Vivian Y Shi, et al. Gender differences in sexual health impairment in hidradenitis suppurativa: A systematic review. Int J Womens Dermatol. 2020; 7(3): 259-264. doi: 10.1016/j.ijwd.2020.10.010.
- Lorite-Fuentes I, Montero-Vilchez T, Arias-Santiago S, Molina-Leyva A. Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population. Nutrients. 2022; 14(3): 551. doi: 10.3390/nu14030551.
- Katoulis AC, Liakou AI, Rotsiamis N, Bonovas S, Bozi E, et al Descriptive Epidemiology of Hidradenitis Suppurativa in Greece: A Study of 152 Cases Skin Appendage Disord. 2017; 3(4): 197-201.
- Kluger N, Ranta M, Serlachius M The Burden of Hidradenitis Suppurativa in a Cohort of Patients in Southern Finland: A Pilot Study Skin Appendage Disord. 2017; 3(1): 20-27.
- Delany E, Gormley G, Hughes R, McCarthy S, et al. cross-sectional epidemiological study of hidradenitis suppurativa in an Irish population (SHIP) J Eur Acad Dermatol Venereol. 2018; 32(3): 467-473.
- Schultheis M, Grabbe S, Staubach P, Hennig K, Mauch M, et al. Clinical Features of Persons Suffering from Acne Inversa Dtsch Arztebl Int. 2023; 120(19): 345-346.
- Loo CH, Tan WC, Tang JJ, Khor YH, Manikam MT, et al. The clinical, biochemical, and ultrasonographic characteristics of patients with hidradenitis suppurativa in Northern Peninsular Malaysia: A multicenter study Int J Dermatol. 2018; 57(12): 1454-1463.
- Hammud A, Avitan-Hersh E, Khamaysi Z. Clinical-Epidemiological Characteristics of Hidradenitis Suppurativa: A Retrospective Cohort Study from a Tertiary Care Centre in Northern Israel Journal of Clinical Medicine 2023; 12(12): 3921.
- Choi E, Cook AR, Chandran NS. Hidradenitis Suppurativa: An Asian Perspective from a Singaporean Institute Skin Appendage Disord. 2018; 4(4): 281-285.
- Yüksel M, Basım P. Demographic and Clinical Features of Hidradenitis Suppurativa in Turkey J Cutan Med Surg. 2020; 24(1): 55-59.
- Alsadhan H, Alfawzan AI, Yaqoub A, Almoneef A, Almohideb M. Hidradenitis Suppurativa: Estimated Prevalence, Clinical Features, and Risk Factors in Riyadh, Saudi Arabia Cureus. 2022; 14(3): e23029.
- Hayama K, Fujita H, Hashimoto T, Terui T. Japanese HS Research Group Questionnaire-based epidemiological study of hidradenitis suppurativa in Japan revealing characteristics different from those in Western countries J Dermatol. 2020; 47(7): 743-748.
- Vazquez BG, Alikhan A, Weaver AL, Wetter DA, Davis MD. Incidence of hidradenitis suppurativa and associated factors: A population-based study of Olmsted County, Minnesota J Invest Dermatol. 2013; 133(1): 97-103.
- Kamat D, Gaba S, Kumaran MS. Clínico-Epidemiological Characteristics of Hidradenitis Suppurativa: A Retrospective Cohort Study from a Tertiary Care Centre in Northern India Indian Dermatol Online. J 2021; 12(4): 561-565.
- Schrader AM, Deckers IE, van der Zee HH, Boer J, Prens EP. Hidradenitis suppurativa: A retrospective study of 846 Dutch patients to identify factors associated with disease severity J Am Acad Dermatol. 2014; 71(3): 460-7.
- Wang, Zhong-Shuai, Li, Jing, Ju Qiang, et al. Prevalence of Acne Inversa (Hidradenitis Suppurativa) in China: A Nationwide CrossSectional Epidemiological Study International Journal of Dermatology and Venereology. 2022; 5(1): 1-7.
- Fabbrocini G, De Vita V, Donnarumma M, Russo G, Monfrecola G. South Italy: A Privileged Perspective to Understand the Relationship between Hidradenitis Suppurativa and Overweight/Obesity Skin Appendage Disord. 2016; 2(1-2): 52-56.
- Clark AM, Des Meules M, Luo W, Duncan AS, Wielgosz A. Socioeconomic status and cardiovascular disease: risks and implications for care Nat Rev Cardiol. 2009; 6(11): 712-22.
- Majumder S. Socioeconomic status scales: Revised Kuppuswamy, BG Prasad, and Udai Pareekh’s scale updated for 2021 J Family Med Prim Care. 2021; 10(11): 3964-3967.
- Wani RT. Socioeconomic status scales-modified Kuppuswamy and Udai Pareekh’s scale updated for 2019 J Family Med Prim Care. 2019; 8(6): 1846-1849.
- Pawlak R. Economic considerations of health literacy Nurs Econ. 2005; 23(4): 173-80.
- Prens LM, Bouwman K, Troelstra LD, Prens EP, Alizadeh BZ, et al. New insights in hidradenitis suppurativa from a population-based Dutch cohort: Prevalence, smoking behaviour, socioeconomic status and comorbidities Br J Dermatol. 2022; 186(5): 814-822.
- Deckers IE, Janse IC, van der Zee HH, Nijsten T, Boer J, et al. Hidradenitis Suppurativa (HS) is associated with low socioeconomic status (SES): A cross-sectional reference study J Am Acad Dermatol. 2016; 75(4): 755-759e1.
- Williams DR, Mohammed SA, Leavell J, Collins C Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities Ann N Y Acad Sci. 2010; 1186: 69-101.
- Mielck A, Vogelmann M, Leidl R. Health-related quality of life and socioeconomic status: Inequalities among adults with a chronic disease Health Qual Life Outcomes. 2014; 12: 58.
- Killasli H, Sartorius K, Emtestam L, Svensson Å. Hidradenitis Suppurativa in Sweden: A Registry-Based Cross-Sectional Study of 13,538 Patients Dermatology. 2020; 236(4): 281-288.
- Matusiak Ł, Bieniek A, Szepietowski JC. Bacteriology of hidradenitis suppurativa - which antibiotics are the treatment of choice? Acta Derm Venereol. 2014; 94(6): 699-702.
- Kishimoto T. IL-6: From its discovery to clinical applications Int Immunol. 2010; 22(5): 347-52.
- De Britto Rosa NM, de Queiroz BZ, Pereira DS, di Sabatino Santos ML, Oliveira DM. Interleukin-6 plasma levels and socioeconomic status in Brazilian elderly community-dwelling women Arch Gerontol Geriatr. 201; 53(2): 196-9.
- Pietras SA, Goodman E. Socioeconomic status gradients in inflammation in adolescence Psychosom Med. 2013; 75(5): 442-8.
- Muscatell KA, Brosso SN, Humphreys KL. Socioeconomic status and inflammation: A meta-analysis Mol Psychiatry. 2020; 25(9): 2189-2199.
- Nosrati A, Torpey ME, Shokrian N, Ch’en PY, Andriano TM, et al. Adalimumab efficacy is inversely correlated with Body Mass Index (BMI) in hidradenitis suppurativa Int J Dermatol. 2023; 62(6): 764-769.
- Xu H, Xiao X, He Y, Zhang X, Li C, et al. Increased serum interleukin-6 levels in patients with hidradenitis suppurativa Postepy Dermatol Alergol. 2017; 34(1): 82-84.
- Jiménez-Gallo D, de la Varga-Martínez R, Ossorio-García L, Albarrán-Planelles C, Rodríguez C, et al. The Clinical Significance of Increased Serum Proinflammatory Cytokines, C-Reactive Protein, and Erythrocyte Sedimentation Rate in Patients with Hidradenitis Suppurativa Mediators Inflamm. 2017; 2017: 2450401.
- Ingram JR, Jenkins-Jones S, Knipe DW, Morgan CLI, Cannings-John R, et al. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa Br J Dermatol. 2018; 178(4): 917-924.
- Omine T, Miyagi T, Hayashi K, Yamaguchi S, Takahashi K. Clinical characteristics of hidradenitis suppurativa patients in Okinawa, Japan: Differences between East Asia and Western countries. J Dermatol 2020; 47(8): 855-862.
- Yang JH, Moon J, Kye YC, Kim KJ, Kim MN, et al. Korean Society for Acne Research Demographic and clinical features of hidradenitis suppurativa in Korea J Dermatol. 2018; 45(12): 1389-1395.
- Offidani A, Molinelli E, Sechi A, Brisigotti V, Campanati A. Hidradenitis suppurativa in a prepubertal case series: A call for specific guidelines J Eur Acad Dermatol Venereol. 2019; 6: 28-31.
- Mengesha YM, Holcombe TC, Hansen RC. Prepubertal hidradenitis suppurativa: Two case reports and review of the literature Pediatr Dermatol. 1999; 16(4): 292-6.
- Shih T, Seivright JR, McKenzie SA, Harview CL, Truong AK, et al. Gender differences in hidradenitis suppurativa characteristics: A retrospective cohort analysis. Int J Womens Dermatol. 2021; 7(5Part B): 672-674.
- Cuenca-Barrales C, Montero-Vílchez T, Szepietowski JC, Matusiak L, Molina-Leyva A. Sexual impairment in patients with hidradenitis suppurativa: A systematic review J Eur Acad Dermatol Venereol. 2021; 35(2): 345-352.
- Cuenca-Barrales C, Montero-Vilchez T, Krajewski PK, Szepietowski JC, Matusiak L, et al. Sexual Dysfunction and Quality of Life in Patients with Hidradenitis Suppurativa and Their Partners Int J Environ Res Public Health. 2022; 20(1): 389.
- Sampogna F, Abeni D, Gieler U, Tomas-Aragones L, Lien L, et al. Impairment of Sexual Life in 3,485 Dermatological Outpatients From a Multicentre Study in 13 European Countries. Acta Derm Venereol. 2017; 97(4): 478-482. doi: 10.2340/00015555-2561.
- Seetan K, Al-Zubi M, Al-Omari R. Sexual Dysfunction in Patients with Hidradenitis Suppurativa: A Systematic Review and MetaAnalysis. J Clin Aesthet Dermatol. 2021; 14(8): 61-65.
- Mineroff J, Nguyen JK, Jagdeo J. Racial and ethnic underrepresentation in dermatology clinical trials. J Am Acad Dermatol. 2023; 89(2): 293-300. doi: 10.1016/j.jaad.2023.04.011.
- Nock MR, Barbieri JS, Krueger LD, Cohen JM. Racial and ethnic differences in barriers to care among US adults with chronic inflammatory skin diseases: A cross-sectional study of the All of Us Research Program. J Am Acad Dermatol. 2023; 88(3): 568-576. doi: 10.1016/j.jaad.2022.09.054.
- Brown SG 3rd, Cobb CBC, Harvey VM. Racial and Ethnic Health Disparities in Dermatology. Dermatol Clin. 2023; 41(2): 325-333. doi: 10.1016/j.det.2022.10.003.
- Ulschmid C, Serrano L, Wu R, Roth GM, Sokumbi O. African American race is a risk factor for severe hidradenitis suppurativa. Int J Dermatol. 2023; 62(5): 657-663. doi: 10.1111/ijd.16428.
- Sachdeva M, Shah M, Alavi A. Race-Specific Prevalence of Hidradenitis Suppurativa. J Cutan Med Surg. 2021; 25(2): 177-187. doi: 10.1177/1203475420972348.
- Price KN, Hsiao JL, Shi VY. Race and Ethnicity Gaps in Global Hidradenitis Suppurativa Clinical Trials. Dermatology. 2021; 237(1): 97-102. doi: 10.1159/000504911.
- Vlassova N, Kuhn D, Okoye GA. Hidradenitis suppurativa disproportionately affects African Americans: A single-center retrospective analysis. Acta Derm Venereol. 2015; 95(8): 990-1. doi: 10.2340/00015555-2176.
- Lee DE, Clark AK, Shi VY. Hidradenitis Suppurativa: Disease Burden and Etiology in Skin of Color. Dermatology. 2017; 233(6): 456-461. doi: 10.1159/000486741.
- Cullen MR, Lemeshow AR, Russo LJ, Barnes DM, Ababio Y, et al. Disease-Specific Health Disparities: A Targeted Review Focusing on Race and Ethnicity. Healthcare (Basel). 2022; 10(4): 603. doi: 10.3390/healthcare10040603.
- McKay C, Kuraitis D, Murina A. Serum cytokine levels in patients with hidradenitis suppurativa vary with race. J Am Acad Dermatol. 2021; 84(5): 1405-1406. doi: 10.1016/j.jaad.2020.08.084.
- Serrano L, Ulschmid C, Szabo A, Roth G, Sokumbi O. Racial disparities of delay in diagnosis and dermatologic care for hidradenitis suppurativa. Journal of the National Medical Association. 2022; 114(6): 613-616.
- Kilgour JM, Li S, Sarin KY. Hidradenitis suppurativa in patients of color is associated with increased disease severity and healthcare utilization: A retrospective analysis of 2 U.S. cohorts. JAAD Int. 2021; 3: 42-52. doi: 10.1016/j.jdin.2021.01.007.
- Udechukwu NS, Fleischer AB Jr. Higher Risk of Care for Hidradenitis Suppurativa in African American and Non-Hispanic Patients in the United States. J Natl Med Assoc. 2017; 109(1): 44-48. doi: 10.1016/j.jnma.2016.09.002.
- Robinson I, Lee L, Cotton C. The Impact of Racial Differences on Treatment Strategies in Hidradenitis Suppurativa: A Retrospective Review. J Drugs Dermatol. 2022; 21(3): 270-275. doi: 10.36849/JDD.6446.
- Edigin E, Kaul S, Eseaton PO, Albrecht J. Racial and Ethnic Distribution of Patients Hospitalized With Hidradenitis Suppurativa, 2008-2018. JAMA Dermatol. 2021; 157(9): 1125-1127. doi: 10.1001/jamadermatol.2021.2999.
- Ramos-Rodriguez AJ, Timerman D, Khan A, Bonomo L, Hunjan MK, et al. The in-hospital burden of hidradenitis suppurativa in patients with inflammatory bowel disease: A decade nationwide analysis from 2004 to 2014. Int J Dermatol. 2018; 57(5): 547-552. doi: 10.1111/ijd.13932.
- Paradies Y. A systematic review of empirical research on self-reported racism and health. Int J Epidemiol. 2006; 35(4): 888-901. doi: 10.1093/ije/dyl056.
- Gee GC, Ro A, Shariff-Marco S, Chae D. Racial discrimination and health among Asian Americans: Evidence, assessment, and directions for future research. Epidemiol Rev. 2009; 31: 130-51. doi: 10.1093/epirev/mxp009.
- Priest N, Paradies Y, Trenerry B, Truong M, Karlsen S, et al. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Soc Sci Med. 2013; 95: 115-27. doi: 10.1016/j.socscimed.2012.11.031.
- Pascoe EA, Smart Richman L. Perceived discrimination and health: A meta-analytic review. Psychol Bull. 2009; 135(4): 531-54. doi: 10.1037/a0016059.
- James D. Health and Health-Related Correlates of Internalized Racism Among Racial/Ethnic Minorities: A Review of the Literature. J Racial Ethn Health Disparities. 2020; 7(4): 785-806. doi: 10.1007/s40615-020-00726-6. Epub 2020 Feb 21.
- Clark R, Anderson NB, Clark VR, Williams DR. Racism as a stressor for African Americans. A biopsychosocial model. Am Psychol. 1999; 54(10): 805-16. doi: 10.1037//0003-066x.54.10.805.
- Hua VJ, Kilgour JM, Cho HG, Li S, Sarin KY. Characterization of comorbidity heterogeneity among 13,667 patients with hidradenitis suppurativa. JCI Insight. 2021; 6(21): e151872. doi: 10.1172/jci.insight.151872.
- Liakou AI, Papadakis M, Tsantes AG, Tsante KA, Kontochristopoulos G, et al. Perception and Knowledge of Hidradenitis Suppurativa in Greece: A Cross-Sectional Study of 1301 Individuals. Indian J Dermatol. 2022; 67(6): 835. doi: 10.4103/ijd.ijd_622_21.
- Marmot M G, Fuhrer R. Socioeconomic Position and Health across Midlife. In OG Brim, CD Ryff, RC Kessler (Eds.) How healthy are we?: A national study of well-being at midlife. The University of Chicago Press. 2004; 64-89.
- Koumaki D, Efthymiou O, Bozi E, Katoulis AC. Perspectives on Perceived Stigma and Self-Stigma in Patients with Hidradenitis Suppurativa. Clin Cosmet Investig Dermatol. 2019; 12: 785-790. doi: 10.2147/CCID.S180036.
- Van Straalen KR, Prens LM, Hylkema TH, Janse IC, Dickinson J, et al. Impact of hidradenitis suppurativa on work productivity and associated risk factors. J Am Acad Dermatol. 2021; 84(5): 1401-1405. doi: 10.1016/j.jaad.2020.07.115.
- Von der Werth JM, Williams HC. The natural history of hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2000; 14(5): 389-92. doi: 10.1046/j.1468-3083.2000.00087.x.
- Schneider-Burrus S, Kalus S, Fritz B, Wolk K, Gomis-Kleindienst S, et al. The impact of hidradenitis suppurativa on professional life. Br J Dermatol. 2023; 188(1): 122-130. doi: 10.1093/bjd/ljac027.
- Yao Y, Jørgensen AR, Thomsen SF. Work productivity and activity impairment in patients with hidradenitis suppurativa: A cross-sectional study. Int J Dermatol. 2020; 59(3): 333-340. doi: 10.1111/ijd.14706.
- Tzellos T, Yang H, Mu F, Calimlim B, Signorovitch J. Impact of hidradenitis suppurativa on work loss, indirect costs and income. Br J Dermatol. 2019; 181(1): 147-154. doi: 10.1111/bjd.17101.
- Gáspár K, Hunor Gergely L, Jenei B, Wikonkál N, Kinyó Á, et al. Resource utilization, work productivity and costs in patients with hidradenitis suppurativa: A cost-of-illness study. Expert Rev Pharmacoecon Outcomes Res. 2022; 22(3): 399-408. doi: 10.1080/14737167.2021.1895753.
- Tsentemeidou A, Sotiriou E, Sideris N, Kourouklidou A, Lallas A, et al. Adalimumab Effect on Pain in Hidradenitis Suppurativa Patients: Systematic Review and Meta-Analysis. Dermatol Pract Concept. 2022; 12(2): e2022099. doi: 10.5826/dpc.1202a99.
- Khalsa A, Liu G, Kirby JS. Increased utilization of emergency department and inpatient care by patients with hidradenitis suppurativa. J Am Acad Dermatol. 2015; 73(4): 609-14. doi: 10.1016/j.jaad.2015.06.053.
- Desai N, Shah P. High burden of hospital resource utilization in patients with hidradenitis suppurativa in England: a retrospective cohort study using hospital episode statistics. Br J Dermatol. 2017; 176(4): 1048-1055. doi: 10.1111/bjd.14976.
- Ortiz A, Grando SA. Smoking and the skin. Int J Dermatol. 2012; 51(3): 250-62. doi: 10.1111/j.1365-4632.2011.05205.x.
- Schane RE, Ling PM, Glantz SA. Health effects of light and intermittent smoking: A review. Circulation. 2010; 121(13): 1518-22. doi: 10.1161/CIRCULATIONAHA.109.904235.
- Huttunen R, Heikkinen T, Syrjänen J. Smoking and the outcome of infection. J Intern Med. 2011; 269(3): 258-69. doi: 10.1111/j.1365-2796.2010.02332.x.
- Langton AK, Sherratt MJ, Griffiths CE, Watson RE. A new wrinkle on old skin: the role of elastic fibres in skin ageing. Int J Cosmet Sci. 2010; 32(5): 330-9. doi: 10.1111/j.1468-2494.2010.00574.x.
- Metelitsa AI, Lauzon GJ. Tobacco and the skin. Clin Dermatol. 2010; 28(4): 384-90. doi: 10.1016/j.clindermatol.2010.03.021.
- Thomsen SF, Sørensen LT. Smoking and skin disease. Skin Therapy Lett. 2010; 15(6): 4-7.
- Bukvić Mokos Z, Miše J, Balić A, Marinović B. Understanding the Relationship Between Smoking and Hidradenitis Suppurativa. Acta Dermatovenerol Croat. 2020; 28(1): 9-13.
- Wu BB, Gu DZ, Yu JN, Feng LP, Xu R, et al. Relationship between Smoking and Pressure Injury Risk: A Systematic Review and MetaAnalysis. Wound Manag Prev. 2021; 67(9): 34-46.
- Droomers M, Schrijvers CT, Mackenbach JP. Why do lower educated people continue smoking? Explanations from the longitudinal GLOBE study. Health Psychol. 2002; 21(3): 263-72. doi: 10.1037//0278-6133.21.3.263.
- Hiscock R, Bauld L, Amos A, Fidler JA, Munafò M. Nível socioeconômico e tabagismo: Uma revisão. 2012; 1248: 107-23. DOI: 10.1111/j.1749-6632.2011.06202.x.
- Reid JL, Hammond D, Driezen P. Socio-economic status and smoking in Canada, 1999-2006: Has there been any progress on disparities in tobacco use? Can J Public Health. 2010; 101(1): 73-8. doi: 10.1007/BF03405567.
- De Azevedo Barros MB, Lima MG, Medina LP, Szwarcwald CL, Malta DC. Social inequalities in health behaviors among Brazilian adults: National Health Survey, 2013. Int J Equity Health. 2016; 15(1): 148. doi: 10.1186/s12939-016-0439-0.
- Szklo AS, Thrasher JF, Perez C, Figueiredo VC, Fong G, et al. Understanding the relationship between socioeconomic status, smoking cessation services provided by the health system and smoking cessation behavior in Brazil. Cad Saude Publica. 2013; 29(3): 485-95. doi: 10.1590/s0102-311x2013000300007.
- Giskes K, van Lenthe FJ, Turrell G, Brug J, Mackenbach JP. Smokers living in deprived areas are less likely to quit: A longitudinal followup. Tob Control. 2006; 15(6): 485-8. doi: 10.1136/tc.2006.015750.
- Kromann CB, Deckers IE, Esmann S, Boer J, Prens EP, et al. Risk factors, clinical course and long-term prognosis in hidradenitis suppurativa: A cross-sectional study. Br J Dermatol. 2014; 171(4): 819-24. doi: 10.1111/bjd.13090.
- Denny G, Anadkat MJ. The effect of smoking and age on the response to first-line therapy of hidradenitis suppurativa: An institutional retrospective cohort study. J Am Acad Dermatol. 2017; 76(1): 54-59. doi: 10.1016/j.jaad.2016.07.041.
- Parks RW, Parks TG. Pathogenesis, clinical features and management of hidradenitis suppurativa. Ann R Coll Surg Engl. 1997; 79(2): 83-9.
- Qiu F, Liang CL, Liu H, Zeng YQ, Hou S, et al. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget. 2017; 8(1): 268-284. doi: 10.18632/oncotarget.13613.
- Hirt PA, Castillo DE, Yosipovitch G, Keri JE. Skin changes in the obese patient. J Am Acad Dermatol. 2019; 81(5): 1037-1057. doi: 10.1016/j.jaad.2018.12.070.
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014 Aug 30; 384(9945): 766-81. doi: 10.1016/S0140-6736(14)60460-8.
- Jaacks LM, Vandevijvere S, Pan A, McGowan CJ, Wallace C, et al. The obesity transition: Stages of the global epidemic. Lancet Diabetes Endocrinol. 2019; 7(3): 231-240. doi: 10.1016/S2213-8587(19)30026-9.
- Yosipovitch G, DeVore A, Dawn A. Obesity and the skin: Skin physiology and skin manifestations of obesity. J Am Acad Dermatol. 2007; 56(6): 917-20. doi: 10.1016/j.jaad.2006.12.004.
- Tremmel M, Gerdtham UG, Nilsson PM, Saha S. Economic Burden of Obesity: A Systematic Literature Review. Int J Environ Res Public Health. 2017; 14(4): 435. doi: 10.3390/ijerph14040435.
- Darlenski R, Mihaylova V, Handjieva-Darlenska T. The Link Between Obesity and the Skin. Front Nutr. 2022; 9: 855573. doi: 10.3389/fnut.2022.855573.
- Wenczl E. A túlsúly és az elhízás bortünetei, kezelés, rehabilitáció [Skin manifestations, treatment and rehabilitation in overweight and obesity]. Orv Hetil. 2009; 150(37): 1731-8. Hungarian. doi: 10.1556/OH.2009.28693.
- Saalbach A. Association of Nutrition, Obesity and Skin. Nutrients. 2023; 15(9): 2028. doi: 10.3390/nu15092028.
- Ballard K, Shuman VL. Hidradenitis Suppurativa. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2023.
- Stunkard AJ. Socioeconomic status and obesity. Ciba Found Symp. 1996; 201: 188-93.
- Vazquez CE, Cubbin C. Socioeconomic Status and Childhood Obesity: a Review of Literature from the Past Decade to Inform Intervention Research. Curr Obes Rep. 2020; 9(4): 562-570. doi: 10.1007/s13679-020-00400-2.
- Drewnowski A, Specter SE. Poverty and obesity: the role of energy density and energy costs. Am J Clin Nutr. 2004; 79(1): 6-16. doi: 10.1093/ajcn/79.1.6.
- Dastgiri S, Mahdavi R, TuTunchi H, Faramarzi E. Prevalence of obesity, food choices and socio-economic status: a cross-sectional study in the north-west of Iran. Public Health Nutr. 2006; 9(8): 996-1000. doi: 10.1017/s1368980006009827.
- Drewnowski A, Moudon AV, Jiao J, Aggarwal A, Charreire H, et al. Food environment and socioeconomic status influence obesity rates in Seattle and in Paris. Int J Obes (Lond). 2014; 38(2): 306-14. doi: 10.1038/ijo.2013.97.
- Condamina M, Penso L, Tran VT, Hotz C, Guillem P, et al. Baseline Characteristics of a National French E-Cohort of Hidradenitis Suppurativa in ComPaRe and Comparison with Other Large Hidradenitis Suppurativa Cohorts. Dermatology. 2021; 237(5): 748-758. doi: 10.1159/000513447.
- Seyed Jafari SM, Knüsel E, Cazzaniga S, Hunger RE. A Retrospective Cohort Study on Patients with Hidradenitis Suppurativa. Dermatology. 2018; 234(1-2): 71-78. doi: 10.1159/000488344.
- Peterson GC, Preston A, Frieder J, Wang X, Paek SY. Analysis of Characteristics and Trends in Treatment Response of Hidradenitis Suppurativa Patients: A Southern US Cohort Study. Dermatology. 2020; 236(5): 413-420. doi: 10.1159/000504843.
- König A, Lehmann C, Rompel R, Happle R. Cigarette smoking as a triggering factor of hidradenitis suppurativa. Dermatology. 1999; 198(3): 261-4. doi: 10.1159/000018126.
- Arnson Y, Shoenfeld Y, Amital H. Effects of tobacco smoke on immunity, inflammation and autoimmunity. J Autoimmun. 2010; 34(3): J258-65. doi: 10.1016/j.jaut.2009.12.003.
- Ferrara F, Prieux R, Woodby B, Valacchi G. Inflammasome Activation in Pollution-Induced Skin Conditions. Plast Reconstr Surg. 2021; 147(1S-2): 15S-24S. doi: 10.1097/PRS.0000000000007617.
- Abolhasani R, Araghi F, Tabary M, Aryannejad A, Mashinchi B, et al. The impact of air pollution on skin and related disorders: A comprehensive review. Dermatol Ther. 2021; 34(2): e14840. doi: 10.1111/dth.14840.
- Kimball AB, Sundaram M, Gauthier G, Guérin A, Pivneva I, Singh R, Ganguli A. The Comorbidity Burden of Hidradenitis Suppurativa in the United States: A Claims Data Analysis. Dermatol Ther (Heidelb). 2018; 8(4): 557-569. doi: 10.1007/s13555-018-0264-z.
- Garg A, Hundal J, Strunk A. Overall and Subgroup Prevalence of Crohn Disease Among Patients With Hidradenitis Suppurativa: A Population-Based Analysis in the United States. JAMA Dermatol. 2018; 154(7): 814-818. doi: 10.1001/jamadermatol.2018.0878.
- Egeberg A, Jemec GBE, Kimball AB, Bachelez H, Gislason GH, et al. Prevalence and Risk of Inflammatory Bowel Disease in Patients with Hidradenitis Suppurativa. J Invest Dermatol. 2017; 137(5): 1060-1064. doi: 10.1016/j.jid.2016.11.040.
- Yadav S, Singh S, Edakkanambeth Varayil J, Harmsen WS, Zinsmeister AR, et al. Hidradenitis Suppurativa in Patients With Inflammatory Bowel Disease: A Population-Based Cohort Study in Olmsted County, Minnesota. Clin Gastroenterol Hepatol. 2016; 14(1): 65-70. doi: 10.1016/j.cgh.2015.04.173.
- Richette P, Molto A, Viguier M, Dawidowicz K, Hayem G, et al. Hidradenitis suppurativa associated with spondyloarthritis -- results from a multicenter national prospective study. J Rheumatol. 2014; 41(3): 490-4. doi: 10.3899/jrheum.130977.
- Kjaersgaard Andersen R, Saunte SK, Jemec GBE, Saunte DM. Psoriasis as a comorbidity of hidradenitis suppurativa. Int J Dermatol. 2020; 59(2): 216-220. doi: 10.1111/ijd.14651.
- Thomi R, Cazzaniga S, Seyed Jafari SM, Schlapbach C, Hunger RE. Association of Hidradenitis Suppurativa With T Helper 1/T Helper 17 Phenotypes: A Semantic Map Analysis. JAMA Dermatol. 2018; 154(5): 592-595. doi: 10.1001/jamadermatol.2018.0141.
- Pinter A, Kokolakis G, Rech J, Biermann MHC, Häberle BM, et al. Hidradenitis Suppurativa and Concurrent Psoriasis: Comparison of Epidemiology, Comorbidity Profiles, and Risk Factors. Dermatol Ther (Heidelb). 2020; 10(4): 721-734. doi: 10.1007/s13555-020-00401-y.
- Gau SY, Preclaro IAC, Wei JC, Lee CY, Kuan YH, et al. Risk of psoriasis in people with hidradenitis suppurativa: A systematic review and meta-analysis. Front Immunol. 2022; 13: 1033844. doi: 10.3389/fimmu.2022.1033844.
- Kridin K, Shani M, Schonmann Y, Fisher S, Shalom G, et al. Psoriasis and hidradenitis suppurativa: A large-scale populationbased study. J Am Acad Dermatol. 2023; 88(5): e231-e236. doi: 10.1016/j.jaad.2018.11.036.
- Bhalla R, Sequeira W. Arthritis associated with hidradenitis suppurativa. Ann Rheum Dis. 1994; 53(1): 64-6. doi: 10.1136/ard.53.1.64.
- Schneeweiss MC, Kim SC, Schneeweiss S, Rosmarin D, Merola JF. Risk of Inflammatory Arthritis after a New Diagnosis of Hidradenitis Suppurativa. JAMA Dermatol. 2020; 156(3): 342-345. doi: 10.1001/jamadermatol.2019.4590.
- Kridin K, Shavit E, Damiani G, Cohen AD. Hidradenitis suppurativa and rheumatoid arthritis: evaluating the bidirectional association. Immunol Res. 2021; 69(6): 533-540. doi: 10.1007/s12026-021-09221-4.
- Almuhanna N, Finstad A, Alhusayen R. Association between Hidradenitis Suppurativa and Inflammatory Arthritis: A Systematic Review and Meta-Analysis. Dermatology. 2021; 237(5): 740-747. doi: 10.1159/000514582.
- Antonoplis S. Studying Socioeconomic Status: Conceptual Problems and an Alternative Path Forward. Perspect Psychol Sci. 2023; 18(2): 275-292. doi: 10.1177/17456916221093615.
- Bromberger JT, Schott LL, Matthews KA, Kravitz HM, Harlow SD, et al. Childhood socioeconomic circumstances and depressive symptom burden across 15 years of follow-up during midlife: Study of Women’s Health across the Nation (SWAN). Arch Womens Ment Health. 2017; 20(4): 495-504. doi: 10.1007/s00737-017-0747-4.
- Everson SA, Maty SC, Lynch JW, Kaplan GA. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res. 2002; 53(4): 891-5. doi: 10.1016/s0022-3999(02)00303-3.
- Rojas-García A, Ruiz-Perez I, Rodríguez-Barranco M, Gonçalves Bradley DC, Pastor-Moreno G, et al. Healthcare interventions for depression in low socioeconomic status populations: A systematic review and meta-analysis. Clin Psychol Rev. 2015; 38: 65-78. doi: 10.1016/j.cpr.2015.03.001.
- Falconnier L. Socioeconomic status in the treatment of depression. Am J Orthopsychiatry. 2009; 79(2): 148-58. doi: 10.1037/a0015469.
- Verbeek T, Bockting CLH, Beijers C, Meijer JL, van Pampus MG, et al. Low socioeconomic status increases effects of negative life events on antenatal anxiety and depression. Women Birth. 2019; 32(1): e138-e143. doi: 10.1016/j.wombi.2018.05.005.
- Lee GB, Kim HC, Jeon YJ, Jung SJ. Association between socioeconomic status and longitudinal sleep quality patterns mediated by depressive symptoms. Sleep. 2021; 44(8): zsab044. doi: 10.1093/sleep/zsab044.
- Ridley M, Rao G, Schilbach F, Patel V. Poverty, depression, and anxiety: Causal evidence and mechanisms. Science. 2020; 370(6522): eaay0214. doi: 10.1126/science.aay0214.
- Assari S. Family Socioeconomic Status and Exposure to Childhood Trauma: Racial Differences. Children (Basel). 2020; 7(6): 57. doi: 10.3390/children7060057.
- Peverill M, Dirks MA, Narvaja T, Herts KL, Comer JS, et al. Socioeconomic status and child psychopathology in the United States: A meta-analysis of population-based studies. Clin Psychol Rev. 2021; 83: 101933. doi: 10.1016/j.cpr.2020.101933.
- Houtepen LC, Heron J, Suderman MJ, Fraser A, Chittleborough CR, et al. Associations of adverse childhood experiences with educational attainment and adolescent health and the role of family and socioeconomic factors: A prospective cohort study in the UK. PLoS Med. 2020; 17(3): e1003031. doi: 10.1371/journal.pmed.1003031.
- Xue B, Xue Y, Dong F, Zheng X, Shi L, et al. The impact of socioeconomic status and sleep quality on the prevalence of multimorbidity in older adults. Frontiers in Public Health. 2022; 10: 959700.
- Vilsaint CL, NeMoyer A, Fillbrunn M, Sadikova E, Kessler RC, et al. Racial/ethnic differences in 12-month prevalence and persistence of mood, anxiety, and substance use disorders: Variation by nativity and socioeconomic status. Compr Psychiatry. 2019; 89: 52-60. doi: 10.1016/j.comppsych.2018.12.008.
- Muscatell KA. Socioeconomic influences on brain function: implications for health. Ann N Y Acad Sci. 2018; 1428(1): 14-32. doi: 10.1111/nyas.13862.
- Goodman E, Slap GB, Huang B. The public health impact of socioeconomic status on adolescent depression and obesity. Am J Public Health. 2003; 93(11): 1844-50. doi: 10.2105/ajph.93.11.1844.
- Gooderham M, Papp K. The psychosocial impact of hidradenitis suppurativa. J Am Acad Dermatol. 2015; 73(5 Suppl 1): S19-22. doi: 10.1016/j.jaad.2015.07.054.
- Matusiak Ł, Bieniek A, Szepietowski JC. Hidradenitis suppurativa markedly decreases quality of life and professional activity. Journal of the American Academy of Dermatology. 2010; 62(4): 706-708.
- Alavi A, Farzanfar D, Rogalska T, Lowes MA, Chavoshi S. Quality of life and sexual health in patients with hidradenitis suppurativa. Int J Womens Dermatol. 2018; 4(2): 74-79. doi: 10.1016/j.ijwd.2017.10.007.
- Esmann S, Jemec GB. Psychosocial impact of hidradenitis suppurativa: A qualitative study. Acta Derm Venereol. 2011; 91(3): 328-32. doi: 10.2340/00015555-1082.
- Orenstein LAV, Salame N, Siira MR, Urbanski M, Flowers NI, et al. Pain experiences among those living with hidradenitis suppurativa: A qualitative study. Br J Dermatol. 2023; 188(1): 41-51. doi: 10.1093/bjd/ljac018.
- Caccavale S, Tancredi V, Boccellino MP, Babino G, Fulgione E, et al. Hidradenitis Suppurativa Burdens on Mental Health: A Literature Review of Associated Psychiatric Disorders and Their Pathogenesis. Life (Basel). 2023; 13(1): 189. doi: 10.3390/life13010189.
- Keary E, Hevey D, Tobin AM. A qualitative analysis of psychological distress in hidradenitis suppurativa. Br J Dermatol. 2020; 182(2): 342-347. doi: 10.1111/bjd.18135.
- Krajewski PK, Matusiak Ł, Szepietowska M, Rymaszewska JE, Jemec GBE, et al. Hidradenitis Suppurativa Quality of Life (HiSQOL): creation and validation of the Polish language version. Postepy Dermatol Alergol. 2021; 38(6): 967-972. doi: 10.5114/ada.2020.97064.
- Wolk K, Join-Lambert O, Sabat R. Aetiology and pathogenesis of hidradenitis suppurativa. Br J Dermatol. 2020; 183(6): 999-1010. doi: 10.1111/bjd.19556.
- Nielsen RM, Lindsø Andersen P, Sigsgaard V, Theut Riis P, Jemec GB. Pain perception in patients with hidradenitis suppurativa. Br J Dermatol. 2020; 182(1): 166-174. doi: 10.1111/bjd.17935.
- Jalenques I, Ciortianu L, Pereira B, D’Incan M, Lauron S, et al. The prevalence and odds of anxiety and depression in children and adults with hidradenitis suppurativa: Systematic review and meta-analysis. J Am Acad Dermatol. 2020; 83(2): 542-553. doi: 10.1016/j.jaad.2020.03.041.
- Mavrogiorgou P, Juckel G, Reimelt A, Hessam S, Scholl L, et al. Psychiatrische Komorbidität bei Hidradenitis suppurativa/Acne inversa [Psychiatric comorbidities in hidradenitis suppurativa/acne inversa]. Hautarzt. 2021; 72(5): 426-434. German. doi: 10.1007/s00105-020-04742-9.
- Krajewski PK, Matusiak Ł, von Stebut E, Schultheis M, Kirschner U, et al. Quality-of-Life Impairment among Patients with Hidradenitis Suppurativa: A Cross-Sectional Study of 1795 Patients. Life (Basel). 2021; 11(1): 34. doi: 10.3390/life11010034.
- McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain. 2003; 106(1-2): 127-33. doi: 10.1016/s0304-3959(03)00301-4.
- Fabrazzo M, Cipolla S, Signoriello S, Camerlengo A, Calabrese G, et al. A systematic review on shared biological mechanisms of depression and anxiety in comorbidity with psoriasis, atopic dermatitis, and hidradenitis suppurativa. Eur Psychiatry. 2021 Nov 25; 64(1): e71. doi: 10.1192/j.eurpsy.2021.2249.
- Machado MO, Stergiopoulos V, Maes M, Kurdyak PA, Lin PY, et al. Depression and Anxiety in Adults With Hidradenitis Suppurativa: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019; 155(8): 939-945. doi: 10.1001/jamadermatol.2019.0759.
- Misitzis A, Goldust M, Jafferany M, Lotti T. Psychiatric comorbidities in patients with hidradenitis suppurativa. Dermatol Ther. 2020; 33(4): e13541. doi: 10.1111/dth.13541.
- Tzur Bitan D, Berzin D, Cohen A. Hidradenitis Suppurativa and Bipolar Disorders: A Population-Based Study. Dermatology. 2020; 236(4): 298-304. doi: 10.1159/000504535.
- Rymaszewska JE, Krajewski PK, Szczęch J, Szepietowski JC. Depression and anxiety in hidradenitis suppurativa patients: A crosssectional study among Polish patients. Postepy Dermatol Alergol. 2023; 40(1): 35-39. doi: 10.5114/ada.2022.119080.
- Wright S, Strunk A, Garg A. Prevalence of depression among children, adolescents, and adults with hidradenitis suppurativa. J Am Acad Dermatol. 2022; 86(1): 55-60. doi: 10.1016/j.jaad.2021.06.843.
- Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. 2005; 58(3): 175-89. doi: 10.1016/j.biopsych.2005.05.001.
- Shenefelt PD. Psychodermatological disorders: Recognition and treatment. Int J Dermatol. 2011; 50(11): 1309-1322. doi: 10.1111/j.1365-4632.2011.05096.x.
- Mavrogiorgou P, G Juckel. Dermatologische Erkrankungen und ihre Bedeutung für die Psychiatrie. Der Nervenarzt. 2016; 3(88): 254-267.
- Kieć-Swierczyńska M, Dudek B, Krecisz B, Swierczyńska-Machura D, Dudek W, et al. Rola czynników psychologicznych i zaburzeń psychicznych w chorobach skóry. The role of psychological factors and psychiatric disorders in skin diseases. Med Pr. 2006; 57(6): 551-5. Polish.
- Petri V. Dermatologia Prática. Guanabara Koogan. Rio de Janeiro, 1ª Ed. 2009.
- Gottlieb AB, Prussick L, Rothstein B, Joshipura D, Saraiya A, et al. Open-label, investigator-initiated, single-site exploratory trial evaluating secukinumab, an anti-interleukin-17A monoclonal antibody, for patients with moderate-to-severe hidradenitis suppurativa. Br J Dermatol. 2019; 181(3): 609-611. doi: 10.1111/bjd.17822.
- Montero-Vilchez T, Diaz-Calvillo P, Rodriguez-Pozo JA, Cuenca-Barrales C, Martinez-Lopez A, et al. The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021; 18(13): 6709. doi: 10.3390/ijerph18136709.
- Koumaki D, Rovithi E, Solia Apokidou E, Papadakis M, Katoulis A, et al. Cutaneous body image in patients with hidradenitis suppurativa: A hospital-based cross-sectional study. Sci Rep. 2023; 13(1): 7898. doi: 10.1038/s41598-023-35120-9.
- Krajewski PK, Matusiak Ł, von Stebut E, Schultheis M, Kirschner U, et al. Pain in Hidradenitis Suppurativa: A Cross-sectional Study of 1,795 Patients. Acta Derm Venereol. 2021; 101(1): adv00364. doi: 10.2340/00015555-3724.
- Gergely LH, Gáspár K, Brodszky V, Kinyó Á, Szegedi A, et al. Validity of EQ-5D-5L, Skindex-16, DLQI and DLQI-R in patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020; 34(11): 2584-2592. doi: 10.1111/jdv.16642.
- Włodarek K, Głowaczewska A, Matusiak Ł, Szepietowski JC. Psychosocial burden of Hidradenitis Suppurativa patients’ partners. J Eur Acad Dermatol Venereol. 2020; 34(8): 1822-1827. doi: 10.1111/jdv.16255.
- Ramos-Alejos-Pita C, Arias-Santiago S, Molina-Leyva A. Quality of Life in Cohabitants of Patients with Hidradenitis Suppurativa: A Cross-sectional Study. Int J Environ Res Public Health. 2020; 17(16): 6000. doi: 10.3390/ijerph17166000.
- McAndrew R, Lopes FCPS, Sebastian K, Diaz LZ. Quality of life in hidradenitis suppurativa: A cross-sectional study of a pediatric population. J Am Acad Dermatol. 2021; 84(3): 829-830. doi: 10.1016/j.jaad.2020.09.072.
- Cuenca-Barrales C, Montero-Vilchez T, Krajewski PK, Szepietowski JC, Matusiak L, et al. Sexual Dysfunction and Quality of Life in Patients with Hidradenitis Suppurativa and Their Partners. Int J Environ Res Public Health. 2022; 20(1): 389. doi: 10.3390/ijerph20010389.
- Romaní J, Vilarrasa E, Martorell A, Fuertes I, Ciudad C, et al. Ustekinumab with Intravenous Infusion: Results in Hidradenitis Suppurativa. Dermatology. 2020; 236(1): 21-24. doi: 10.1159/000501075.
- Blok JL, Li K, Brodmerkel C, Horvátovich P, Jonkman MF, et al. Ustekinumab in hidradenitis suppurativa: clinical results and a search for potential biomarkers in serum. Br J Dermatol. 2016; 174(4): 839-46. doi: 10.1111/bjd.14338.
- Muralidharan V, Pathmarajah P, Peterknecht E, Qazi E, Barlow R, et al. Real life data on the biopsychosocial effects of Adalimumab in the management of hidradenitis suppurativa: A multicenter cross sectional analysis and consideration of a multisystem monitoring approach to follow up. Dermatol Ther. 2021; 34(1): e14643. doi: 10.1111/dth.14643.
- Caposiena Caro RD, Cannizzaro MV, Tartaglia C, Bianchi L. Clinical response rate and flares of hidradenitis suppurativa in the treatment with adalimumab. Clin Exp Dermatol. 2020; 45(4): 438-444. doi: 10.1111/ced.14127.
- Marzano AV, Genovese G, Casazza G, Moltrasio C, Dapavo P, et al. Evidence for a ‘window of opportunity’ in hidradenitis suppurativa treated with adalimumab: a retrospective, real-life multicentre cohort study. Br J Dermatol. 2021; 184(1): 133-140. doi: 10.1111/bjd.18983.
- Marasca C, Annunziata MC, Villani A, Volpe S, Marasca D, et al. Adalimumab versus Rifampicin Plus Clindamycin for the Treatment of Moderate to Severe Hidradenitis Suppurativa: A Retrospective Study. J Drugs Dermatol. 2019; 18(5): 437-438.
- Fabbrocini G, Marasca C, Megna M, Peris K. HS Quality of Life Study Group. Age and gender influence on HIDRAdisk outcomes in adalimumab-treated hidradenitis suppurativa patients. J Eur Acad Dermatol Venereol. 2019; 33 Suppl 6: 25-27. doi: 10.1111/jdv.15821.
- Vossen ARJV, van Doorn MBA, van der Zee HH, Prens EP. Apremilast for moderate hidradenitis suppurativa: Results of a randomized controlled trial. J Am Acad Dermatol. 2019; 80(1): 80-88. doi: 10.1016/j.jaad.2018.06.046.
- Kerdel FR, Azevedo FA, Kerdel Don C, Don FA, Fabbrocini G, et al. Apremilast for the Treatment of Mild-to-Moderate Hidradenitis Suppurativa in a Prospective, Open-Label, Phase 2 Study. J Drugs Dermatol. 2019; 18(2): 170-176.
- Caposiena Caro RD, Molinelli E, Brisigotti V, Offidani A, Bianchi L. et al. Clindamycin plus rifampicin in hidradenitis suppurativa treatment: Clinical and ultrasonography evaluation. Clin Exp Dermatol. 2021; 46(1): 96-102. doi: 10.1111/ced.14388.
- Caposiena Caro RD, Cannizzaro MV, Botti E, Di Raimondo C, Di Matteo E, et al. Clindamycin versus clindamycin plus rifampicin in hidradenitis suppurativa treatment: Clinical and ultrasound observations. J Am Acad Dermatol. 2019; 80(5): 1314-1321. doi: 10.1016/j.jaad.2018.11.035.
- Wilden S, Friis M, Tuettenberg A, Staubach-Renz P, Wegner J, et al. Combined treatment of hidradenitis suppurativa with intense pulsed light (IPL) and radiofrequency (RF). J Dermatolog Treat. 2021; 32(5): 530-537. doi: 10.1080/09546634.2019.1677842.
- Grimstad Ø, Kvammen BØ, Swartling C. Botulinum Toxin Type B for Hidradenitis Suppurativa: A Randomised, Double-Blind, PlaceboControlled Pilot Study. Am J Clin Dermatol. 2020; 21(5): 741-748. doi: 10.1007/s40257-020-00537-9.
- Fania L, Clemente A, Sampogna F, Mazzanti C, Pallotta S, et al. Intralesional ultrasound-guided combined treatment with triamcinolone plus lincomycin in hidradenitis suppurativa: A pilot study. Dermatol Ther. 2020; 33(6): e13901. doi: 10.1111/dth.13901.
- Grimstad Ø, Tzellos T, Dufour DN, Bremnes Ø, Skoie IM, et al. Evaluation of medical and surgical treatments for hidradenitis suppurativa using real-life data from the Scandinavian registry (HISREG). J Eur Acad Dermatol Venereol. 2019; 33(6): 1164-1171. doi: 10.1111/jdv.15353.
- Gibrila J, Chaput B, Boissière F, Atlan M, Fluieraru S, et al. Traitement radical de la maladie de Verneuil : comparaison de l’utilisation du derme artificiel et des lambeaux perforants pédiculés. Radical treatment of hidradenitis suppurativa: Comparison of the use of the artificial dermis and pedicled perforator flaps. Ann Chir Plast Esthet. 2019; 64(3): 224-236. French. doi: 10.1016/j.anplas.2018.06.013.
- Marchesi A, Amendola F, Garieri P, Steinberger Z, Vaienti L. Wide Local Excisions and Pedicled Perforator Flaps in Hidradenitis Suppurativa: A Study of Quality of Life. Ann Plast Surg. 2021; 86(2): 201-205. doi: 10.1097/SAP.0000000000002482.
- Prens LM, Huizinga J, Janse IC, Horváth B. Surgical outcomes and the impact of major surgery on quality of life, activity impairment and sexual health in hidradenitis suppurativa patients: a prospective single centre study. J Eur Acad Dermatol Venereol. 2019; 33(10): 1941-1946. doi: 10.1111/jdv.15706.
- Guart JA, Byers VV, Sasson DC, Bassiri-Tehrani B, Ranzer M, et al. Postoperative Quality of Life in Patients with Hidradenitis Suppurativa Utilizing the Hidradenitis Suppurativa Burden of Disease Tool. Cureus. 2021; 13(2): e13172. doi: 10.7759/cureus.13172.
- Vaillant C, Berkane Y, Lupon E, Atlan M, Rousseau P, et al. Outcomes and Reliability of Perforator Flaps in the Reconstruction of Hidradenitis Suppurativa Defects: A Systemic Review and Meta-Analysis. J Clin Med. 2022; 11(19): 5813. doi: 10.3390/jcm11195813.
- Gierek M, Kitala D, Łabuś W, Szyluk K, Niemiec P, et al. Impact of Hidradenitis Suppurativa Surgical Treatment on Health-Related Life Quality. J Clin Med. 2022; 11(15): 4327. doi: 10.3390/jcm11154327.
- Šitum M, Kolić M, Buljan M. PSYCHODERMATOLOGY. Acta Med Croatica. 2016; 70 Suppl 1: 35-8.