Introduction
Common Bile Duct Stones (CBDS) are relatively frequent disorders in clinical practice and can cause serious complications,
such as obstructive jaundice, acute suppurative cholangitis, and
acute pancreatitis, resulting in significant morbidity and mortality
if untreated. Endoscopic Retrograde Cholangiopancreatography
(ERCP) is a specialized endoscopic procedure for the management
of CBDS, and two main methods, Endoscopic Papillary Balloon Dilatation (EPBD) and Endoscopic Sphincterotomy (EST), are generally used for treatment [1]. Compared to transcystic common duct
stone removal and laparoscopic choledochotomy, ERCP has become the preferred method for the treatment of CBDS due to the
advantages of a simple surgery, reduced trauma, and a high success rate of stone removal [2]. However, ERCP also has procedurerelated complications, such as Postoperative Pancreatitis (PEP),
cholangitis, bleeding, perforation, and infection. Among these,
PEP is the most common and serious complication [3]. PEP is defined as an iatrogenic illness associated with at least a threefold
increase in serum amylase (or lipase) at 24 h, with intense pain
requiring extended hospitalization [4], which is a crucial factor in
morbidity and mortality. At present, there are contrasting reports
on the incidence of PEP, ranging from 3% to 15% [5,6]. Although its
determinants remain unclear, the development of PEP is thought
to be based on a pro-inflammatory cascade caused by pancreatic
acinar cell injury during endoscopic surgery, which induces systemic cytokine release. Understanding these mechanisms and the
identification of risk factors for PEP will help to adopt prophylactic
measures in high-risk patients and reduce morbidity.
The factors related to PEP occurrence identified in different
studies vary widely. In pancreaticobiliary diseases, risk factors for
developing PEP have been investigated in many studies for years
and the relevant factors from the mainstream view include young
age, female gender, history of pancreatitis, endoscopic sphincterotomy, papillary balloon dilatation, and pancreatic stent placement [7,8]. There is still controversy regarding some risk factors;
however, recent studies have shown that the risk factors for PEP
are affected by various factors, such as different regions, races,
and surgical purposes (such as the placement of pancreaticobiliary stents, temporary placement of nasobiliary duct drainage,
duodenal papilla or pancreaticobiliary duct biopsy, choledochoscopy, CBDS removal, etc.) [9,10]. The majority of the current literature reporting on the risk factors for PEP are based on studies
in Western countries, while relatively few reports have been published in Asia, particularly China. Prevention and reduction in the
occurrence of PEP has aroused increasing attention from endoscopists. Therefore, this study focused on the risk factors for PEP
after successful CBDS removal using ERCP in a Chinese population.
Materials and methods
Study population
The study was a single-center retrospective study performed
at First Affiliated Hospital of Nanjing Medical University in China
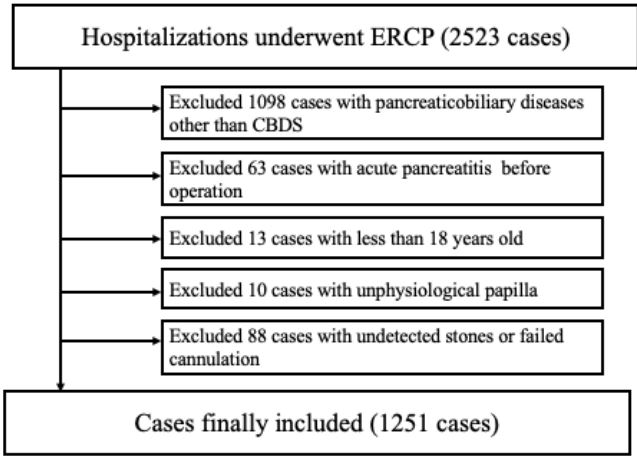
from January 2021 to December 2023. The study enrolled 1251
procedures applied on 1173 patients who had undergone endoscopic CBDS removal successfully by ERCP. The inclusion criteria
were as follows: (1) patients who had been diagnosed with CBDS
and received ERCP, (2) age over 18 years, (3) physiological papilla. The exclusion criteria were as follows: (1) acute pancreatitis within 2 weeks prior to ERCP, (2) 18 years of age, (3) undetected
CBDS during ERCP, (4) failed stone removal. The patient selection
process is shown in Figure 1. As a retrospective study, written informed consent is not required.
Data collection
Information on demographic and clinical variables of included patients was retrospectively extracted from medical records,
and the following data were included: sex, age, BMI, history of
smoking and drinking, history of hypertension, diabetes, atrial
fibrillation, coronary heart disease cerebral infarction, fatty liver
disease, history of surgical intervention, including liver transplantation and cholecystectomy, history of ERCP, acute pancreatitis
history, blood tests. ERCP method and findings was also collected,
including the size and number of stones, common bile duct stenosis, sphincterotomy, papillary balloon dilation and pancreatic duct
stent implantation.
Patients who present with two of the following three manifestations are diagnosed of acute pancreatitis [11]: (1) characteristic
upper abdominal pain (2) pancreatic enzyme values were greater
than three times the upper normal limit, or (3) findings of imaging examination suggesting acute pancreatitis. Pancreatic enzyme
tests were performed at 24 hours after the procedure.
Statistical analyses
Statistical analysis was performed using SPSS 26.0. To identify factors independently associated with the occurrence of PEP,
multivariate regression analysis was performed using significantly
associated factors identified in univariate analyses. A value of
p<0.05 was regarded as statistically significant.
Results
From January 2021 to December 2023, a total of 2523 hospitalizations underwent ERCP at First Affiliated Hospital of Nanjing Medical University was identified from discharge diagnosis.
Among them, 1,251 procedures were enrolled in our research.
The screening processes are shown in Figure 1.
Univariate analysis
Overall, PEP occurred in 84(6.71%) cases in the study population. We evaluated 32 variables, including 15 patient-related
factors, four stone-related indexes, three operation-related factors, and 10 blood tests. For patient-related factors, female gender (P=0.034, 95% CI: 1.047-3.257), cerebral infarction (P=0.005,
95% CI: 1.338-5.171), acute pancreatitis history (P=0.001, 95% CI:
2.522-8.507), fatty liver disease (P=0.027, 95% CI: 1.119-6.136)
were found to be associated with the increased risk of PEP by univariate analysis. Among stone-related indexes, diameter of common bile duct <10 mm (P=0.015, 95% CI: 1.175-4.341) was a risk
factor significantly associated with PEP. Among operation-related
risk factors, only EPBD was found to be a protective factor associated with PEP (P=0.003, 95% CI: 0.243-0.740) (Table 1).
Multivariate analysis
Those factors with a P value of less than 0.05 were included
in the multivariate logistic regression analysis. All factors were
determined to be relevant to PEP in multivariate analysis, including female gender (P=0.049, 95% CI: 1.002-2.521), cerebral infarction (P=0.011, 95% CI: 1.197-3.964), acute pancreatitis history (P=0.001, 95% CI: 2.436-7.249), fatty liver disease (P=0.021,
95% CI: 1.140-4.843), diameter of common bile duct <10 mm (P=
0.005, 95% CI: 1.299-4.313) EPBD (P=0.01, 95% CI: 0.321-0.855)
(Table 2).
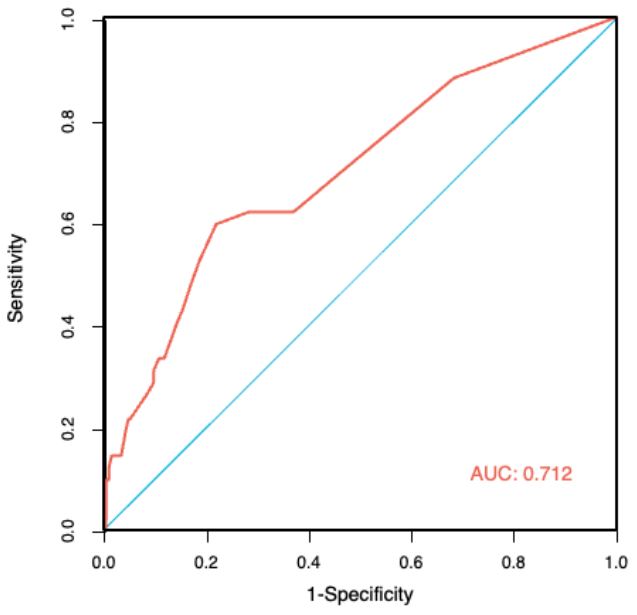
Multi-factor joint diagnosis of ROC curve
Six risk factors were considered to be relevant to PEP: Female
gender, cerebral infarction, acute pancreatitis history, fatty liver
disease, diameter of common bile duct <10 mm and EPBD. We
combined the PEP with 6 risk factors to draw the ROC curve. As
show in Figure 2, the AUC was 0.712 with a 95% CI of 0.651-0.773
(P<0.001) for joint factor. The predicting sensitivity, specificity, positive predictive value and negative predictive value were
59.5%, 78.1%, 16.3%, and 96.4% respectively.
Table 1: Univariate analysis of risk factors for PEP in CBDS patients.
|
P value |
OR (95% CI) |
| Basic characteristics |
|
|
| Age (>65y) |
0.102 |
1.520(0.921-2.510) |
| Female gender |
0.034 |
1.847(1.047-3.257) |
| BMI |
0.306 |
0.956(0.876-1.042) |
| Smoking |
0.535 |
1.263(0.604-2.643) |
| Drinking |
0.991 |
1.005(0.398-2.541) |
| Hypertension |
0.131 |
0.637(0.355-1.143) |
| Coronary heart disease |
0.892 |
0.945(0.418-2.138) |
| Cerebral infarction |
0.005 |
2.630(1.338-5.171) |
| Diabetes |
0.457 |
1.325(0.631-2.783) |
|
Acute pancreatitis history
|
0.001 |
4.631(2.522-8.507) |
| Atrial fibrillation |
0.172 |
2.033(0.735-5.625) |
| Fatty liver disease |
0.027 |
2.620(1.119-6.136) |
| Operation history |
|
|
| Liver transplantation |
0.886 |
0.892(0.189-4.222) |
| Cholecystectomy |
0.676 |
1.115(0.669-1.859) |
| History of ERCP |
0.339 |
1.362(0.722-2.570) |
| Disease-related factors |
|
|
| Number of Stones=1 |
0.431 |
0.791(0.442-1.416) |
|
Maximum Stone Diameter ≥10
mm
|
0.34 |
1.306(0.755-2.261) |
|
Diameter of Common Bile Duct
<10 mm
|
0.015 |
2.258(1.175-4.341) |
|
periampullary diverticula
|
0.087 |
0.555(0.283-1.090) |
|
Operation-related factors
|
|
|
| EST |
0.153 |
1.526(0.855-2.726) |
| EPBD |
0.003 |
0.424(0.243-0.740) |
| pancreatic duct stent |
0.252 |
1.560(0.718-3.547) |
|
Blood examination before
ERCP
|
|
|
|
Alanine aminotransferase
|
0.269 |
1.002(0.999-1.005) |
|
Aspartate aminotransferase
|
0.365 |
0.997(0.991-1.003) |
| Alkaline phosphatase |
0.176 |
0.998(0.995-1.001) |
| γ-glutamyl transferase |
0.325 |
0.999(0.998-1.001) |
| Serum total bilirubin |
0.561 |
1.009(0.979-1.039) |
| Conjugated bilirubin |
0.765 |
0.993(0.950-1.038) |
| Total cholesterol |
0.156 |
0.820(0.623-1.079) |
| Triglyceride |
0.148 |
0.729(0.474-1.119) |
| Fasting plasma glucose |
0.512 |
1.039(0.927-1.164) |
| Blood urea nitrogen |
0.426 |
0.955(0.852-1.070) |
| Serum creatinine |
0.932 |
1.000(0.994-1.007) |
| Serum uric acid |
0.726 |
1.001(0.998-1.003) |
Table 2: Multivariate analysis of risk factors for PEP in CBDS patients.
|
P value |
OR (95% CI) |
| Basic characteristics |
|
|
| Female gender |
0.049 |
1.589(1.002-2.521) |
| Cerebral infarction |
0.011 |
2.178(1.197-3.964) |
|
Acute pancreatitis history
|
0.001 |
4.201(2.436-7.249) |
| Fatty liver disease |
0.021 |
2.349(1.140-4.843) |
| Disease-related factors |
|
|
Diameter of Common
Bile
Duct <10 mm
|
0.005 |
2.367(1.299-4.313) |
|
Operation-related factors
|
|
|
| EPBD |
0.01 |
0.524(0.321-0.855) |
Discussion
Although the success rate of endoscopic treatment for
CBD stones using ERCP is improving, PEP remains a major concern. In this study, we evaluated the risk factors for PEP in patients with CBDS and found that female sex, history of FLD, cerebral infarction, previous acute pancreatitis, and common bile
duct stenosis significantly increased the risk of PEP, whereas EPBD
reduced this risk.
Although several studies have not found an association between sex and PEP, most have reported that women are more
prone to develop PEP [12], which could be attributed to the higher frequency of biliary stones and Sphincter of Oddi Dysfunction
(SOD) [13]. Consistent with the majority of previous studies, our
results also confirmed an increased incidence of PEP in female
patients compared to males.
The association between younger age and PEP remains controversial. Many reports have suggested that younger patients
have an increased risk of PEP [14,15]. The higher incidence of PEP
in younger patients has been explained by more active pancreatic exocrine function, smaller common bile duct diameter, and a
higher incidence of SOD. Unfortunately, there are no unified standards for the definition of younger age among studies, since cutoff values of 35, 50, and 60 years have all been used. Conversely,
a study involving 11,497 ERCP procedures grouped patients as 18-
50 years, 50-65 years, 65-80 years, and >80 years and showed that
younger age was insignificant in developing PEP [16]. This finding
was also confirmed by later studies [17]. Accordingly, age was not
an independent predictor of pancreatitis in our study of patients
with CBDS.
A large data analysis study by Reddy et al. revealed an association between NAFLD and acute pancreatitis [18]. In line with
this, a recent study by Sbeit et al. [19]. Showed that NAFLD is a
significant risk factor for PEP. A higher incidence of PEP in obese
patients has also been previously reported. Fujisawa et al. found
that the rate of PEP was significantly higher in obese patients than
in normal weight patients [20]. Kim et al. showed that obesity was
an important risk factor for moderately severe and severe PEP
[21]. Therefore, obese patients with high NAFLD rates may have
more severe PEP due to abnormal lipid metabolism. However,
high BMI was not a significant risk factor in our study, likely because we addressed this research among Asian populations who
tend to have a relatively low average BMI. Along with obesity, the effects of atherosclerosis on the rate and severity of pancreatitis have shown contradictory results. Atherosclerosis is a risk
factor for high-risk diseases, such as coronary heart disease and
cerebral infarction [22]. To the best of our knowledge, this is the
first study to define a history of cerebral infarction as a risk factor
for PEP in patients with CBDS. The exact mechanism by which a
history of cerebral infarction is a risk factor for PEP is unknown.
We believe that this may be associated with atherosclerosis, as
hyperlipidemia has been described as a significant contributor to
atherosclerosis and pancreatitis risk [23]. However, a retrospective study by Harsh et al. seems to disprove our conjecture; they
found a lower incidence of PEP in patients with a history of previous myocardial infarction [24]. However, in their analysis, patients
with acute coronary syndrome were advised to take antiplatelet
agents, such as aspirin, irrespective of the insertion of coronary
stents and history of PCI. In our study, the history of drug use was
not taken into account as we incorporated lacunar cerebral infarction indicated by radiological imaging, and some patients did not
take medication due to mild symptoms. This may partially explain
these differences. More research is required regarding cerebral
infarction to determine whether a history of drug use could affect
the outcome and prognosis of PEP.
A prior history of acute pancreatitis has been considered a
risk factor for PEP in many studies [25,26]. A higher risk of PEP
with previous acute pancreatitis was found to be associated with
a longer procedure time, which is associated with previous parenchymal pancreatic injury [25]. Similar to previous findings, a
history of acute pancreatitis was found to be a risk factor for PEP
after endoscopic removal of CBDS in our study. Therefore, it is our
recommendation that CBDS patients planning to undergo ERCP
must be informed about the high-risk of PEP as well as the additional methods to prevent PEP prior to surgery. Moreover, patients should be monitored for a longer duration before discharge
to minimize the risk of PEP.
It is not certain whether the common bile duct diameter affects PEP. Some studies have shown a higher PEP incidence in patients with narrow bile ducts [14], whereas others have shown
no difference in PEP in patients with different common bile duct
diameters [13,27]. Köseoğlu H et al. reported that common bile
duct stenosis is a risk factor for PEP only in patients with CBDS
[9]. Our data support the hypothesis that a smaller common bile
duct diameter is a risk factors for PEP after endoscopic removal
of CBDS.
EPBD is widely used because of its ease of operation and the
advantage of preserving the function of the Oddi sphincter compared to EST. In our study, contradictory to previous studies, EPBD
was found to be a protective factor against PEP. Makoto et al.
showed that EPBD for biliary stone removal is associated with a
greater risk of PEP, and suggested that EPBD should be avoided,
particularly in patients with CBDS [28]. They suggested that the
possible mechanism for this is papillary edema or spasm after
dilatation and damage to the pancreatic duct during papillary
dilatation. If so, placement of a prophylactic pancreatic duct stent
could prevent EPBD-related PEP. However, another study by Liao
indicated that insufficient dilatation of the papilla appears to be
one reason for the increased PEP rate in conventional EPBD [29].
Sufficient papillary dilation may be a protective factor against PEP.
Endoscopists in our hospital are experienced and have a longer duration of EPBD with large papillary dilation (diameter ≥1 cm),
which can partly explain the lower incidence of PEP in our study.
Moreover, a meta-analysis reported that the EPBD procedure increased the PEP rate only in Western patients, not in Asian patients, which could be due to the different sensitivities of EPBDrelated PEP in different ethnic groups [30]
We established a practical nomogram for predicting PEP. According to the ROC curve of the multivariate model, the AUC was
0.712 (95% CI: 0.651-0.773) and it could identify PEP occurrence
with an overall sensitivity of 59.5%, specificity of 78.1%, positive
predictive value of 16.3%, and negative predictive value of 96.4%.
The data revealed high sensitivity and negative predictive value
for PEP, which can be used to screen high-risk patients with PEP.
This study had several limitations. First, it was a single-center
retrospective study with a limited sample size, and further prospective studies are required to validate the results. Second, several other factors could also affect the risk of PEP, such as the frequency of intraoperative intubation, the amount and frequency
of contrast agent injection, the number of times the guidewire enters the pancreatic duct, and the total operation time of ERCP. In
future, the impact of new lithotripsy techniques, such as choledochoscopy, on PEP should also be considered. However, to the best
of our knowledge, this is the first study to report the risk factors
of PEP in Chinese patients with CBDS and demonstrated that female sex, a history of FLD, cerebral infarction, previous pancreatitis, and common bile duct stenosis are statistically significant risk
factors, while EPBD is a protective factor associated with PEP after
endoscopic removal of CBDS. These findings provide evidence for
future clinical decision-making.
Disclosure/conflict of interest: No conflicts of interest, financial or otherwise, are declared by the authors.
References
- Arvanitakis M, Devière J. Endoscopic retrograde cholangiopancreatography (ERCP). Endoscopy. 2009; 41: 890-894.
- Manes G, Paspatis G, Aabakken L, et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019; 51: 472-491.
- Trikudanathan G, Arain MA, Attam R, et al. Advances in the endoscopic management of common bile duct stones. Nat Rev Gastroenterol Hepatol. 2014; 11: 535-544.
- Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: An attempt at consensus. Gastrointest Endosc.1991; 37: 383-393.
- Kochar B, Akshintala VS, Afghani E, et al. Incidence, severity, and mortality of post-ERCP pancreatitis: A systematic review by using randomized, controlled trials. Gastrointest Endosc. 2015; 81: 143-149
- Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: A comprehensive review. Gastrointest Endosc. 2004; 59: 845-864.
- Elmunzer BJ. Reducing the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig Endosc. 2017; 29: 749-757.
- Ribeiro IB, do Monte Junior ES, Miranda Neto AA, et al. Pancreatitis after endoscopic retrograde cholangiopancreatography: A narrative review. World J Gastroenterol. 2021; 27: 2495-2506.
- Köseoğlu H, Solakoğlu T, Başaran M, et al. Risk factors for postERCP pancreatitis: It depends on the ERCP indication. Acta Gastroenterol Belg. 2020; 83: 598-602.
- Testoni PA. Why the incidence of post-ERCP pancreatitis varies considerably? Factors affecting the diagnosis and the incidence of this complication. Jop. 2002; 3: 195-201.
- Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis-2012: Revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62: 102-111.
- Ding X, Zhang F, Wang Y. Risk factors for post-ERCP pancreatitis: A systematic review and meta-analysis. Surgeon. 2015; 13: 218-229.
- Cheng CL, Sherman S, Watkins JL, et al. Risk factors for post-ERCP pancreatitis: A prospective multicenter study. Am J Gastroenterol. 2006; 101: 139-147.
- Wang P, Li ZS, Liu F, et al. Risk factors for ERCP-related complications: A prospective multicenter study. Am J Gastroenterol. 2009; 104: 31-40.
- Kakutani H, Hino S, Ikeda K, et al. Risk factors of post-ERCP pancreatitis at a tertiary referral center in Japan. Surg Laparosc Endosc Percutan Tech. 2014; 24: 270-273.
- Cotton PB, Garrow DA, Gallagher J, et al. Risk factors for complications after ERCP: A multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc. 2009; 70: 80-88.
- Ergin E, Oruç N, Ersöz G, et al. Prognosis and risk factors of ERCP pancreatitis in elderly. Sci Rep. 2021; 11: 15930.
- Reddy SK, Zhan M, Alexander HR, et al. Nonalcoholic fatty liver disease is associated with benign gastrointestinal disorders. World J Gastroenterol. 2013; 19: 8301-8311.
- Sbeit W, Khoury T, Wengrower D, et al. Nonalcoholic fatty liver disease and the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis: The hidden danger. Scand J Gastroenterol. 2021; 56: 369-373.
- Fujisawa T, Kagawa K, Hisatomi K, et al. Obesity with abundant subcutaneous adipose tissue increases the risk of post-ERCP pancreatitis. J Gastroenterol. 2016; 51: 931-938.
- Kim EJ, Cho JH, Oh KY, et al. The Risk Factors for Moderately Severe and Severe Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis According to the Revised Atlanta Classification.Pancreas. 2017; 46: 1208-1213.
- Wu Z, Wang X, Jiang X. Study on the Mechanism of Probucol Nanosuspension on Hyperlipidemic Pancreatitis and Regulation of Blood Lipid Function. J Nanosci Nanotechnol. 2021; 21: 1286-1292.
- Yang AL, McNabb-Baltar J. Hypertriglyceridemia and acute pancreatitis. Pancreatology. 2020; 20: 795-800.
- Patel HK, Desai R, Doshi S, et al. Endoscopic Retrograde Cholangiopancreatography in Patients With Versus Without Prior Myocardial Infarction or Coronary Revascularization: A Nationwide Cohort Study. Cureus. 2021; 13: e13921.
- Takenaka M, Fujita T, Sugiyama D, et al. What is the most adapted indication of prophylactic pancreatic duct stent within the highrisk group of post-endoscopic retrograde cholangiopancreatography pancreatitis? Using the propensity score analysis. J Hepatobiliary Pancreat Sci. 2014; 21: 275-280.
- Funatsu E, Masuda A, Takenaka M, et al. History of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis and Acute Pancreatitis as Risk Factors for Post-ERCP Pancreatitis. Kobe J Med Sci. 2017; 63: E1-e8.
- Park JS, Kim TN, Kim KH. Endoscopic papillary large balloon dilation for treatment of large bile duct stones does not increase the risk of post-procedure pancreatitis. Dig Dis Sci. 2014; 59: 3092-3098.
- Disario JA, Freeman ML, Bjorkman DJ, et al. Endoscopic balloon dilation compared with sphincterotomy for extraction of bile duct stones. Gastroenterology. 2004; 127: 1291-1299.
- Liao WC, Lee CT, Chang CY, et al. Randomized trial of 1-minute versus 5-minute endoscopic balloon dilation for extraction of bile duct stones. Gastrointest Endosc. 2010; 72: 1154-1162.
- Zhao HC, He L, Zhou DC, et al. Meta-analysis comparison of endoscopic papillary balloon dilatation and endoscopic sphincteropapillotomy. World J Gastroenterol. 2013; 19: 3883-3891.