Introduction
Transcanal Endoscopic Ear Surgery (TEES) is a mini-invasive
technique, used increasingly by otologists all over the world. More
and more studies have proved the feasibility of this approach for
many ear diseases including the cholesteatoma. The aim of this
clinical report is to describe the surgical steps for the management
of an attic cholesteatoma and the result for the patient.
Case presentation
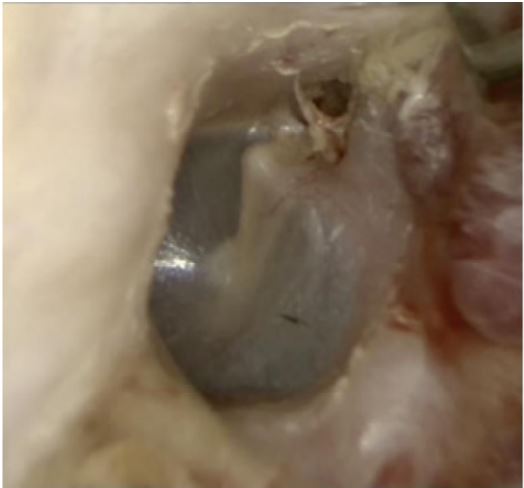
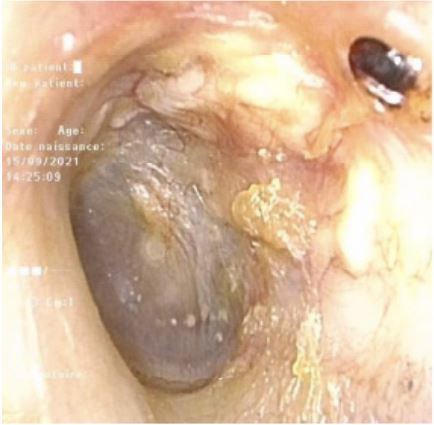
We report a case of a 46-year-old man, presenting left otorrhea
and a progressive hearing loss. An ear endoscopy showed an attic
cholesteatoma (Figure 1). An audiogram showed he had a mild
conductive hearing loss on medium and low frequencies. On the
CT scan the cholesteatoma occupied anterior, lateral and medial
attic, giving a lysis of the head of malleus and of the incus, no lysis
of the fallopian canal, of the tegmen tympani were observed. The
posterior extension of cholesteatoma was the aditus ad antrum
without passing the lateral semi-circular canal. So, there were no
radiological findings contraindicating a TEES. The patient accepted
to be operated by this mini-invasive approach. We used Storz
endoscopes of 0 and 45°, with 3 mm calibre and 14 cm length,
and a full HD video.
Surgical steps: Infiltration of the external auditory canal by
xylocaine and adrenaline 1% solution. A wide tympanomeatal
flap was incised from 9 to 7 o’clock, a certain distance from the
cholesteatoma. Cotonoid socked in adrenaline diluted with
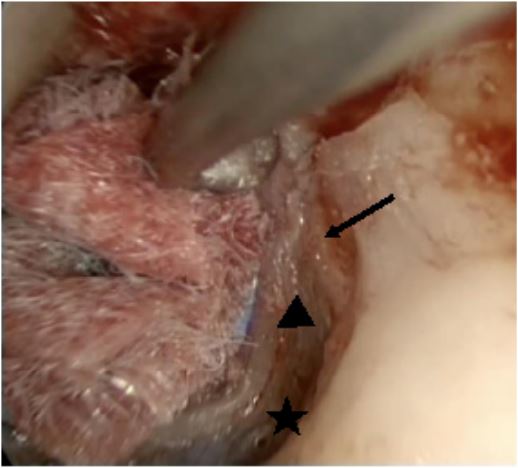
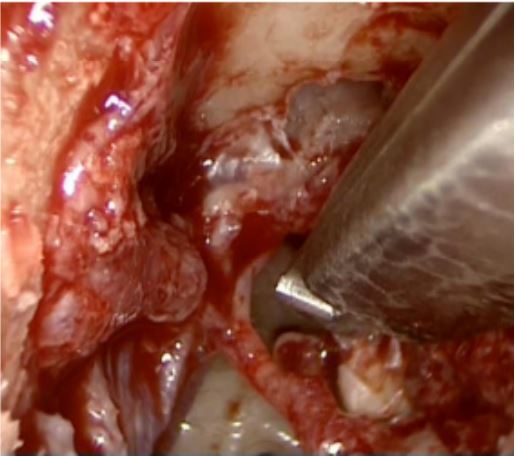
physiological solution was used to control the bleeding. The anulus
was elevated reaching the corda tympani and we accessed to the
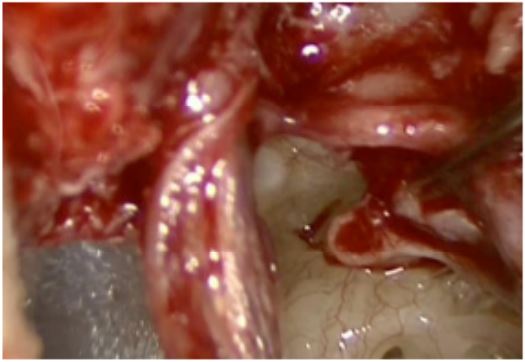
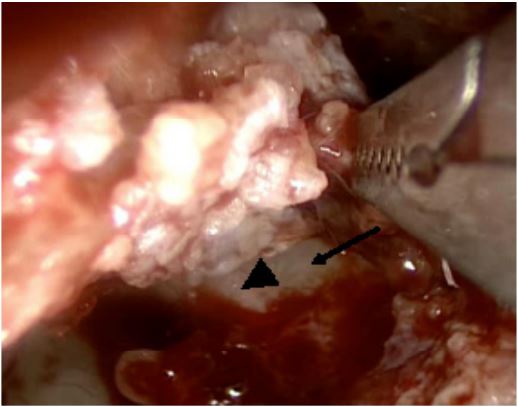
middle ear in its inferior part as shown in Figure 2. Cholesteatoma
was identified juste above the stapedius tendon (Figure 3) and
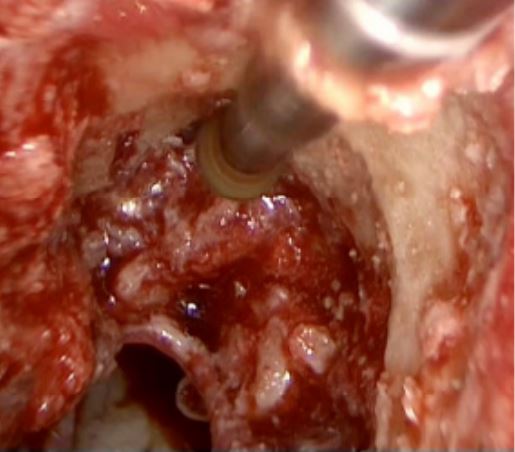
incudo-stapedial joint was disarticulated (Figure 4). The scutum
was enlarged by a curet and a 2 mm diamond burr to reach the
limits of the disease (Figure 5). The tympano-meatal flap was
protected by a silicon sheet. The head of malleus was cut (Figure
6) and the cholesteatoma was removed in one bloc including
incus and the head of the malleus (Figure 7). All the attic, sinus
tympani and aditus ad antrum were inspected minutely with a
45° endoscope, showing no residual disease. The atticotomy was
reconstructed by several slices of tragal cartilage. The last piece
of cartilage had its own perichondrium on the external surface.
Ossiculoplasty was performed with cartilage. The tympano-meatal
flap was replaced and an absorbable ear packing was applied. A
non-resorbable packing of the external auditory canal was added.
The non-resorbable and absorbable packing were removed at
one week and one month after surgery respectively in outpatient
service. The attic was correctly reconstructed by the cartilage
and perichondrium grafts. There was a conductive hearing loss
improvement on audiogram.
During follow up the ear drum was found to be stable and dry
as shown on Figure 8. The patient complained of a non-disabling
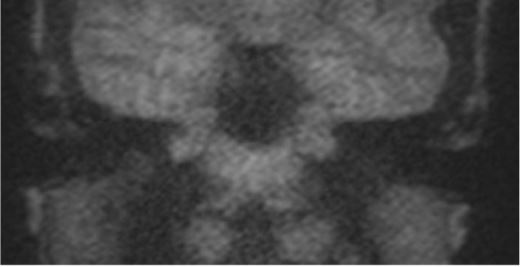
tinnitus only. CT scan at one year after surgery showed no
anomalies with a good aeration of the attic. A diffusion-weighted
MRI non-EPI showed no relapse of the cholesteatoma at 2 and 3
years after surgery (Figure 9).
Discussion
The role and the utility of the endoscopic ear surgery for management of cholesteatoma has been widely discussed over the
past twenty years. Tarabichi M showed in several studies that a
transcanal endoscopic approach gives a wide field of view despite
a transcanal approach under microscopic view [1]. El-Messelaty
et al. reported on the value of endoscopy as an adjunct in cholesteatoma surgery and documented a reduced risk of recurrence
when the endoscope was used [2]. The reduction in residual disease was further confirmed by Yung MW [3] and Ayache S [4].
Marchioni D and Presutti L described how opening the tensor fold
during endoscopic management of cholesteatoma allows a good
aeration of the attic [5].
According to the experience reported by all these authors, the
case reported here confirms that TEES for attic cholesteatoma is a
mini-invasive technique allowing good functional and anatomical
long-term results.
Conclusion
This case report showed that attic cholesteatoma can be totally managed by a transcanal endoscopic approach with very good
results, confirming that this technique is safe and advantageous
for our patients.
References
- Muaaz Tarabichi. Transcanal Endoscopic Management of Cholesteatoma. Otology & Neurotology. 2010; 31: 580-588.
- El-Meselaty K, Badr-El-Dine M, Mandour M, Mourad M, Darweesh
R. Endoscope affects decision making in cholesteatoma surgery.
Otolaryngol Head Neck Surg. 2003; 129: 490Y6.
- Yung MW. The use of middle ear endoscopy: has residual cholesteatoma been eliminated? J Laryngol Otol. 2001; 115: 958Y61.
- Ayache S, Tramier B, Strunski V. Otoendoscopy in cholesteatoma
surgery of the middle ear. What benefits can be expected? Otol
Neurotol. 2008; 29: 1085Y90.
- Marchioni D, Mattioli F, Ciufelli MA, Presutti L. Endoscopic approach to tensor fold in patients with attic cholesteatoma. Acta
Otolaryngol. 2008; 19: 1Y9.