Introduction
As breast-augmented women age, they will constitute a growing part of the patient population in future breast cancer cases.
For the time being, there is a lack of consensus regarding the
treatment of breast-augmented women diagnosed with breast
cancer. Non-augmented patients are preferably offered BreastConserving Therapy (BCT), which is associated with superior outcomes regarding recurrence and mortality when compared to
mastectomy [1], which is used in about 30% of cases, primarily in
large tumors and/or in small breasts [2]. BCT includes a lumpectomy followed by radiotherapy to the residual breast to reduce the
risk of recurrence. Irradiation is associated with potential side effects, including fibrosis, edema, dyspigmentation, telangiectasia,
and pain [3]. Currently, the literature provides limited and discordant data regarding BCT and radiotherapy in patients with breast
implants. While some studies report that the presence of breast
implants has little impact on fibrosis and cosmesis, other studies
have shown both high rates of capsular contracture (firm fibrous
tissue around the implant) as well as poor cosmetic results [4].
The primary aim of this study was to quantify the proportion
of breast-augmented women who after BCT and radiotherapy for
breast cancer had capsular contracture. Furthermore, we wished
to investigate overall cosmetic outcome and complications that
might affect both development of capsular contracture as well as
cosmesis following BCT.
Materials and methods
Patients and measures
After obtaining approval from the institutional board, all
breast-augmented women who underwent BCT and radiotherapy
at Herlev and Gentofte Hospital, Denmark, from 2018 until 2021
were identified in the patient administrative electronic system
based on radiation codes and radiotherapy planning CT scans
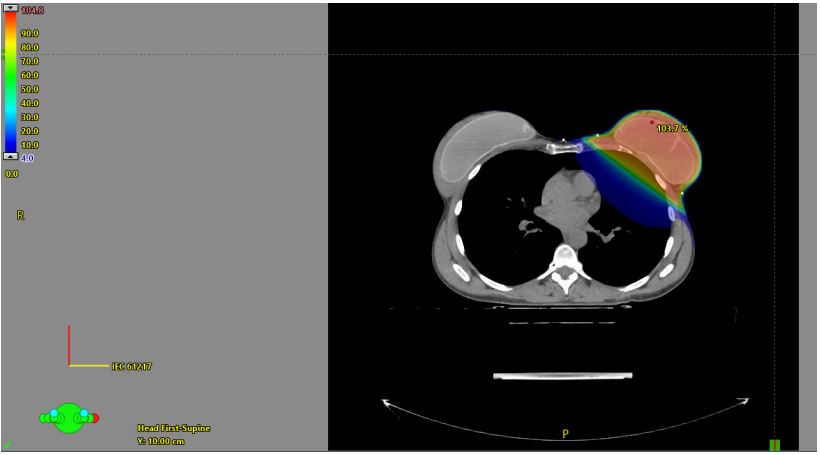
(Figure 1). Data regarding demographics, augmentation, breast
cancer and treatment characteristics, complications, oncological
and cosmetic outcome was extracted through review of electronic patient charts. Breast symmetry was recorded on a three-point
scale (good symmetry, some asymmetry, severe asymmetry) and
capsular contracture on a four-point scale (none, slight, moderate
and severe). Follow-up time was defined as the period from the
date of last radiation therapy until the last date of patient consultation with an oncologist or breast surgeon. Complications were
characterized as surgery-requiring or other complications. Time
from finalized radiation therapy until debut of a complication was
registered. Regarding cosmesis, four-graded scales used in several
radiotherapy protocols [5,6] were copied (Table 3). If no specific
rating of cosmetic appearance was described in medical records,
senior author (LH) assessed cosmesis based on post-operative
photos, if available.
Statistical analysis
We generated frequency analyses of complications, capsular
contractures, oncologic and cosmetic outcomes. No further analyses to explore potential associations could be performed, since
sample sizes were too small. Data analysis was conducted in IBM
SPSS® (IBM Corp. IBM SPSS Statistics for Windows, Version 25.0.
Armonk, NY: IBM Corp; 2017).
Results
Patients
2038 consecutive scans were evaluated, and a total of 30
(1.5%) breast-augmented women undergoing BCT with preservation of breast implants were identified. Median follow-up time
was 29 months (range 0-55 months). One patient with no followup consultations after radiotherapy had a mammography done
five months later, which described inconspicuous conditions surrounding the subpectoral implants. Patient and implant characteristics are summarized in Table 1. Median patient age at date
of surgery was 51 years (range 32-77 years). Median implant age
was 6 years (range 1-30 years). Most implants were placed subpectorally (87%). The different tumor and treatment characteristics can be seen in Table 2.
Complications and capsular contracture
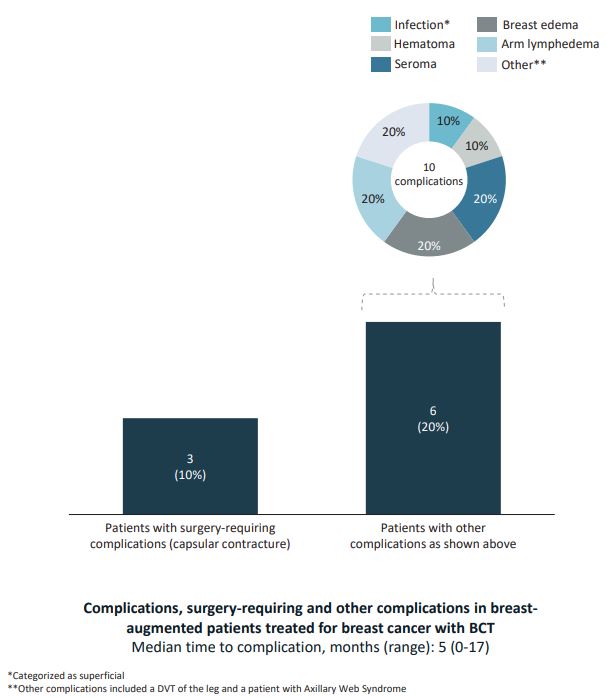
Complications were documented in nine patients (30%), three
of whom required additional surgical treatment due to capsular
contracture. In one case, the implant was removed, in two other
cases capsulotomy was performed and the implants were exchanged. The remaining six patients (20%) had complications that
did not require surgical intervention (Figure 2). Hematoma and
seroma was treated with percutaneous drainage. Patients with
lymphedemas were referred to physiotherapeutic treatment.
Follow-up and outcome data are shown in Table 3. Assessment of
capsular contracture following treatment was only documented
in six of the 30 patients (20%). Three patients (50%) were classified with no contracture and three (50%) with moderate to severe
capsular contracture. One had worsening of a preexisting moderate contracture to severe capsular contracture. The two others
developed moderate and severe contracture, respectively. Median time until patients were diagnosed with a new or worsening
capsular contracture was 12 months. Overall cosmetic appearance following BCT was rated in 11 patients (37%), of whom 63%
had good to excellent cosmetic outcome whereas 36% women
had fair to poor cosmetic outcome. There were no local recurrences during follow-up and all patients were alive at the end of
study.
Table 1: Patient and implant characteristics.
|
Age, years (MEDIAN, range)
|
51(32-77) |
|
BMI, kg/m2 (median, range)
|
21.4(17.9-27.6) |
|
Smoking status, n (%)
|
| Never |
18(60%) |
| Every day |
7(23%) |
| Sometimes |
- |
| Former smoker |
5(17%) |
|
Breast tissue Thickness
preoperatively, mm (median,
range)
|
15(8-36) |
|
Implant age, years (median,
range)
|
6(1-30) |
| Data missing, N |
7 |
|
Baseline capsular
contracture, n (%)
|
| None |
7(78%) |
| Slight |
1(11%) |
| Moderate |
1(11%) |
| Severe |
- |
| Data missing |
21 |
|
Implant shape, n (%)
|
| Round |
3(75%) |
| Anatomical |
1(25%) |
| Data missing |
26 |
|
Implant filling, n (%)
|
| Silicone |
30(100%) |
|
Incision for augmentation, n
(%)
|
| Inframammary |
8(62%) |
| Axillary |
1(8%) |
| Other* |
4(31%) |
| Data missing |
17 |
|
Implant position, n (%)
|
| SubGlandular |
4(13%) |
| Subpectoral |
26(87%) |
*Other incisions included one wise pattern and three patients with
medical charts describing scars following mastopexy.
Table 2: Tumor and treatment characteristics.
|
Tumor localization, n (%)
|
|
| Lower medial quadrant |
- |
| Upper Medial quadrant |
8(27%) |
| Lower Lateral quadrant |
3(10%) |
| Upper Lateral quadrant |
9(30%) |
| Central |
3(10%) |
| Other* |
7(23%) |
|
Tumor histology, n (%)**
|
|
| DCIS |
4(12%) |
| INvasive ductal |
24(73%) |
| Invasive lobular |
3(9%) |
| Other*** |
2(6%) |
|
Tumor size, mm (median,
range)
|
11(2-23) |
|
Nearest resection margin, n
(%)
|
|
|
Negative margin (≥ 2 mm)
|
28(93%) |
|
Positive margin (< 2 mm)
|
2(7%) |
| Reexcision, n (%) |
2(7%) |
| ER expression, n (%) |
|
| Positive |
25(89%) |
| Negative |
3(11%) |
| HER2 expression, n (%) |
|
| Normal expression |
27(96%) |
| Overexpression |
1(4%) |
| Ki67 index, n (%) |
|
| ≤10 % |
16(57%) |
| >10% |
12(43%) |
|
Sentinel node status, n (%)
|
|
| No metastasis |
19(63%) |
| Macrometastasis |
5(17%) |
| Micrometastasis |
3(10%) |
|
Single cell infiltration
|
2(7%) |
| SN not performed |
1(3%) |
|
Subsequent axillary surgery,
n (%)
|
2(7%) |
| Chemotherapy, n (%) |
|
| Before surgery |
1(3%) |
| After surgery |
11(37%) |
| None |
18(60%) |
|
Antihormonal treatment, n
(%)
|
|
| Tamoxifen |
12(40%) |
| Aromatase inhibitor |
11(37%) |
| None |
7(23%) |
|
Biological treatment, n (%)
|
|
| Traztuzumab |
1(3%) |
| None |
29(97%) |
|
Radiation technique, n (%)
|
|
| WBI**** + boost |
14(47%) |
| WBI |
14(47%) |
| PBI***** |
2(7%) |
*Other tumor localization included tumors localized on the border
of two quadrants: four tumors at 12 o’clock and the three remaining at
three, six and nine o’clock, respectively., **One patient can contribute
with >1 tumor. ***Other tumors included a tubular carcinoma and Pag-
ets of the nipple. ****WBI = Whole breast irradiation. *****PBI = Partial
breast irradiation.
Table 3: Follow-up and outcome.
|
Follow-up, months (MEDIAN,
range)
|
29(0-55) |
| Pain (breast), n (%) |
10(33%) |
| Data missing |
20 |
|
Fibrosis (breast), n (%)
|
|
| None |
5(63%) |
| Slightly palpable |
3(38%) |
| Palpable |
- |
|
Clearly palpable, retraction
of skin and fixation
|
- |
| Data missing |
22 |
|
Capsular contracture after
BCT, n (%)
|
|
| None |
3(50%) |
| Slight |
- |
| Moderate |
1(17%) |
| Severe |
2(33%) |
| Data missing |
24 |
|
Time to capsular
contracture, months (median,
range)
|
12(10-12) |
|
Breast symmetry after BCT, n
(%)
|
|
| Good symmetry |
5(56%) |
| Some asymmetry |
4(44%) |
| Severe asymmetry |
- |
| Data missing |
21 |
| Dyspigmentation, n (%) |
|
| No difference |
2(29%) |
| Slight difference |
4(57%) |
| Moderate difference |
1(14%) |
| Dramatic difference |
- |
| Data missing |
23 |
|
Cosmetic appearance, n (%)
|
|
| Excellent |
2(18%) |
| Good |
5(45%) |
| Fair |
3(27%) |
| Poor |
1(9%) |
| Data missing |
19 |
| Local recurrence, n (%) |
None |
Discussion
Only a very small group of women with cosmetic breast implants underwent BCT including radiotherapy in our cohort of
women treated with BCT including radiotherapy in the period
2018-2021. Complications were minor and only 10 percent were
operated for capsular contracture within a follow-up time of a
little more than 2 years as a median.
Capsular contracture
Our group has in 2020 published a systematic review on the
literature based on 17 articles on capsular contracture after BCT
and radiotherapy in breast-augmented women [4], and found a
capsular contracture rate of 22.2% following BCT with reported
rates ranging from 0% to 65% [7-10]. Two more recent studies
also evaluated rates of capsular contracture among breast-augmented breast cancer patients undergoing BCT including radiotherapy. A French study of 50 patients by Lesniak et al. [11] found
34% with capsular contracture within a follow-up time of median
51 months, and a US study of 70 patients by Tadros et al. [12] had a capsular contracture rate of 25.4% observed within 1.9 years.
Our contracture rate is comparable to those of previous studies: 50% of the patients with available information had capsular
contracture at follow-up, and median time until diagnosis of a new
or worsening of contracture was reported in the medical records
was 12 months. Although only six patients had available data on
capsular contracture assessment, we assume the remaining 24
patients did not have contracture to a degree that made them
express concerns or dissatisfactions at follow-up consultations
nor prompted a physician to refer them to surgical revision. The
health care is tax funded and free, and patients with severe symptoms can be expected to be referred. This assumption results in
a proportion of capsular contracture of 3/30 (10%). The true proportion of women with significant capsular contracture, based on
our material, is therefore likely in between 10% and 50%.
Complications rates
Serritzlev et al. found that 30.6% of patients undergoing BCT
developed complications and 17.1% required reoperations due to
complications. In the study by Tadros et al., 12.7% were referred
for revisional surgery. Our study shows a similar complication rate
of 30%. Ten percent of the patients had complications requiring
revisional surgery all due to capsular contracture, and all requiring
implant removal or exchange, and 20% had complications that did
not require surgical intervention. In contrast, Lesniak et al. had no
patients requiring reoperations or explantation of implants due to
early complications.
Cancer control
Our study supports previous findings [10,11,13,14] that good
tumor control can be obtained with BCT in previously breast-augmented women. Two patients (7%) had positive resection margins
and needed subsequent re-excision, and there were no local recurrences. As reference, the overall local recurrence rate within
five years following BCT is 2.4% in Denmark [15].
Prabhakaran et al. investigated tumor margins, re-excision
rates and recurrence in previously breast-augmented women
(n=52) versus non-augmented women (n=51) who underwent
breast-conserving therapy. In the augmented group 11.5% had
positive margins, 21.2% underwent re-excision and 7.7% had recurrence within a follow-up time of median 100.3 months. They
found no statistical difference between the two groups, which led
them to conclude that BCT in augmented breast cancer patients is
safe and feasible, from an oncological standpoint.
In Denmark, the surgical standard care for early-stage breast
cancer is BCT if feasible, because the breast is preserved, and superior survival compared with mastectomy has been found [1].
This also applies to breast-augmented women, however, in some
cases, the tumor/breast tissue ratio does not allow for this solution, and skin or nipple-sparing mastectomy and primary reconstruction is then generally recommended, or a mastectomy “on
top of the implant” may yield a satisfactory cosmetic result. The
distribution of the different surgical solutions is not known.
Overall cosmetic outcome
Even though information on overall cosmetic outcome was
only accessible in 11 patients, our results seem comparable to findings of previous studies. Sixty-three percent of our patients
with available information were rated as having an excellent to
good overall cosmetic appearance following BCT, which is very
similar to the 67.6% and 68% previously reported [4,11]. However, our information was mainly based on information retained
at one-year follow-up consultations with a breast surgeon and implant-related information was limited. Afterwards, patients were
primarily followed by oncologists who did not report further on
cosmesis of the breast.
Complications and cosmetic outcome of BCT in non-augmented women
In a randomized Phase III Trial, the Danish Breast Cancer Group
compared hypofractionated radiotherapy to standard fractionated therapy in 1854 patients following breast-conserving surgery
[16]. Registered complications included induration (considered a
marker for fibrosis), edema and pain as well as overall cosmetic
outcome at three- and five-year follow-ups. Induration was reported in 9% of the patients receiving hypofractionated radiotherapy after 5 years, 1% had edema and 4% experienced pain.
A good to excellent cosmetic outcome was reported in 80% of
the patients. No overall complication rate was specified. Although
comparison to our study is impaired by our small sample sizes, it
seems that non-augmented women have lower rates of complications and better cosmetic outcome following BCT.
Limitations
Our study is limited by the retrospective design, sparse amount
of data in medical records, the small sample size of patients and
a relatively short follow-up period. The lack of data on capsular
contracture assessment and cosmetic outcome makes conclusions less valid. However, we do assume unacceptable levels of
contracture and poor cosmetic results would have been mentioned in medical records or led a clinician to respond with a referral to evaluation by a breast- or plastic surgeon. Despite our small
sample size, we did observe distributions of overall complication
rates and cosmetic outcomes which seem similar to findings in
other studies. The lack of longer follow-up time might influence
the rate of capsular contracture and other complications, since
contracture is known to develop over years [17]. Another limitation is our study’s susceptibility to the risk of selection bias since
the distribution of augmented breast cancer patients between
BCT and mastectomy is unknown. Patients are selected for either
BCT or mastectomy based on patient and cancer characteristics.
This might have resulted in most of the complicated cases being
selected for mastectomy and perhaps primary breast reconstruction rather than lumpectomy. Among strengths are the thorough
evaluation of a consecutive cohort of breast cancer patients to
identify the study group, and since our hospital was responsible
for the radiotherapy for approximately half of the women treated
in the Capital Region of Denmark, it does give valid information
about the small number of breast-augmented women who currently has received this treatment.
Further research in the form of a prospective study is needed
to determine whether BCT is the best treatment option for women with prior augmentation.
Conclusion
This study is merely a step towards better understanding the outcome of BCT in previously breast-augmented women. Our
results suggest that women with prior augmentation should be
informed of the risk of development or worsening of capsular
contracture and the potential impact on overall cosmetic appearance following breast-conserving surgery and radiation therapy.
Furthermore, our study emphasizes the importance of improved
documentation concerning implant- and breast-related factors in
breast cancer treatment of breast-augmented women.
Conflicts of interest: Senior author Lisbet Rosenkrantz Hölmich
has received a research grant from Johnson & Johnson/Mentor.
All other authors have no conflict of interest to declare.
References
- Christiansen P, Mele M, Bodilsen A, Rocco N, Zachariae R. BreastConserving Surgery or Mastectomy?: Impact on Survival. Annals of Surgery Open [Internet]. 2022;3(4). Available from: https://journals.lww.com/aosopen/Fulltext/2022/12000/Breast_Conserving_Surgery_or_Mastectomy___Impact.6.aspx
- DMCG. Kirurgisk behandling af brystkræft [Internet]. Available from: https://www.dmcg.dk/Kliniske-retningslinjer/kliniskeretningslinjer-opdelt-paa-dmcg/brystcancer/kirurgisk-behandlingaf-brystkraft/
- Oncology AS of C. Breast Cancer: Types of Treatment [Internet]. 2018. Available from: https://www.cancer.net/cancer-types/breast-cancer/types-treatment#radiation-therapy
- Serritzlev MS, Lorentzen AK, Matthiessen LW, Hölmich LR. Capsular contracture in patients with prior breast augmentation undergoing breast conserving therapy and irradiation. J Plast Surg Hand Surg. 2020/05/08. 2020;54(4):225–32.
- Danish Breast Cancer Group. DBCG Proton Trial Cosmetic form [Internet]. 2020. Available from: https://www.dbcg.dk/images/PDF/Skemaer/RT/PROTON/DBCG_PROTON_trial_Cosmetic_form_1.pdf
- Danish Breast Cancer Group. DBCG 2018 Natural Trial [Internet]. 2018. Available from: https://dbcg.dk/PDF%20Filer/DBCG_2018_RT_01.09.2018_EN_cosmeticAndFunction.pdf
- Handel N, Lewinsky B, Jensen JA, Silverstein MJ. Breast conservation therapy after augmentation mammaplasty: is it appropriate? Plast Reconstr Surg. 1996/12/01. 1996;98(7):1216–24.
- Lei RY, Leonard CE, Howell KT, Henkenberns PL, Johnson TK, Hobart TL, et al. External beam accelerated partial breast irradiation yields favorable outcomes in patients with prior breast augmentation. Front Oncol. 2014/07/06. 2014;4:154.
- Krishnan L, Krishnan EC, Wolf CD, Jewell WR. Preservation of augmented breasts in patients with breast cancer. Radiographics. 1993/07/01. 1993;13(4):831–9.
- Tuli R, Flynn RA, Brill KL, Sabol JL, Usuki KY, Rosenberg AL. Diagnosis, treatment, and management of breast cancer in previously augmented women. Breast J. 2006/07/20. 2006;12(4):343–8.
- Lesniak DM, Millochau J, Wang KC, Atlan M, Otmezguine Y, Sarfati I, et al. Breast-conserving therapy can be offered to women with prior breast augmentation. Eur J Surg Oncol. 2020/05/28. 2020;46(8):1456–62.
- Tadros AB, Moo TA, Zabor EC, Gillespie EF, Khan A, McCormick B, et al. Feasibility of Breast-Conservation Therapy and Hypofractionated Radiation in the Setting of Prior Breast Augmentation. Pract Radiat Oncol [Internet]. 2020/02/02. 2020 Sep;10(5):e357–62. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1879850020300035
- Prabhakaran S, Elston JB, Lleshi A, Kumar A, Sun W, Khakpour N, et al. Single Institution Review of Patients With Prior Breast Augmentation Undergoing Breast Conservation Therapy for Breast Cancer. Ann Plast Surg [Internet]. 2017;78(6S):S289–91. Available from: https://journals.lww.com/annalsplasticsurgery/Fulltext/2017/06005/Single_Institution_Review_of_Patients_With_Prior.9.aspx
- Gray RJ, Forstner-Barthell AW, Pockaj BA, Schild SE, Halyard MY. Breast-conserving therapy and sentinel lymph node biopsy are feasible in cancer patients with previous implant breast augmentation. Am J Surg. 2004/07/14. 2004;188(2):122–5.
- Group DBC. DBCG Kvalitetsindikatorrapport for Brystkræft 2021 [Internet]. Vol. 2022. 2021. Available from: https://www.dbcg.dk/images/PDF/Rapporter/DBCG_årsrapport_2021_Publiceret_FINAL.pdf
- Offersen B V, Alsner J, Nielsen HM, Jakobsen EH, Nielsen MH, Krause M, et al. Hypofractionated Versus Standard Fractionated Radiotherapy in Patients With Early Breast Cancer or Ductal Carcinoma In Situ in a Randomized Phase III Trial: The DBCG HYPO Trial. Journal of Clinical Oncology [Internet]. 2020;38(31):3615–25. Available from: https://doi.org/10.1200/JCO.20.01363
- Stevens GW, Calobrace BM, Alizadeh RK, Zeidler LK, Harrington CJ, D’incelli CR. Ten-year Core Study Data for Sientra’s Food and Drug Administration–Approved Round and Shaped Breast Implants with Cohesive Silicone Gel. Plast Reconstr Surg. 2018;141(4S Sientra Shaped and Round Cohesive Gel Implants):7S-19S.