Introduction
Colorectal Cancer (CRC) ranks third in global incidence and
is the second leading cause of cancer-related deaths, with latestage patients lacking effective treatment strategies [1]. Despite
the development of immunotherapy benefiting many late-stage
cancer patients, most CRCs are insensitive to immunotherapy. It is
widely believed that this is related to the immune microenvironment of CRC, where the infiltration and status of immune cells
are among the important reasons [2]. Tumor-Associated Macrophages (TAMs) are an essential component of the tumor immune microenvironment. Under certain conditions, TAMs can be
polarized into M1 or M2 phenotypes. M1 macrophages are generally considered to promote inflammation and exert anti-tumor
effects, while M2 macrophages suppress inflammation and promote immune tolerance. The polarization state of macrophages
is associated with drug resistance and prognosis of tumors, with
a high M2/M1 ratio being associated with immunotherapy resistance and poor prognosis [2,3].
Farnesoid X Receptor (FXR) is a nuclear receptor for bile acids,
highly expressed in intestinal epithelial cells under physiological conditions, and can be activated by bile acids to regulate bile
acid circulation and metabolism [4]. Recent studies have revealed
the important role of FXR in inhibiting CRC, with significantly decreased expression of FXR in colorectal cancer tissues compared
to normal tissues [5], and its association with the occurrence, progression, and drug resistance of CRC [6,7]. It is worth noting that
FXR is also expressed in certain cells in the tumor stroma, such as
macrophages, intestinal mononuclear cells, and T cells [8]. However, current research on FXR in CRC mainly focuses on its expression in cancer cells, while the expression and role of FXR in the
tumor stroma remain to be further studied.
This study aims to use immunohistochemistry to detect the
expression of FXR in tumor cells and tumor stroma separately,
analyze its correlation with the clinicopathological features of
colorectal cancer and the polarization state of macrophages, and
explore the significant impact of FXR on colorectal cancer.
Materials and methods
Conducted with approval from the Ethics Committee of Wuhan Central Hospital, this study involved the retrospective collection of data from the pathology-confirmed samples of colorectal
adenocarcinoma, which underwent surgical treatment at Wuhan
Central Hospital from January 2022 to December 2022. A total
of 48 patients were identified through the hospital’s sample database. Among them, 31 samples met the following inclusion
criteria: 1) Histopathological confirmation of primary colorectal
adenocarcinoma; 2) No prior anti-tumor treatments such as chemotherapy or radiotherapy; 3) Absence of a family history of malignant tumors or other malignancies; 4) Exclusion of cases with
insufficient tissue samples. Samples, including tumor tissue and
adjacent non-cancerous tissue, were fixed in 4% formaldehyde,
embedded in paraffin, and sectioned continuously at 5 μm thickness for subsequent research.
Data collection: Clinical and pathological characteristics of
colorectal cancer patients, including gender, age, location, size,
differentiation degree, clinical stage, Ki-67 expression, neural invasion, and vascular invasion, were collected through the laboratory information system and hospital information system of Wuhan Central Hospital for subsequent statistical analysis.
mmunohistochemistry procedure: Sections were deparaffinized in an environmentally friendly dewaxing solution, hydrated in a graded alcohol series, subjected to heat-induced antigen retrieval using a sodium citrate buffer in a microwave, and
blocked for endogenous peroxidase activity for 10 minutes. After
blocking with a goat serum at room temperature for 60 minutes,
the sections were incubated with primary antibodies overnight at
4°C (Mouse anti-human FXR monoclonal antibody 1:50, Perseus
Proteomics, A9033A; Rabbit anti-human CD86 monoclonal antibody 1:100, Huanan Biological, ET1606-50; Rabbit anti-human
CD206 polyclonal antibody 1:400, Proteintech, 18704-1-AP). Subsequently, the sections were incubated with secondary antibodies
at room temperature in the dark for 30 minutes, followed by DAB
color development. Counterstaining was performed with hematoxylin for 5 minutes, and then differentiation and bluing were
carried out. Dehydration was achieved through a graded alcohol
and environmentally friendly dewaxing transparent solution. Finally, the sections were air-dried and mounted with a resinous
medium.
Result interpretation: Immunohistochemistry slides were reviewed under a microscope at 400x magnification in three representative fields selected using a double-blind method. Qualitative
analysis of FXR expression was performed by identifying brownyellow granules located in the nucleus as positive, and the expression of FXR-positive cells in tumor cells and tumor stroma was
assessed separately. Quantitative analysis of CD86 and CD206 expression was conducted by identifying brown-yellow staining located on the cell membrane as positive. The number of positive
cells in each field was counted using Image J software, the average value was calculated for three fields, and the CD206/CD86
ratio was determined.
Data processing: Statistical analysis of FXR expression in tumor cells and tumor stroma, clinical pathological characteristics,
CD86 cell count, CD206 cell count, and CD86/CD206 ratio was
conducted using SPSS 21.0 statistical analysis software. The correlations among these variables were examined. For count data
such as age, size, Ki-67 expression, CD86 and CD206 cell counts,
and CD86/CD206 ratio, t-tests and non-parametric U-tests were
applied (t-tests were used when the data followed a normal distribution with equal variances, and non-parametric U-tests were
used when the data did not follow a normal distribution). For
quantitative data such as gender, location, stage, differentiation
degree, neural invasion, and vascular invasion, Fisher’s exact test
and Mann-Whitney U test methods were employed (Mann-Whitney U test was applied for ordinal variables, and Fisher’s exact
test was applied for unordered variables). A significance level of
P<0.05 was considered statistically significant, and numerical values were presented as mean ± standard deviation. Graphs and
charts were generated using GraphPad Prism 9 based on the experimental results.
Results
Expression of farnesoid X receptor in colorectal cancer tumor
cells and tumor stroma
Existing studies have indicated that the expression of FXR in tumor cells of colorectal cancer patients is lower compared to
normal tissues [5]. Additionally, some cells in the tumor stroma,
such as mononuclear cells, macrophages, and T cells, have been
shown to express FXR [8]. However, the specific expression pattern of FXR in the tumor stroma of colorectal cancer patients has
not been reported. In this study, immunohistochemical detection
of FXR expression was performed on 31 specimens according to
the aforementioned procedure.
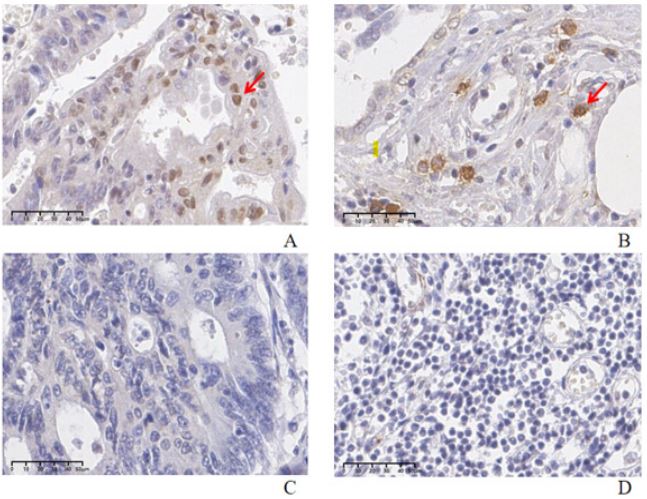
Microscopic observation was conducted (400×), and slides
were reviewed using a double-blind method. Brown-yellow granules located in the nucleus were considered positive expression.
The qualitative interpretation of FXR expression in tumor cells and
tumor stroma was categorized into positive expression group and
loss of expression group (Figure 1). The results showed that FXR
was expressed in both tumor cells and tumor stroma of colorectal
cancer. Among the 31 samples, 9 cases showed positive FXR expression in tumor cells, and 14 cases showed positive FXR expression in tumor stroma, with positive rates of 29.03% and 45.16%,
respectively.
Relationship between farnesoid X receptor expression and
clinical pathological characteristics of colorectal cancer
Current studies on the relationship between FXR expression
and clinical pathological characteristics of CRC have yielded conflicting results [5,9,10], and there is a lack of research on the correlation between FXR expression in the tumor stroma and clinical
pathological characteristics of CRC. This study collected clinical
pathological characteristics including gender, age, location, size,
differentiation degree, clinical stage, Ki-67, nerve invasion, and
vascular invasion from enrolled patients. The relationship between FXR expression in tumor cells and tumor stroma and clinical pathological characteristics was analyzed.
Regarding demographic characteristics, there was no significant statistical difference in FXR expression in tumor cells by gender (Table 1). The mean age of patients with FXR-positive expression in tumor cells was (66.8±9.4) years, while that of patients
with FXR-negative expression was (64.5±12.8) years, with no significant statistical difference between the two groups (P>0.05).
Due to the small sample size in this study, differences in lifestyle
habits and geographical factors between the two groups could
not be statistically analyzed.
Regarding the primary site of the tumor, differences were observed in FXR expression in tumor cells. The primary site of CRC
has received widespread attention in recent years, and it can be
divided into left-sided colon cancer and right-sided colon cancer
based on the splenic flexure, with different embryonic origins and
significant differences between them [11]. The CALGB/SWOG
80405 trial clarified the differences in treatment efficacy and survival prognosis between left-sided and right-sided colon cancer
and ongoing research has explored their differences in molecular
characteristics [12]. In this study, it was found that the expression of FXR in colon cancer cells was associated with the primary
site of the tumor, with a positivity rate of FXR in left-sided colon
cancer of 14.3% and in right-sided colon cancer of 60%. Patients
with left-sided colon cancer were more likely to have loss of FXR
expression compared to those with right-sided colon cancer, and
the difference between the two groups was statistically significant
(P=0.015). This conclusion supplements the differences in molecular expression between left-sided and right-sided colon cancer,
providing new insights into the molecular mechanisms underlying
the differences between left and right colon cancer.
However, FXR expression did not show significant statistical
differences in some traditional high-risk factors such as clinical
stage, differentiation, tumor size, Ki-67, nerve invasion, and vascular invasion. FXR expression was not associated with clinical
stage (P=0.170) or differentiation degree (P=0.305). The mean Ki67 value in the FXR loss group of tumor cells was (69.5±10.5)%,
which was higher than that in the FXR-positive expression group
(58.9±21.3)%, but there was no significant statistical difference
between the two groups (P=0.070). The proportion of nerve invasion was 33.3% in the FXR-positive group and 18% in the FXRnegative group, with no statistical difference between the two
(P=0.384). The proportion of vascular invasion was 55.6% in the
FXR-positive group and 45.5% in the FXR-negative group, with no
statistical difference between the two (P=0.704).
Similarly, the correlation between FXR expression in the tumor
stroma and the aforementioned clinical pathological characteristics was analyzed. The results showed that FXR expression in the
tumor stroma of colorectal cancer was not associated with gender, age, location, size, differentiation degree, clinical stage, Ki-67,
nerve invasion, or vascular invasion factors (P>0.05).
Relationship between farnesoid X receptor expression and
macrophage polarization
Macrophages are essential components of the tumor immune
microenvironment and can be polarized into M1 and M2 macrophages under certain conditions. CD86 and CD206 are commonly
used molecular markers for M1 and M2 macrophages, respectively [13,14]. In this experiment, immunohistochemistry was used to
detect the expression of CD86 and CD206, reflecting the polarization status of macrophages in the tumor microenvironment. The
relationship between FXR expression and the infiltration quantity
of M1, M2 macrophages, and the M1/M2 ratio was analyzed.
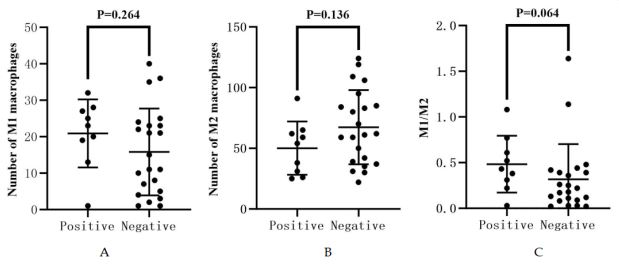
Under high-power magnification (400×), in the tumor cells
with positive FXR expression group, the infiltration quantity of M1
macrophages was (20.9±9.3), M2 macrophages was (50.1±21.9),
and the M1/M2 ratio was (0.5±0.3). In the FXR-deficient group,
the infiltration quantity of M1 macrophages was (15.8±11.9),
M2 macrophages was (67.4±30.5), and the M1/M2 ratio was
(0.5±0.4). The results showed that there was no significant correlation between the expression of FXR in tumor cells and the infiltration quantity of M1 (P=0.264) or M2 (P=0.136) macrophages,
as well as the M1/M2 ratio (P=0.064) (Figure 2).
Table 1: Analysis of FXR expression in colorectal cancer cells and
clinical pathological features clinical pathological features.
| Clinical pathological features |
Expression |
Expression loss |
P value |
| Gender |
Male
Female
Female |
4 |
9 |
0.999 |
| 5 |
13 |
| Age |
|
66.8+9.4 |
64.5±12.8 |
0.627 |
| Site |
Left-sided |
3 |
18 |
0.015* |
| Right-sided |
6 |
4 |
| Size |
|
4.3±1.3 |
3.9±1.6 |
0.274 |
Differentiation
grade |
Low |
5 |
6 |
0.305 |
Moderate
High |
2
2 |
11
5 |
| Clinical stage |
Ⅰ
Ⅱ
Ⅲ
Ⅳ |
2
3
4
0 |
10
8
2
2 |
0.170 |
| Ki-67 |
|
58.9±21.3 |
69.5±10.5 |
0.070 |
| Nerve invasion |
Positive |
3 |
4 |
0.384 |
| Negative |
6 |
18 |
| Vascular invasion |
Positive |
5 |
10 |
0.704 |
| Negative |
4 |
12 |
* P<0.05
In current studies concerning FXR expression in colorectal cancer CRC patients, the research focus has primarily been on cancer cells, lacking analysis of FXR expression in the tumor stroma.
The tumor stroma is an indispensable part of tumors and plays
a crucial role in tumor invasion, metastasis, and drug resistance
[15]. Therefore, this study further investigated the relationship
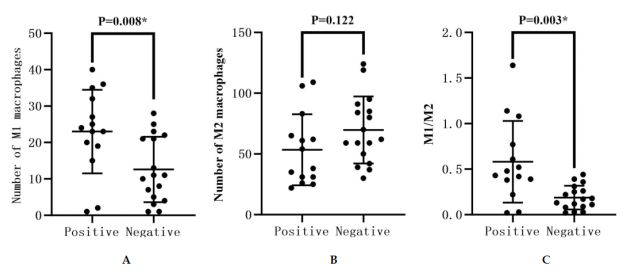
between FXR in the stroma and macrophage polarization. Under high-power microscopy (400×), the infiltration quantity of
M1 macrophages in the FXR-positive group in the tumor stroma
was (23.0±11.5), while that of M2 macrophages was (53.4±29.3),
with an M1/M2 ratio of (0.6±0.4). In contrast, in the FXR-deficient
group, the infiltration quantity of M1 macrophages was (12.6±9.0),
that of M2 macrophages was (69.7±27.6), with an M1/M2 ratio of
(0.2±0.1). The results indicate that compared to FXR expression
in tumor cells, FXR expression in the stroma is associated with
macrophage polarization. The FXR-positive group in the tumor
stroma showed a higher number of M1 cell infiltrations than the
FXR-deficient group (P=0.008), and the FXR-positive group had a
higher M1/M2 ratio (P=0.003), suggesting a trend towards M1
polarization of macrophages. However, there was no significant
correlation between the infiltration quantity of M2 macrophages
and FXR expression (P=0.122) (Figure 3).
Correlation between FXR expression in tumor stroma and the
infiltration quantity of M1 macrophages (P=0.008). (b) There is
no significant difference in the infiltration quantity of M2 macrophages between the FXR-positive and FXR-deficient groups in
tumor stroma (P=0.122). (c) There is a correlation between FXR
expression in tumor stroma and the M1/M2 ratio (P=0.003).
In summary, FXR expression in the stroma is associated with
polarization of macrophages toward the M1 phenotype. M1 macrophages can promote immune responses, and a high M1/M2
ratio in the tumor environment is more favorable for colorectal
cancer CRC patients to benefit from immunotherapy, indicating
a better prognosis. Patients with FXR deficiency exhibit a higher
proportion of M2 macrophages, which can promote the progression of CRC and are associated with immune tolerance in colorectal cancer patients [3,16].
Discussion
Colorectal cancer ranks third in global incidence and second in
cancer-related mortality worldwide, with a rising incidence, particularly notable in developing countries [17]. Moreover, there’s
a trend toward younger ages and later stages of diagnosis. Poor prognosis characterizes late-stage CRC patients, with a median
overall survival of about 30 months, posing a serious threat to
human health [18].
FXR, a member of the nuclear receptor superfamily, is activated
by bile acids, its endogenous ligands, to regulate bile acid circulation and metabolism under physiological conditions [19]. Recent
studies suggest that FXR plays a significant role in CRC, exerting
multiple pathways to inhibit CRC occurrence and development
[6,7,20]. However, the specific mechanisms of action remain to
be explored further.
This study demonstrates that FXR is expressed in both tumor
cells and the tumor stroma of CRC, with positivity rates of 29.03%
and 45.16%, respectively, and is correlated with CRC characteristics.
The expression of FXR in CRC tumor cells is associated with
tumor location, with FXR deficiency more common in left-sided
colon cancer. Left and right-sided colon cancers have differences in embryonic origins, treatment, and prognosis. Right-sided
colon cancer originates from the midgut, while left-sided colon
cancer originates from the hindgut, possibly forming the basis of
heterogeneity between left and right-sided colon cancers [11].
Studies have shown that patients with left-sided colon cancer
are more likely to benefit from anti-EGFR targeted therapy and
exhibit better prognosis than those with right-sided colon cancer
[21,22]. Mechanistic studies on the differences between left and
right-sided colon cancer have been a hot topic, possibly related
to differences in consensus molecular subtypes, genetic mutations, immune microenvironments, among other factors, but the
exact molecular mechanisms explaining the differences between
left and right-sided colon cancers remain to be fully elucidated
[23,24]. The results of this study show different expressions of FXR
in left and right-sided colon cancer, enriching the heterogeneity of
molecular expression between left and right-sided colon cancers.
The expression of FXR in the CRC tumor stroma is related to
the polarization status of macrophages in the CRC immune microenvironment. With the recent advances in immunotherapy,
many late-stage cancer patients, such as those with lung cancer
and melanoma, have benefited from immunotherapy, leading to
significantly prolonged survival [25]. Unfortunately, most CRCs
are not sensitive to immunotherapy, with the tumor immune microenvironment believed to be a key factor causing immune resistance in CRC [26,27]. TAMs are an important component of the
tumor immune microenvironment and can be polarized into two
phenotypes, M1 or M2, under certain conditions, exerting drastically different effects. M1 macrophages are generally considered
to promote inflammation, participate in immune responses, and
exhibit anti-tumor effects, while M2 macrophages can suppress
inflammation, promote tumor initiation and progression, and
mediate immune tolerance [27,28]. Studies have shown that the
polarization status of macrophages plays a decisive role in CRC
resistance to therapy, with the ratio of different subtypes of macrophages related to patient prognosis. A high M2/M1 ratio in the
immune microenvironment leads to CRC immune therapy resistance and predicts poor prognosis. The results of this study show
that CRC tumor stroma with positive FXR expression has a higher
infiltration of M1 macrophages and a higher M1/M2 ratio compared to the FXR deficiency group. This demonstrates the important role of FXR in shaping the colorectal immune microenvironment and suggests the potential of FXR as a therapeutic target for
CRC. Activating FXR expression is expected to reverse the state of
immune tolerance in colorectal cancer.
The expression of FXR is associated with CRC location and
macrophage polarization status, but the specific mechanisms of
action await further investigation. As a regulator that integrates
various key factors of CRC, FXR holds promise as a potential target
for CRC diagnosis and treatment, providing new insights into the
treatment of advanced CRC.
Conclusion
FXR is expressed in both tumor cells and the tumor stroma of
colorectal cancer patients, and the expression patterns of FXR in
both locations are correlated with the clinical and pathological
characteristics of CRC. The expression of FXR in tumor cells is associated with tumor location, with FXR deficiency being more common in left-sided colon cancer. The expression of FXR in the tumor
stroma is related to the polarization status of macrophages, with a
higher infiltration of M1 macrophages and a higher M1/M2 ratio
in the FXR-positive group compared to the FXR deficiency group.
Declarations
Conflicts of interest: Conflicts of interest does not exist.
Funding: This research was funded by the National Natural Science Foundation of China, grant number 81372931 and 82003238.
Publication ethics: The study was conducted in accordance
with the Declaration of Helsinki, and approved by the Ethics
Committee of The Central Hospital of Wuhan (protocol code
T20234106, 2023.09).
Data availability statement: Data available on request due to
restrictions privacy, the data presented in this study are available
on request from the corresponding author.
Acknowledgments: Not applicable.
References
- Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023; 72: 338-344.
- Chen Y, Zheng X, Wu C. The Role of the Tumor Microenvironment and Treatment Strategies in Colorectal Cancer. Front Immunol. 2021; 12: 792691.
- Li Y, Chen Z, Han J, et al. Functional and Therapeutic Significance of Tumor-Associated Macrophages in Colorectal Cancer. Front Oncol. 2022; 12: 781233.
- Chiang JYL, Ferrell JM. Discovery of farnesoid X receptor and its role in bile acid metabolism. Molecular and Cellular Endocrinology. 2022; 548: 111618.
- Lax S, Schauer G, Prein K, et al. Expression of the nuclear bile acid receptor/farnesoid X receptor is reduced in human colon carcinoma compared to nonneoplastic mucosa independent from site and may be associated with adverse prognosis. Int J Cancer. 2012; 130: 2232-2239.
- Yu J, Li S, Guo J, et al. Farnesoid X receptor antagonizes Wnt/betacatenin signaling in colorectal tumorigenesis. Cell Death Dis. 2020; 11: 640.
- Fu T, Coulter S, Yoshihara E, et al. FXR Regulates Intestinal Cancer Stem Cell Proliferation. Cell. 2019; 176: 1098-1112. e1018.
- Anderson KM, Gayer CP. The Pathophysiology of Farnesoid X Receptor (FXR) in the GI Tract: Inflammation, Barrier Function and Innate Immunity. Cells. 2021; 10: 3206.
- Zhang D, Weng S, Cui C, et al. Decreased expression of farnesoid X receptor may indicate poor prognosis in patients with colorectal cancer. Transl Cancer Res. 2020; 9: 4290-4296.
- Torres J, Bao X, Iuga AC, et al. Farnesoid X receptor expression is decreased in colonic mucosa of patients with primary sclerosing cholangitis and colitis-associated neoplasia. Inflamm Bowel Dis. 2013; 19: 275-282.
- Ghidini M, Petrelli F, Tomasello G. Right Versus Left Colon Cancer: Resectable and Metastatic Disease. Current Treatment Options in Oncology. 2018; 19: 31.
- Venook AP, Niedzwiecki D, Innocenti F. Impact of primary (1°) tumor location on overall survival (os) and progression-free survival (pfs) in patients (pts) with metastatic colorectal cancer (mcrc): Analysis of calgb/swog 80405(alliance). J Clin Oncol. 2017; 15: 3504.
- Dong P, Ma L, Liu L, et al. CD86(+)/CD206(+), Diametrically Polarized Tumor-Associated Macrophages, Predict Hepatocellular Carcinoma Patient Prognosis. Int J Mol Sci. 2016; 17: 320.
- Yunna C, Mengru H, Lei W, et al. Macrophage M1/M2 polarization. Eur J Pharmacol. 2020; 877: 173090.
- Wu T, Dai Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017; 387: 61-68.
- Vayrynen JP, Haruki K, Lau MC, et al. The Prognostic Role of Macrophage Polarization in the Colorectal Cancer Microenvironment. Cancer Immunol Res. 2021; 9: 8-19.
- Hossain MS, Karuniawati H, Jairoun AA, et al. Colorectal Cancer: A Review of Carcinogenesis, Global Epidemiology, Current Challenges, Risk Factors, Preventive and Treatment Strategies. Cancers (Basel). 2022; 14: 1732.
- Xi Y, Xu P. Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 2021; 14: 101174.
- Lee FY, Lee H, Hubbert ML, et al. FXR, a multipurpose nuclear receptor. Trends Biochem Sci. 2006; 31: 572-580.
- Modica S, Murzilli S, Salvatore L, et al. Nuclear bile acid receptor FXR protects against intestinal tumorigenesis. Cancer Res. 2008; 68: 9589-9594.
- Petrelli F, Tomasello G, Borgonovo K, et al. Prognostic Survival Associated With Left-Sided vs Right-Sided Colon Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2017; 3: 211-219.
- Tejpar S, Stintzing S, Ciardiello F, et al. Prognostic and Predictive Relevance of Primary Tumor Location in Patients With RAS WildType Metastatic Colorectal Cancer: Retrospective Analyses of the CRYSTAL and FIRE-3 Trials. JAMA Oncol. 2017; 3: 194-201.
- Lee GH, Malietzis G, Askari A, et al. Is right-sided colon cancer different to left-sided colorectal cancer? - a systematic review. Eur J Surg Oncol. 2015; 41: 300-308.
- Yang SY, Cho MS, Kim NK. Difference between right-sided and leftsided colorectal cancers: From embryology to molecular subtype. Expert Rev Anticancer Ther. 2018; 18: 351-358.
- Gong J, Chehrazi-Raffle A, Reddi S, et al. Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: A comprehensive review of registration trials and future considerations. J Immunother Cancer. 2018; 6: 8.
- Yang W, Zheng H, Lv W, et al. Current status and prospect of immunotherapy for colorectal cancer. Int J Colorectal Dis. 2023; 38: 266.
- Zou Z, Lin H, Li M, et al. Tumor-associated macrophage polarization in the inflammatory tumor microenvironment. Front Oncol. 2023; 13: 1103149.
- Kishore C, Bhadra P. Current advancements and future perspectives of immunotherapy in colorectal cancer research. Eur J Pharmacol. 2021; 893: 173819.