Case presentation
The patient sought medical attention at the outpatient clinic
due to experiencing epigastric discomfort persisting for a duration
of 20 days. Subsequent gastroscopy conducted at the outpatient
clinic revealed the presence of circumferential thickening in the
gastric antrum and encroachment of the duodenal bulb across
the pyloric ring. Additionally, biopsy of the intragastric lesion
indicated the presence of high-grade intraepithelial neoplasia.
Upon admission, the patient reported postprandial bloating and
discomfort, accompanied by a loss of appetite. However, there
were no reports of nausea, vomiting, or weight loss. Abdominal
examination did not reveal any signs of abdominal pain, and the
remainder of the physical examination yielded no noteworthy
findings. The patient presented with a documented history of
hypertension spanning three years, effectively managed through
standardized medication. No additional gastrointestinal symptoms were reported. Laboratory tests, including admission blood
routine, biochemical routine, and gastrointestinal tumor markers, did not reveal any abnormalities. Furthermore, the serum antibody test for Helicobacter pylori yielded a negative result.
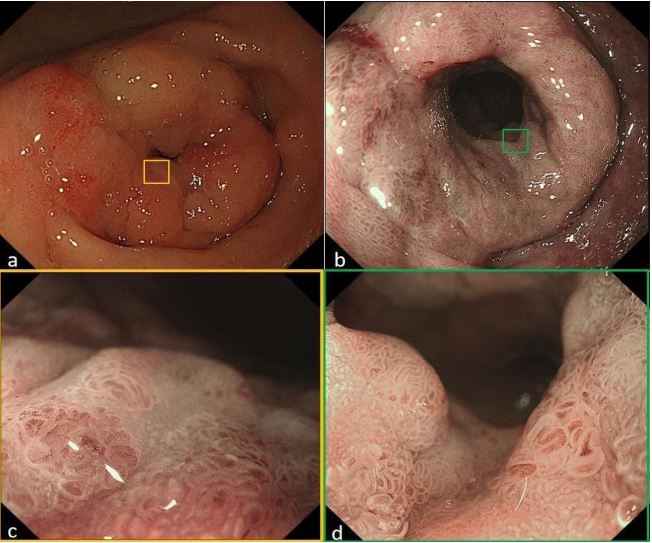
Following that, a meticulous examination of the upper gastrointestinal endoscopy was conducted, revealing the thickening of
the distal gastric sinus and pyloric ring, accompanied by an unevenly elevated surface (type 0-I and 0-IIa) (Figures 1a,1b). Notably, no ulceration or erosion was observed. Further assessment
through Narrow-Band Imaging Magnification Endoscopy (NBIME) demonstrated that the gastric sinus exhibited a background
of atrophic mucosa, while the overall mucosa of the lesion displayed a distinct “tea browness color”. Additionally, irregular widening of the ducts, covered by White Opaque Substance (WOS)
(Figures 1c,1d). During the endoscopic insufflation test, the lesion
demonstrated softness and displayed normal functionality of the
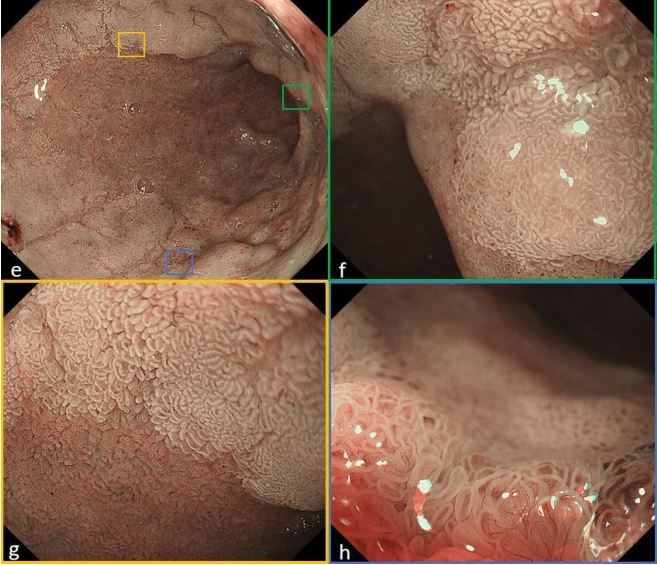
pyloric ring. The lesion extended into the duodenal bulb, where
it exhibited a characteristic flat and elevated appearance (type
0-IIa) with a distinct boundary, resembling the morphology of a
Laterally Spreading Tumor (LST) in the colon (Figure 2e). Magnification observation using NBI revealed that a significant portion of
the lesion’s surface was extensively attached with WOS. The glandular ducts exhibited Irregular Microvascular Pattern (IMVP) and
Irregular Microsurface Pattern (IMSP), while the blood vessels
displayed varying thickness and disorganized alignment (Figures
2f,2h). However, the level of disorganization observed was comparatively lower than that observed in the gastric sinus lesions.
Regrettably, the unavailability of indigo carmine staining and ultrasonic endoscopy hindered their utilization in this study due to
material constraints in the endoscopy department. The abdominal CT scan revealed a marginal thickening of the gastric sinus,
with no evidence of distant metastasis or enlarged perigastric
lymph nodes. Multiple biopsies were obtained from intragastric
and duodenal lesions, indicating high-grade intraepithelial neoplasia in the gastric sinus, low-grade intraepithelial neoplasia in
the duodenum, and focal high-grade neoplasia.
Treatment programs
Following a Multidisciplinary Team (MDT) evaluation encompassing gastrointestinal surgery, gastroenterology, imaging and
pathology departments, a unanimous consensus was reached
indicating a high likelihood of EGC for the lesion under consideration. However, due to the lesion’s extensive size and circumferential growth involving the pylorus and duodenum, endoscopic
treatment posed significant challenges, with potential complications such as stenosis and perforation difficult to avoid after
Endoscopic Submucosal Dissection (ESD). Consequently, surgical
intervention emerged as the preferred treatment option. Subsequently, the patient underwent laparoscopic-assisted major
gastrectomy with B-II anastomosis and D2 lymph node dissection. Following the postoperative pathological examination of the
tumor, it was determined that the gastric sinus lesion exhibited
characteristics of highly differentiated adenocarcinoma, while
the duodenal lesion displayed primarily low-grade intraepithelial
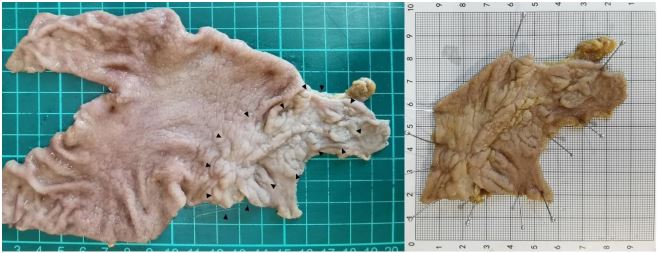
neoplasia. The lesion measured approximately 6.5 cm x 4.6 cm
and was confined to the mucosal muscular layer, with cancer cells
extending to the duodenum. The distance from the anal side to
the pyloric ring was 2.6 cm (Figure 3), and the margins were devoid of cancer cells. Notably, there was no evidence of lymph or
venous invasion, nor any metastasis to peripheral lymph nodes.
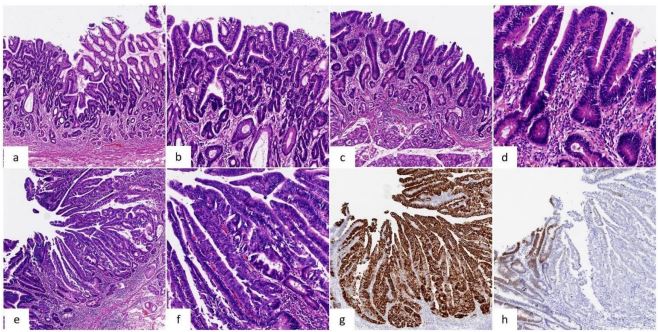
Based on these findings, the tumor was classified as pT1aN0M0 Ia stage.The surgical specimen revealed the presence of High-Grade
Intraepithelial Neoplasia (HGIN) with localized moderately differentiated adenocarcinoma(Figures 4a-4f).Immunostains suggests
that the lesion as a whole is strongly positive for Muc5ac and
partially positive for CDX2 (Figures 4g,4h). P53 exhibited weak
staining (1+) in 30% of cells, and the Ki-67 proliferation index was
measured at 60%. Following surgical intervention, the patient
experienced a successful recovery and was discharged from the
hospital after 11 days. Subsequently, during a 13-month followup period, the patient remained in a stable condition without any
signs of recurrence.
Discussion
The etiology of gastric cancer is influenced by a combination
of genetic predisposition and environmental factors [2]. ECG
patients are usually asymptomatic. In the case, the patient with
early gastric cancer exhibited peripheral growth in the distal
gastric sinus and pyloric ring, only resulting in discomfort such
as abdominal bloating rather than the typical symptoms associated with malignant tumors in the distal stomach. This highlights
the significance of utilizing endoscopy for the early diagnosis of
gastric cancer. Advanced gastric cancer in the antrum has been
found to occasionally invade the pyloric ring and duodenum,
with a majority of cases demonstrating submucosal vertical invasion. The occurrence of ECG invading the duodenum while being
confined to the mucosa is extremely rare. Namikawa T et al. [3]
examined reports from the Japanese Centra database spanning
33 years after 1975, identifying 13 similar cases. The average tumor diameter was measured at 6.3 cm, with the mean length of
duodenal infiltration recorded at 0.9 cm (ranging from 0.2 to 3.8 cm). Based on the Japanese pathologic staging system for early
gastric cancer, the predominant tumor types observed in these
cases were Tub (differentiated) and Sig (signet ring) tumors. Our
case aligns with Tub1 classification, as confirmed by immunohistochemistry indicating gastric type gastric cancer. Furthermore,
the extent of duodenal invasion in our case exceeded the mean
diameter reported in existing literature. A comprehensive search
of the Medline database spanning the past two decades yielded a
mere four pertinent reports [3-5]. In contrast, this case was extensively documented, presenting a series of consecutive magnified
endoscopic and histopathologic images that effectively illustrate
not only the macroscopic morphological alterations of the lesion,
but also offer a comprehensive Magnifying Endoscopy (NBI-ME)
perspective of the flat and depressed regions within the lesion.
The clinical definition of the boundary between the stomach
and duodenum poses challenges due to its lack of clear demarcation [6]. In practice, the pyloric ring is commonly employed
as a reference point to distinguish between the two anatomical
structures. However, this demarcation is better characterized as
a region of pyloric annulus, as the criteria for delineating this line
are not as stringent as those applied to the boundary between
the stomach and esophagus in clinical settings. From a clinicopathological perspective, the commencement of Brunner’s gland
is frequently employed as the demarcation boundary between
the stomach and the duodenum [7]. The prevalence of malignant
neoplasms at the gastroduodenal junction in clinical settings is
considerably lower compared to those occurring at the esophagogastric junction. Is there a correlation between the distinctive
structure of the pyloric region and the recurrence of Early Gastric
Cancer (EGC)? A Japanese scholar [8] reported a case that EGC
recurrenced in the pyloric region, occurring eight months after
Endoscopic Mucosal Resection (EMR). The recurrence was accompanied by extensive infiltration in the duodenal mucosa, leading
to the suspicion that the disruption of the microstructure of the
gastroduodenal mucosa caused by EMR facilitated the invasion
of cancer cells into the duodenal mucosa. This prompts the question of whether there exists a barrier between the mucosa and
submucosa of the gastroduodenum that hinders the progression
of gastric tumors towards the distal end? Scholars [1] have noted
that Brunner’s glands can remain unaffected even when cancer
cells directly infiltrate the duodenal mucosa. Therefore, it can be
hypothesized that Brunner’s glands may potentially impede the
advancement of gastric cancer cells from the gastric mucosa to
the duodenum. Brunner’s glands, situated in the submucosa of
the duodenum [9], serve the purpose of producing an alkaline
fluid that counteracts gastric acid. Additionally, these glands secrete various substances such as epidermal growth factor, trefoil
peptides, bactericidal factors, proteinase inhibitors, and surfaceactive lipids. These components effectively bind to the mucus
layer, safeguarding it and the underlying mucosa from degradation caused by gastric acid, pancreatic enzymes, and other surfactants present in the area. However, the medical community has
not provided detailed elucidation on the potential involvement of
Brunner’s gland in tumor suppression. From a molecular pathology standpoint, it has been proposed that the demarcation between gastric and duodenal regions lies in the expression boundary of SOX2 and CDX2 [10]. Additionally, abnormal CDX2 expression in the stomach is believed to be associated with intestinal
metaplasia, which in turn is closely linked to the development of intestinal-type gastric cancer. This provides evidence, in part, for
the molecular expression boundary theory. It is worthwhile to investigate the presence of crucial proteins in the duodenum that
possess the ability to impede tumorigenesis.
The utilization of endoscopic techniques has become increasingly prominent in the management of gastric and duodenal early
cancers [11]. As per the sixth edition of the Japanese Guidelines
for the Treatment of Gastric Cancer [12], intramucosal carcinoma
exceeding a diameter of 2 cm (cT1a), differentiated carcinomas,
and UL0 are regarded as definitive indications for endoscopic
intervention. However, in the case of lesions situated in specific
regions, such as sizable Early Gastric Cancers (EGCs) found in the
pylorus, cardia, and duodenum, while Endoscopic Submucosal
Dissection (ESD) is theoretically viable as a treatment option, it
necessitates a surgeon with advanced proficiency in this intricate
technique, as well as thorough readiness to manage potential
postoperative gastrointestinal perforation and stenosis. Nakayama et al. [13]reviewed 24 cases of invasion of the duodenum in
Japan and found that duodenal infiltration was detectable preoperatively in only 4 cases. Their findings revealed that preoperative
detection of duodenal infiltration was only possible in four cases.
Consequently, when dealing EGCs located in close proximity to
the pylorus, it is crucial to thoroughly evaluate lesion margins
prior to endoscopic treatment and exercise caution when selecting the appropriate resection method. The presence of a tubular
structure in the pyloric region poses additional challenges to endoscopic treatment, necessitating a careful assessment of the risk
of positive margins before opting for EMR treatment. ESD mitigates the likelihood of margin positivity; however, it is imperative
to conduct the procedure subsequent to magnification endoscopy for the purpose of accurately delineating the tumor boundary.
In this case, the decision to opt for laparoscopic-assisted surgery
instead of ESD treatment was based on a thorough assessment of
the tumor’s location and dimensions. Furthermore, Laparoscopic
Endoscopic Cooperative Surgery (LECS) [14] has been documented as an investigative therapeutic alternative for specific sites of
EGC, offering superior preservation of healthy tissues and organs
compared to standalone surgery. In summary, it is imperative to
thoroughly assess lesions in the pyloric region prior to surgery in
order to determine the potential risk of duodenal invasion, irrespective of the stage.
Conclusion
In summary, further investigation of additional cases is warranted to enhance our understanding of the underlying mechanism of early gastric cancer with duodenal invasion. Our study has
revealed that early gastric cancers situated in the gastric antrum,
particularly in the prepyloric region, possess the ability to directly
infiltrate the duodenal mucosal layer.
Declarations
Acknowledgements: This work was completely supported by
Weifang People’s Hospital.
Author’s contributions: Guangxu Zhu, and Hao Fu conjectured
the study and reviewed the paper; Guangxu Zhu, and Shengjie
Zhou analyzed the data and wrote the draft; Hao Fu, and Aifeng
Pan selected the patients and collected the data.
Funding: Funding program: The Scientific Research Project of
Weifang Health Commission
(WFWSJK-2021-028), Medical and Health Science Technology
Development Program in Shandong Province (202104080159,
202204010313), Natural Science Foundation of Shandong Province (ZR2022LSW005), Science Technology Development Program
in Weifang City (2021YX007),
Availability of data and materials: All data generated or analysed during this study are included in this published article.
Ethics approval and consent to participate: Not applicable.
Consent for publication: Not applicable.
Competing interests: The authors declare that they have no
competing interests.
References
- Kakeji Y, Tsujitani S, Baba H, Moriguchi S, Mori M, et al. Clinicopathologic features and prognostic significance of duodenal invasion in patients with distal gastric carcinoma. Cancer. 1991; 68(2): 380-4.
- Matsuda A, Kato S, Furuya M, Shimizu Y, Okino T, et al. Multiple early gastric cancer with duodenal invasion. World J Surg Oncol. 2007; 5: 125.
- Namikawa T, Kobayashi M, Kitagawa H, Okabayashi T, Dabanaka K, et al. Early gastric cancer with widespread duodenal invasion within the mucosa. Dig Endosc. 2010; 22(3): 223-7.
- Khan S, Zhu LP, Zhang Y, Chen X, Wang BM. Laterally spreading tumour of the distal stomach: A case report. BMC Cancer. 2018; 18(1): 502.
- Matsuda A, Kato S, Furuya M, Shimizu Y, Okino T, et al. Multiple early gastric cancer with duodenal invasion. World J Surg Oncol. 2007; 5: 125.
- Li X, Udager AM, Hu C, Qiao XT, Richards N, et al. Dynamic patterning at the pylorus: Formation of an epithelial intestine-stomach boundary in late fetal life. Dev Dyn. 2009; 238(12): 3205-17.
- Krause WJ. Brunner’s glands: A structural, histochemical and pathological profile. Prog Histochem Cytochem. 2000; 35(4): 259-367.
- Ishikawa M, Kitayama J, Fujii S, Ishigami H, Kaizaki S, et al. Recurrent intramucosal gastric carcinoma with extensive invasion to duodenal mucosa after endoscopic mucosal resection: A case report. Am Surg. 2005; 71(4): 366-8.
- Goldner B, Stabile BE. Duodenal adenocarcinoma: Why the extreme rarity of duodenal bulb primary tumors? Am Surg. 2014; 80(10): 956-9.
- San Roman AK, Shivdasani RA. Boundaries, junctions and transitions in the gastrointestinal tract. Exp Cell Res. 2011; 317(19): 2711-8.
- Yamada T, Sugiyama H, Ochi D, Akutsu D, Suzuki H, et al. Risk factors for submucosal and lymphovascular invasion in gastric cancer looking indicative for endoscopic submucosal dissection. Gastric Cancer. 2014; 17(4): 692-6.
- Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer. 2023; 26(1): 1-25.
- Nakayama Y, Kadowaki K, Hirata K, Higure A, Nagata N, et al. A case report of early gastric cancer with duodenal extension. Jpn J Gastroenterol Surg. 2004; 37: 506-511.
- Hiki N, Nunobe S. Laparoscopic endoscopic cooperative surgery (LECS) for the gastrointestinal tract: Updated indications. Ann Gastroenterol Surg. 2019; 3(3): 239-246.