Introduction
In 1764, Baurienne described an idiopathic and fatal necrotizing process that led to gangrene of the male genitalia [1]. However, Jean Alfred Fournier, a dermatologist expert in venereology,
who described this pathology in more detail based on a series of
5 cases of male patients in 1883 [2]. Since then, understanding
of the pathophysiology and etiology of the disease has been increasing. In the first descriptions, it was thought to be a pathology
exclusive to adult men, although it was later found that it could
affect women and children with a much lower prevalence [1].
Fournier’s Gangrene (FG) is a rare and potentially fatal infectious disease, with a mortality rate between 20 and 40% [3]. It is
a necrotizing fasciitis that affects the external genitalia, perineum and perianal region. The prevalence of this is around 0.02%
of hospital admissions, with an incidence ratio of 1.6 cases per
100,000 men/year. The female/male ratio is 1:10, with males
mainly affected in the age group of 40 to 50 years [4].
Material and methods
A narrative literature review narrative has been carried out to
identify the risk factors and etiology of FG, as well as to describe
the diagnostic methods and therapeutic management of it. A has
been carried out a bibliographic search in primary and secondary sources using as a search strategy: (“Fournier” [All Fields] or
“suppliers” [All Fields], (“Fournier gangrene” [MeSH Terms] or
(“Fournier” [All Fields] and “gangrene” [All Fields]) or (“Fournier”
[All Fields] and “gangrene” [All Fields]), including only studies in
Spanish and English.
Table 1: Evaluation and scoring system for Fournier’s Gangrene: Fournier Gangrene Severity Index (FGSI).
| Variable |
Abnormal high values |
Normal |
Abnormal low values |
| Score |
4 |
3 |
2 |
1 |
0 |
1 |
2 |
3 |
4 |
| Temperature (oC) |
>41 |
39-40,9 |
- |
38,5-38,4 |
36-38,4 |
34-35,9 |
32-33,9 |
30-31,9 |
<29,9 |
| Heart rhythm (lpm) |
>180 |
140-179 |
110-139 |
- |
70-109 |
- |
56-59 |
40-54 |
<39 |
| Frequencyrespiratory (rmp) |
>50 |
35-49 |
- |
25-34 |
24-12 |
11;-10 |
9;-6 |
- |
<5 |
| Serum sodium (mmol/l) |
>180 |
160-179 |
155-159 |
150-154 |
130-149 |
- |
120-129 |
111-119 |
<110 |
| Serum potassium (mmol/l) |
>7 |
6-6,9 |
- |
5,5-5,4 |
3,5-4 |
3-3,4 |
2,5-2,9 |
- |
<2,5 |
| Serum creatine (mg) |
>3,5 |
2-3,4 |
1,5-1,9 |
- |
0,6-1,4 |
- |
<0,6 |
- |
- |
| Hematocrit (%) |
>60 |
- |
50-59,9 |
46-49 |
30-45,9 |
- |
20-29,9 |
- |
<20 |
| GB (total mm³/1.000) |
>40 |
- |
20-39,9 |
15-19,9 |
3-14,9 |
- |
1-2,9 |
- |
<1 |
| Serum bicarbonate (mmol/l) |
>52 |
41-51,9 |
- |
32-40,9 |
22-31,9 |
- |
18-21,9 |
15-17,9 |
<15 |
Table 2: Antibiotic therapy regimens recommended for the treat-
ment of Fournier’s Gangrene with mixed microbiological etiology.
| Antibiotic |
Dose |
| Piperacillin-Tazobactan+ Vancomycin |
4,5 g c/6-8 h iv + 15 mg/kg c12 h |
| Imipenem-Cilastatina |
1 g c/6-8 h iv |
| Meropenem |
1g c/8 h iv |
| Ertapenem |
1g /24h |
| Gentamicin |
5mg/kg c/24h |
Cefotaxime+Metronidazole+Clinda
mycin |
2 g c/6h iv + 500 mg c/6h iv + 600-900
mg c/8h iv |
| Cefotaxima+Fosfomicin+Metronidazol |
2g c/6 h iv + 5g c/8h iv +500 mg c/6h iv |
Results and discussion
Etiology and common microorganisms
The cryptogenic nature of this illness has been reduced to a
scarce 10% and inflammatory processes and local lesions have
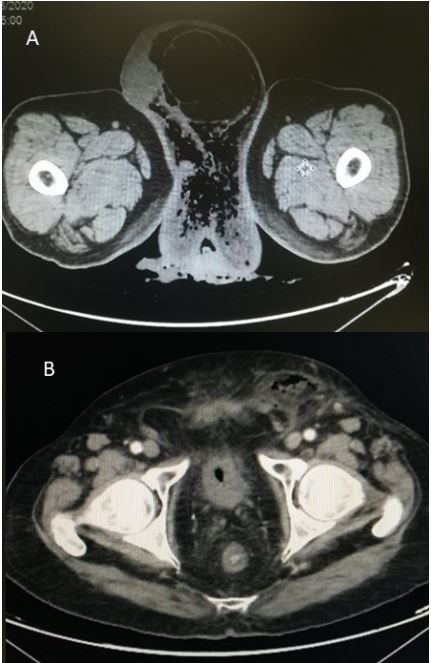
gained weight as the origin of FG. In 90% of cases, a clear triggering cause is identified. Of them, the most common are: perianal
pathology (especially perianal abscesses, complex fistulas and
anal fissures) (Figure 1A), genitourinary diseases (such as urethral
injuries, whether in patients with a permanent urinary catheter
or not), genitourinary infections (including postoperative genital
infections) (Figure 1B), malformations (such as hypospadias), and
skin lesions resulting from trauma or infectious processes [5].
FG is a polymicrobial or type 1 necrotizing fasciitis, with mixed
flora of aerobic and anaerobic bacteria. Usually at least one anaerobic species is found such as Bacteroides, Clostridium or Peptostreptococcus. These are usually isolated in combination with
someenterobacteria such as E. Coli, Enterobacter, Klebsiella or
Proteus and one or more non-group A facultative anaerobic streptococci, such as S. agalactiae [4].
Predisposing factors
There are several conditions related to the appearance of the
disease. Diabetes mellitus has been identified as the most prevalent comorbidity in patients with Fournier’s gangrene, since hyperglycemia directly affects the functions of chemotaxis, phagocytosis and cellular immune response [4]. In recent years and with
the appearance of inhibitors of cotransporters sodium-glucose
type II, cases of FG are described in patients who use them [6,7].
However, other predisposing factors have also been identified
such as obesity, neurological deficit, chronic alcoholism, malignant neoplasms, chronic corticosteroid consumption, malnutrition, HIV infection, peripheral vascular disease and essential hypertension [4].
Laor and collaborators (cols.) described FGSI (Fournier Gangrene Severity Index, Table 1) [8] with the aim of evaluating the
severity of FG. A score greater than or equal to 9 on this index is
associated with a 75% probability of death, and a score less than
9 indicates a 78% probability of survival [9].
Amr Ehab El-Qushayri and cols. in the metanalysis that they
published in 2020 showed that there was a higher risk of mortality in patients with diabetes, cardiovascular disease, acute kidney
failure and kidney disease [10]. However, no association was demonstrated between mortality and hypertension, lung disease, liver
disease or tumor pathology [11].
Recently, in Agost 2023, A. Tufano and cols. published a systematic review and metaanalysis above a value to apply the systems Fournier’s gangrene score on admission to predict mortality. For it, they used the FGSI, the simplified FGSI (SFGSI), and the
Uladag FGSI (UFGSI). They concluding that high values are associated with a highest mortality, with the UFGSI being the most
accurate [12].
Pathophysiology
In FG there is usually an entry point in the skin. After the penetration of the germs, the infection is favored by the mentioned
factors that generate an imbalance between the host’s immunity and the virulence of the microorganisms. The production of
enzymes such as collagenase, lecithinase and exotoxins, lead to
rapid multiplication of microorganisms and the spread of the disease. Invading bacterias cause thrombosis in vessels found in the
hypodermis, leading to tissue ischemia aggravated by edema. The
decrease in oxygen in the tissues favors the proliferation of anaerobic bacteria with the consequent necrosis of the fascia [13].
Diagnostic evaluation
The diagnostic is fundamentally clinical. It is a condition that
is characterized because in most cases it begins with perianal or
perineal pain, which seems disproportionately greater than the
physical finding, accompanied by inflammation, erythema, edema or pruritus in the affected area.
During the first 24 hours it evolves to necrosis, crepitation, foul
odor and exudate serosanguineous dark. Between the following
48 and 72 hours, the erythema takes blue-black color and evolves
towards tissue necrosis (Figure 2). On the fourth or fifth day, gangrene is evident, there is a decrease in pain due to necrosis of the
nerves and between the eighth and tenth day, the necrotic tissue
is separated by a suppurative process from the adjacent tissues
[14].
As for systemic manifestations, they are usually caused by
deterioration of general condition, marked prostration, nausea
and vomiting, progressing to hydroelectrolyte alterations, sepsis,
shock and death.
In general, patients consult a doctor once the necrotic lesions
have been established, although in some cases they consult before this evolutionary stage [15].
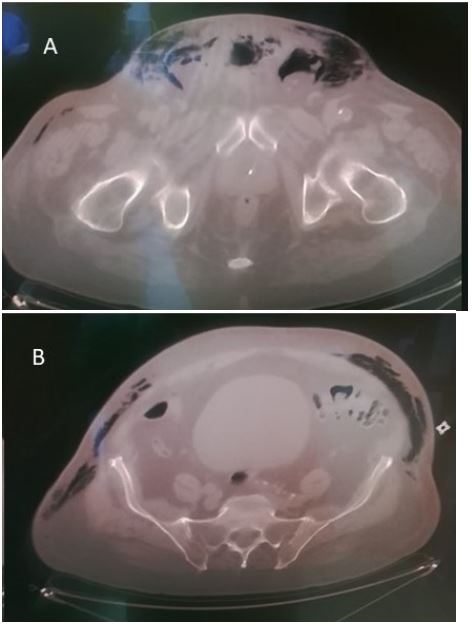
The diagnosis can be supported by radiological imaging techniques (Figure 3). Among them is the simple genitourinary radiograph, which can show a thickening of the soft tissues associated
with a radiolucent pattern demonstrating interstitial gas in the
subcutaneous tissues, although it does not allow demonstrating fascial involvement. Genital ultrasound may show edema of
the affected wall with diffuse hyperechogenic foci giving a typical
dirty appearance due to subcutaneous emphysema, accompanied by reactive unilateral or bilateral hydrocele in males when the scrotum and testicular sheaths are affected. The Computerized Tomography (CT) is the most sensitive and specific technique.
The most frequently found finding is subcutaneous emphysema,
which appears in 90% of cases as a granular hypodense area. Despite this being a usually present sign, we cannot rule out the diagnosis of FG when it does not exist. Additionally, CT can show
the presence of subcutaneous collections and the extent of fascial
damage, which could not be demonstrated with the other techniques [16].
For microbiological diagnosis, a sample must be taken from a
representative area, in an adequate quantity, avoiding contamination of commensal flora and before administering antibiotic
treatment [17]. Aspiration of purulent collections (deeper area)
with a needle and syringe, biopsy and curettage are preferred to
swabs. However, some studies have indicated that this last method is simpler, cheaper, non-invasive and useful for wounds [17].
The rapid and correct transport of the samples (transport means
or capped syringe), as well as their proper processing, will be of
great importance for the recovery of microorganisms, especially
anaerobes [17]. Gram stains and cultures should be done in aerobic and anaerobic media [17].
Treatment
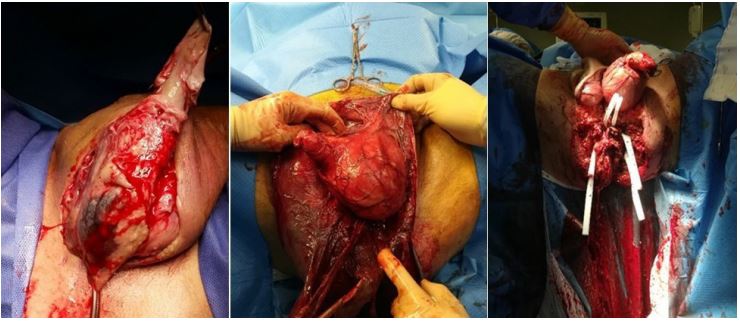
Currently, treatment is based on initial surgery, with extensive debridement and resections (Figure 4), removing all necrotic
or infected tissue associated with profuse lavage and the use of
broad-spectrum antibiotic therapy (Table 2) [18,19].
It has been proven that tissue gangrene can reach dizzying
speeds of up to 2-3cm/h, so rapid diagnosis and early initiation of
surgical treatment is vital [18].
Furthermore, it has been shown that the degree of internal
necrosis involvement is often much greater than that suggested
by external signs, and therefore, repeated debridement is usually
necessary in order to reduce mortality [20].
An important part of FG therapy is good local hygiene (wound
dressings should be changed at least twice a day) [21]. In addition,
it is not uncommon for an orchiectomy, cystostomy, or diverting
colostomy to be required, depending on the extent of the infection, ifIt isIt has reached the scrotum, perineal area, or lower abdominal wall, respectively [22].
In case of septic shock, replacement with abundant fluids, crystalloids and colloids if necessary, in addition to perfusion with vasopressors is essential [20,22,23].
Recommended antibiotic therapy (Table 2) would involve a
broad-spectrum penicillin or third-generation cephalosporin, gentamicin and metronidazole or clindamycin, although it should be
adjusted and directed according to the results of microbiological
cultures [20-23].
Conclusion
Fournier’s Gangrene is a necrotizing fasciitis that affects the
external genitalia, perineum and perianal region, with eventual
extension to the abdomen, lower limbs and evenal thorax. It is a
rare pathology (1.6 cases per 100,000 men/year) but with a high
mortality rate (20-40%).
The diagnosis is fundamentally clinical, based on complementary analytical, microbiological and radiological tests, with Computed Tomography (CT) being the most sensitive and specific imaging test for the diagnosis of this disease.
The three fundamental pillars of FG treatment are hemodynamic support of the patient, broad-spectrum empirical antibiotic
therapy and early surgical debridement. It is a time-dependent
disease. Early diagnosis is essential for urgent surgical debridement (<24h) in order to reduce the mortality rate. It is important
to remember the need to carry out active post-surgical surveillance in case the patient’s re-intervention is necessary.
Prevention and correction of risk factors in the population
would help reduce the incidence of this disease, which is often
unsuspected and whose result can be fatal.
Authors’ Contribution and conflicts of interest
Marta Guzman Perez: Takes responsibility for the integrity of
the data and the accuracy of the data. Study concept and design,
drafting of the manuscript, critical review of the manuscript for
important intellectual content.
Julián Solis García del Pozo: Study concept and design, drafting
of the manuscript, critical review of the manuscript for important
intellectual content.
Pablo Luis Guzmán Martínez-Valls: Study concept and design,
drafting of the manuscript, critical review of the manuscript for
important intellectual content.
All authors have read and approved the final version of the
manuscript and declare that this manuscript is original and has
not been edited or sent to another publication, nor is it in the process of being evaluated by any other scientific journal and declare
that are free from any personal or commercial association that
could imply a conflict of interest in connection with the article and
they have respected the ethical principles of research.
References
- Baurienne H. Sur une plaie contuse qui s’est terminee par le sphacele de le scrotum. J Med Chir Pharm. 1764; 20: 251-253.
- Fournier A. Semaine Médical. 1883; 2(3): 345-347.
- Camargo L, García Perdomo H. Gangrena de Fournier: Revisión de factores determinantes de mortalidad. Revista Chilena de Cirugía. 2016; 68(3): 273-277.
- Vargas T, Mora S, Zeledón A. Gangrena de Fournier: Generalidades. Revista Médica Sinergia 2019; 4(6): 100-107.
- Montoya R, Izquierdo E, Pietricica BN, Pellicer E, Aguayo JL, et al. Análisis descriptivo de 20 casos y revisión de la bibliografía científica. Actas Urologicas Españolas. 2009; 33(8): 873-880.
- Bersoff-Match SJ, Chamberlain C, Cao C, Kortepeter C, Chong WH. Fournier gangrene associated with sodium–glucose cotransporter-2 inhibitors: A review of spontaneous postmarketing cases. Annals of Internal Medicine. 2019; 170 (11): 764-769. doi: 10.7326/M19-0085.
- Tran BA, Updike WH, Bullers K, Serag-Bolos E. Sodium-Glucose Cotransporter 2 Inhibitor Use Associated With Fournier’s Gangrene: A Review of Case Reports and Spontaneous Post-Marketing Cases. Clin Diabetes. 2022; 40(1): 78-86. doi: 10.2337/cd21-0015.
- Laor E, Palmer LS, Tolia BM, Reid RE, Winter HI. Outcome prediction in patients with Fournier’s gangrene. J Urol. 1995; 154: 89-92.
- Fernández DA, Guillén AH, Uribe J, Romero R, Gutierrez A. Etiología de la gangrena de Fournier como factor pronóstico de mortalidad: Análisis de 121 casos. Actas Urológicas Españolas. 2019; 43(10): 557-561.
- El-Qushayri AE, Khalaf KM, Dahy A, Mahmoud AR, Benmelouka AY, et al. Fournier’s gangrene mortality: A 17-year systematic review and meta-analysis. Int J Infect Dis. 2020; 92: 218-225.
- Singh A, Ahmed K, Aydin A, Shamim M, Dasgupta P. Fournier´s gangrene. A clinical review. Archivo Italiano di Urologia e Andrologia. 2016; 88(3): 157-164.
- Tufano A, Dipinto P, Passaro F, Anceschi U, Franco G, et al. The Value of Fournier’s Gangrene Scoring Systems on Admission to Predict Mortality: A Systematic Review and Meta-Analysis. J Pers Med. 2023; 13(9): 1283. doi: 10.3390/jpm13091283.
- Zagli G, Cianchi G, Degl’innocenti S, et al. Treatment of Fournier’s Gangrene with Combination of Vacuum-Assisted Closure Therapy, Hyperbaric Oxygen Therapy, and Protective Colostomy. Case Rep Anesthesiol. 2011; 2011: 430983. doi:10.1155/2011/430983.
- Paty R, Smith AD. Gangrene and Fournier’s Gangrene. Urol Clin North Am. 1992; 19(1): 149-162.
- Gerber GS, Guss SP, Pielet RW. Fournier’s gangrene secondary to intra-abdominal processes. Urology. 1994; 44(5): 779-82.
- Levenson RB, Singh AK, Novelline RA. Fournier gangrene: role of imaging. Radiographics. 2008; 28(2): 519-28.
- Porras L, Sáenz A, Calderon P, Gijón J. Infecciones de piel y partes blandas, en Protocolos Enfermedades Infecciosas de la Sociedad Española de Medicina Interna. 2009.
- Fajdic J, Bukovic D, Hrgovic Z, Habek M, Gugic D, et al. Manegement of Fournier´s gangrene- report of 7 cases and review of the literature. Eur J Med Res. 2007; 12: 169-172.
- Hsu H, Li CM, Sun TB, Cheng LF, Chien SH. Unilateral gracilis myofasciocutaneaous advancement flap for single stage reconstruction of scrotal and perineal defects. J Plast Reconstr Aesthet Surg. 2007; 60: 1055-1059.
- Bonkat G, Bartoletti R, Bruyeres F, Cai T, Köves B, et al. European Association of Urology. Guidelines on Urological Infections 2023.
- Kuzaka B, Wróblewska M, Borkowski T, Kawecki D, Kuzaka P, et al. Founier´s gangrene: Clinical presentation of 13 cases. Med Sci Monit. 2018; 24: 548-555.
- Misiakos E, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, et al. Current concepts in the manegement of necrotizing fasciitis. Front Surg. 2014; 29(1): 00036.
- Barquero Argüello M. Las Bases de la Gangrena de Fournier. Revista Médica de Costa Rica y Centroamérica. 2016; 73(619): 343-346.