Introduction
Total Hip Arthroplasty (THA) is the indicated treatment for
various pathologies affecting the hip joint; predominantly osteoarthritis, femoral neck fractures and osteonecrosis of the femoral
head. There are different options for fixation of the femoral implant [1]. Cemented implants, initially criticized for high loosening rates [2], have given way to non-cemented implants. Although
the recent literature does not report a better survival rate with
cemented implants compared to uncemented implants [3,4], the
latter have nevertheless become the gold standard.
Cementless implants require primary fixation to allow immediate rehabilitation without restrictions to weight-bearing. This stable primary fixation subsequently guarantees good osseointegration of the cup ensuring its long-term secondary fixation. Implants
coated with hydroxyapatite have been developed to promote
primary stability and osseointegration because of their osteoconductive properties observed in vivo [5]. While these implants have
gained popularity, the effectiveness of the hydroxyapatite coating
on long-term survival remains controversial [6,7].
There are different ways to obtain primary fixation [8]: Simple press-fit impaction and the combination of press-fit with the
placement of screws or pegs through the cup to increase its stability (increased fixation). The type of primary fixation required has
not been clearly established according to the indication. Increased
fixation of implants is sometimes used when there is insufficient
primary stability from press-fit alone, or when the bone quality
is poor. Thus, these implants appear ideal for a geriatric population, prone to osteoporosis, and in the management of proximal
femoral fractures.
Several studies comparing press-fit to augmented fixation do
not show any superiority of augmented fixation in the short- or
long-term [8-10]. Several series [11-15] report the results of acetabular implants with fixation augmented by screws and pegs
(known as tripods) with excellent results and a survival greater
than 90% at more than 15 years of follow-up [13]. The indication
for THA is primary or secondary osteoarthritis, with cases of trauma excluded. Consequently, the mean age at surgery is less than
60 years except for one study specifically investigating the use of
this type of implant in the context of acetabular revision [12].
No study, to our knowledge, presents the results of augmented
tripod fixation in a geriatric population prone to osteoporosis and
treated for proximal femoral fractures.
The primary objective of this study was to evaluate, in a geriatric population, the radiological results and the short- and medium-term survival of a Dual Mobility Cup (DMC) coated with hydroxyapatite with tripod fixation increased by 2 pegs and a screw.
The secondary objective was to evaluate the clinical results and
potential complications related to implant placement.
We formulated the hypothesis that, within a population prone
to osteoporosis, this type of implant offers satisfactory short- and
medium-term efficacy and a complication rate similar to the data
in the literature.
Material and methods
This monocentric retrospective cohort study was carried out in accordance with the Declaration of Helsinki. The Ethical Review
Board of the Ile de France IV (IRB 00003835) approved this study
on March 19, 2019 (registration number: 2019-A00229-48). The
data collection was carried out after the study was declared to the
relevant French National authorities (The Agency for the Safety of
Medicines and Health Products and The Commission on Informatics and Liberty). All patients included gave their informed consent.
The series (Figure 1).
This consecutive series of 45 patients (14 men and 31 women)
originated from a consecutive series of 59 patients operated on
between January 1, 2015 and October 31, 2018 at the Savoie metropolitan hospital center. The operators were the department’s
senior orthopedic-trauma surgeons. The inclusion criteria were
age over 70 years at the time of surgery, and placement of the
Cupule Avantage 3P plasma TIHA implant (Zimmer laboratory)
regardless of the surgical indication. The different surgical indications are detailed in Table 1.
The exclusion criteria were refusal to participate in the study,
loss of acetabular bone substance greater than or equal to stage
IIA of the Paprosky classification [16].
Table 1: Surgical indications
| Pathology |
Surgery |
n=45 |
% |
| First-line surgery |
|
30 |
66.6 |
| Femoral neck fracture |
Total hip prosthesis |
21 |
46.6 |
| Coxarthrosis |
Total hip prosthesis |
8 |
17.7 |
| Femoral head osteonecrosis |
Total hip prosthesis |
1 |
2.2 |
| Revision surgery |
|
15 |
33.3 |
| Acetabular PTH Loosening |
Acetabular unipolar revision |
5 |
11.1 |
| Gamma nail failure in apertrochanteric facture |
THA |
3 |
6.6 |
| Aseptic bipolar THA loosening |
Bipolar revision |
3 |
6.6 |
| Chronic THA Infection |
1-stage bipolar revision |
3 |
6.6 |
| Dislocation of intermediate hipprosthesis |
THA revision |
1 |
2.2 |
The characteristics of the population are summarized in Table 2.
Table 2: Preoperative characteristics of the population.
|
|
Number |
% |
Mean ± SD |
Range |
| Number |
|
45 |
|
|
|
|
Males |
14 |
31.1% |
|
|
|
Females |
31 |
68.8% |
|
|
| Age (years) |
|
|
|
79.3±5.4 |
70 - 91 |
| Height (cm) |
|
|
|
67.2±16.9 |
38 - 115 |
| Weight (kg) |
|
|
|
164.7±8.4 |
147 - 183 |
| BMI (kg/m2) |
|
|
|
24.6±5.1 |
14 - 42 |
| Pre-op Parker score |
|
|
|
7.4±2.6 |
0 - 9 |
| Comorbidities |
| Hypertension |
21 |
46% |
|
|
| Atrial Fibrillation |
12 |
26% |
|
|
| Cancer |
10 |
22% |
|
|
| Heart failure |
8 |
18% |
|
|
| Diabetes |
5 |
11% |
|
|
| Hypercholesterolemia |
5 |
11% |
|
|
| CVA |
4 |
9% |
|
|
| Renal failure |
2 |
4% |
|
|
| Respiratory failure |
1 |
2% |
|
|
| Myocardial infarction |
1 |
2% |
|
|
| Parkinson’s disease |
1 |
2% |
|
|
Surgical technique
The implant used was the TIHA Avantage 3P plasma cup, Zimmer laboratory (Figure 2).
The intervention was systematically carried out with the patient positioned in lateral decubitus, using a posterolateral
(Moore) approach. The preparation of the acetabular cavity was
done with motorized acetabular reamers of increasing size until
there was satisfactory reaming of the subchondral bone. The final
implant was chosen to have the same diameter as the last acetabular reamer used, and it was impacted in to the press-fit. The
2 pegs and the fixation screw were then added. For all patients
the Advantage E1® insert was used.
The sizes of the implants used and the characteristics of the
femoral stem are detailed in Table 3.
Table 3: Acetabular implant size and femoral stem type.
|
|
N |
% |
| Implant size |
48 |
1 |
2.2 |
| (mm) |
50 |
8 |
18 |
|
52 |
16 |
35.5 |
|
54 |
7 |
15.5 |
|
56 |
4 |
8.8 |
|
58 |
6 |
13.3 |
|
60 |
2 |
4.4 |
|
62 |
1 |
2.2 |
| Femoral stem |
AURA II® |
1 |
2.2 |
|
Standard EXCEPT |
15 |
33.3 |
|
Varied EXCEPTION |
1 |
2.2 |
|
TARGOSTM |
18 |
40 |
|
Complete UPTION® |
5 |
11.1 |
|
Unknown |
5 |
11.1 |
Evaluation method
Patient data was collected from the medical file and verbally
via a telephone call. This included all the pre- and intra-operative data, radiographs post-operatively and at the last follow-up,
the functional scores (Oxford hip score, EQ-5D-5L, Parker score),
possible complications and any revision of the implant at the last
follow-up.
The interpretation of the radiographs was carried out by 2
evaluators (CH and RP). The interpretation of the radiograph at
the last follow-up was done independently and then in comparison with the immediate postoperative radiograph. The areas of
periprosthetic osteolysis were classified according to their location (DeLee and Charnley [17]).
In the event of the patient’s death, the next of kin was contacted and asked about the cause of death and whether further
surgery on the affected hip had taken place before the death.
The primary endpoint was the clinical and radiological survival
of the implant. The secondary endpoints comprised functional
scores and reported complications.
Statistics
A sample size calculation was performed using SAS® 9.4 Proc
Power software. The study was designed for an alpha error risk
of less than 0.05. Based on the assumption of 98% survival at 2 years, a sample size of 40 had at least an 80% chance of obtaining a lower limit of the 95% Confidence Interval (CI) for implant
survival, with a CI of 9% for the margin of error.
The description of the series and the results were carried out
through descriptive statistics. Survival was calculated using the
Kaplan-Meyer technique.
Results
The mean age was 79.3±5.4 years (range: 70-90). Clinical and
radiological data were complete for 30 patients with a mean follow-up of 39.9±14 months (range: 16-79 months). Among them,
only 3 patients had a follow-up of less than 2 years.
Four patients were lost to follow-up and 11 died before the last
follow-up. For these 15 patients, radiological data were available
with a mean follow-up of 12.1±9.2 months (range: 2-39 months).
For the 11 deceased patients, none had necessary iterative surgery or implant revision before death and no death was related to
a direct complication of the surgical intervention.
Implant survival
Short-term survival was 100%, no revisions were observed.
Radiological results
For the whole series, the last radiological evaluation was made
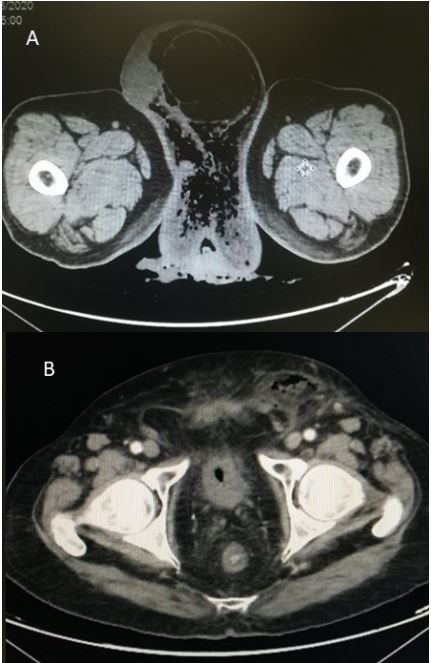
with a mean follow-up of 25.4±16 months (range: 2-79). For 3 patients, peri-prosthetic osteolysis was observed (Figure 3) in zones
I and II, as per DeLee and Charnley. For the 42 other patients, no
radiological complication (implant mobilization, screw breakage,
periprosthetic lucencies, osteolysis) was identified. No radiological changes between the immediate postoperative image and the
image at the last follow-up was visible.
Functional scores
Concerning the clinical data available for the 30 patients,
the Oxford Hip Score was 41.1±8.8 (range: 16-48). The mean
VAS was 0.9±1.6 (range: 0-7) and the mean EQ-5D-5L score was
0.6±0.3 (range: -0.1-1). The mean preoperative Parker score was
7.4±2.6 (range: 0-9) and the mean score at the last follow-up was
7.47±2.07 (range: 3-9).
Complications
One patient presented with an intraoperative Vancouver B
fracture requiring the addition of cerclage wiring. Four patients
presented with postoperative anemia requiring blood transfusions. One patient presented with moderate postoperative pain
consistent with psoas impingement but did not wish to prolong
the assessment, nor consider surgical management. Finally, 2 patients presented with peri-prosthetic femoral fractures following
falls after surgery (Vancouver A G and B1) requiring functional
treatment and plate osteosynthesis respectively. No prosthetic
dislocation was observed in the series and there were no complications related to the placement of the acetabular implant.
Discussion
This study supports our hypothesis as to the short-term efficacy of the use of a DMC with increased fixation by pegs and screws
for total hip arthroplasty in older adults for various indications.
No serious radiological complications or implant revisions were
observed. This is the first series studying this type of implant in
this population.
Our results corroborate those of the literature with a very
low rate of radiological complications and a survival rate close to
100% in the short and medium term. Philippot et al. [14] reported
96% survival at a mean follow-up of 17 years in the largest series
in the literature, including 438 patients with a tripod acetabular
implant, not coated with hydroxyapatite or macrostructure. The
causes of revisions were aseptic loosening, polyethylene wear,
intra-prosthetic dislocations and sepsis. Boyer et al. describe the
radiological results of 62 patients at 20 years of follow-up reporting 13% peri-prosthetic osteolysis, corresponding to our mediumterm observations.
The risk of periprosthetic osteolysis associated with this type
of implant remains a controversial subject. Certainly, surface irregularities between the liner and the cup related to the locations
of the pegs and screws are considered to be a cause of wear and
polyethylene debris ultimately responsible for osteolysis [18]. Various authors [19-21] corroborate this hypothesis, while Taniguchi
et al. [22] did not report a higher rate of osteolysis for this type
of implant after CT evaluation at more than 7 years of follow-up.
The interpretation of the results should be made with consideration to the limitations of the study. This study used a small cohort, with a high rate of deceased patients. The follow-up was also
limited and did not make it possible to make conclusive results
beyond the medium term. However, this limitation is specific to
the population studied given the low life expectancy of this population of geriatric patients (with a mean age of nearly 80 years
old), presenting with numerous comorbidities who underwent
treatment for proximal femoral fractures. About 30% of geriatric
patients die within a year of a femoral neck fracture [23], which corresponds to our results. The evaluation of very long-term results for this type of population is therefore not feasible and ultimately not very useful since the majority of patients die in the
short- or medium-term after surgery.
Assessment of the degree of osteoporosis by bone densitometry was not available, making it impossible to make a precise
decision on the level of bone quality of the patients in the study.
Nevertheless, 89% of patients were initially treated for a proximal femoral fracture (71%), and/or were older postmenopausal
women (68%), making the probability of an advanced osteoporotic state very high in the majority of patients in this series.
The stability of the Parker score between the pre- and post-operative data is explained by cases of revision and of initial failure
of proximal femoral osteosynthesis, in which surgery tends to improve autonomy, unlike cases of femoral neck fracture treatment
which generally leads to a loss of autonomy in the postoperative
months.
The effectiveness of a cup with augmented tripod fixation is
therefore well established. Both in subjects under the age of 60
undergoing arthroplasty for osteoarthritis [14], and in patients
over the age of 80 treated in the context of proximal femoral fractures, as exemplified by the results of this study. Nevertheless,
the usefulness of this type of implant compared to cemented or
simple press-fit implants remains debatable. Indeed, for several
authors [8,9], the increased fixation does not improve the stability of the implant over the long term compared to press-fit alone.
Brulc et al. [24] even argue that the primary stability of a pressfit cup depends almost exclusively on the surgical implantation
technique, with no significant influence on the type of implant or
patient characteristics. They conclude that failures of intraoperative primary fixation do not exceed 5% of cases when performed
by surgeons who are experienced in the simple press-fit implantation technique.
Tripod cups do not exclude the need for press-fit implantation.
Improved implant stability, in a setting where sufficient press-fit
has not been obtained, does not appear to adequately address
the technical challenge posed. In fact, the addition of a screw and
2 pegs does not offer sufficient biomechanical support to completely compensate for inadequate primary fixation, as suggested
by Goodnough et al. [25].
Conclusion
DMC with augmented fixation by screws and pegs is safe and
effective in the short- and medium-term for THA in a geriatric
population. Additional studies, allowing a comparison with pressfit fixation alone or cemented fixation, are needed to assess the
benefit of augmented fixation combining screws and pegs as an
additional option in the surgeon’s therapeutic armamentarium.
Declarations
Compliance with ethical standard: This monocentric retrospective cohort study was carried out in accordance with the
Declaration of Helsinki. The Ethical Review Board of the Ile de
France IV (IRB 00003835) approved this study on March 19, 2019
(registration number: 2019-A00229-48). The data collection was
carried out after the study was declared to the relevant French
National authorities (The Agency for the Safety of Medicines and Health Products and The Commission on Informatics and Liberty).
All patients included gave their informed consent.
This study complies with the current laws from the French legislation
Funding: No funding for this study.
Conflict of interest: CH: Clinical trial: as co-investigator of this
study for the Zimmer laboratory.
BG: No conflict of interest.
PR: Education consultant- B. Braun.
BRD: No conflict of interest.
MS: No conflict of interest.
PR: conflict of interest.
EM: Clinical trial: as principal investigator of this study for the
Zimmer laboratory.
Authors contribution
CH: Collection of clinical data, drafting of the manuscript.
BG: Writing of the manuscript.
RP: Radiological analysis, data collection.
MS: Proofreading of the manuscript, referencing.
BRD: Proofreading and editing.
PR: Proofreading and editing.
EM: Study methodology.
Ethical approval : Obtained the 19th of June (CPP ile de France)
Document in the attached file called “Ethic committee”.
Informed consent: Mentioned in the manuscript
References
- Thanner J. The acetabular component in total hip arthroplasty. Evaluation of different fixation principles. Acta Orthop Scand Suppl. 1999; 286: 1-41.
- Mulroy RD, Harris WH. The effect of improved cementing techniques on component loosening in total hip replacement. An 11-year radiographic review. J Bone Joint Surg Br. 1990; 72: 757-60.
- Jørgensen PB, Tabori-Jensen S, Mechlenburg I, Homilius M, Hansen TB, et al. Cemented and cementless dual mobility cups show similar fixation, low polyethylene wear, and low serum cobaltchromium in elderly patients: a randomized radiostereometry study with 6 years’ follow-up. Acta Orthop. 2022; 93: 906-13.
- Toossi N, Adeli B, Timperley AJ, Haddad FS, Maltenfort M, et al. Acetabular components in total hip arthroplasty: is there evidence that cementless fixation is better? J Bone Joint Surg Am. 2013; 95: 168-74.
- Overgaard S, Lind M, Rahbek O, Bünger C, Søballe K. Improved fixation of porous-coated versus grit-blasted surface texture of hydroxyapatite-coated implants in dogs. Acta Orthop Scand. 1997; 68: 337-43.
- Lazarinis S, Mäkelä KT, Eskelinen A, Havelin L, Hallan G, et al. Does hydroxyapatite coating of uncemented cups improve long-term survival? An analysis of 28,605 primary total hip arthroplasty procedures from the Nordic Arthroplasty Register Association (NARA). Osteoarthritis Cartilage. 2017; 25: 1980-7.
- Tyagi V, Harris AHS, Giori NJ. Survival of Hydroxyapatite-Coated Versus Non-hydroxyapatite-Coated Total Hip Arthroplasty Implants in a Veteran Population. J Arthroplasty. 2022; 37: 1143-5.
- Otten VTC, Crnalic S, Röhrl SM, Nivbrant B, Nilsson KG. Stability of Uncemented Cups - Long-Term Effect of Screws, Pegs and HA Coating: A 14-Year RSA Follow-Up of Total Hip Arthroplasty. J Arthroplasty. 2016; 31: 156-61.
- Ni S, Luo P, Guo L, Jiang T. Are additional screws required for pressfit fixation of cementless acetabular cups? A systematic review and meta-analysis. J Orthop Traumatol. 2022; 23: 9.
- Ni S-H, Guo L, Jiang T-L, Zhao J, Zhao Y-G. Press-fit cementless acetabular fixation with and without screws. Int Orthop. 2014; 38: 7-12.
- Boyer B, Philippot R, Geringer J, Farizon F. Primary total hip arthroplasty with dual mobility socket to prevent dislocation: A 22-year follow-up of 240 hips. Int Orthop. 2012; 36: 511-8.
- Dangin A, Boulat S, Farizon F, Philippot R. Prevention of Dislocation Risk During Hip Revision Surgery with the Dual Mobility Concept; Study of a New Generation of Dual Mobility Cups. Surg Technol Int. 2016; 29: 314-9.
- Philippot R, Camilleri JP, Boyer B, Adam P, Farizon F. The use of a dual-articulation acetabular cup system to prevent dislocation after primary total hip arthroplasty: Analysis of 384 cases at a mean follow-up of 15 years. Int Orthop. 2009; 33: 927-32.
- Philippot R, Farizon F, Camilleri J-P, Boyer B, Derhi G, et al. Survival of cementless dual mobility socket with a mean 17 years followup. Rev Chir Orthop Reparatrice Appar Mot. 2008; 94: e23-27.
- Neri T, Philippot R, Farizon F, Boyer B. Results of primary total hip replacement with first generation Bousquet dual mobility socket with more than twenty-five years follow up. About a series of two hundred and twelve hips. Int Orthop. 2017; 41: 557-61.
- Paprosky WG, Bradford MS, Younger TI. Classification of bone defects in failed prostheses. Chir Organi Mov. 1994; 79: 285-91.
- DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976: 20-32.
- Huk OL, Bansal M, Betts F, Rimnac CM, Lieberman JR, et al. Polyethylene and metal debris generated by non-articulating surfaces of modular acetabular components. J Bone Joint Surg Br. 1994; 76: 568-74.
- Pérez-Coto I, Hernández-Vaquero D, Suárez-Vázquez A, SandovalGarcía MÁ, Escandon-Rodriguez A. Influence of clinical and radiological variables on the extent and distribution of periprosthetic osteolysis in total hip arthroplasty with a hydroxyapatite-coated multiple-hole acetabular component: a magnetic resonance imaging study. J Arthroplasty. 2014; 29: 2043-8.
- Röhrl SM, Nivbrant B, Ström H, Nilsson KG. Effect of augmented cup fixation on stability, wear, and osteolysis: a 5-year follow-up of total hip arthroplasty with RSA. J Arthroplasty. 2004; 19: 962-71.
- Brodt S, Bischoff K, Schulze M, Nowack D, Roth A, et al. The use of acetabular screws in total hip arthroplasty and its influence on wear and periacetabular osteolysis in the long-term follow-up. Int Orthop. 2022; 46: 717-22.
- Taniguchi N, Jinno T, Takada R, Koga D, Ando T, et al. Do screws and screw holes affect osteolysis in cementless cups using highly crosslinked polyethylene? A 7 to 10-year follow-up case-control study. Orthop Traumatol Surg Res. 2018; 104: 307-15.
- Viberg B, Frøslev T, Overgaard S, Pedersen AB. Mortality and revision risk after femoral neck fracture: Comparison of internal fixation for undisplaced fracture with arthroplasty for displaced fracture: a population-based study from Danish National Registries. Acta Orthop. 2021; 92: 163-9.
- Brulc U, Antolič V, Mavčič B. Risk factors for unsuccessful acetabular press-fit fixation at primary total hip arthroplasty. Orthop Traumatol Surg Res. 2017; 103: 993-7.
- Goodnough LH, Bonano JC, Finlay AK, Aggarwal VK, Huddleston JI, et al. Selective screw fixation is associated with early failure of primary acetabular components for aseptic loosening. J Orthop Res. 2020; 38: 2429-33.