Introduction
Migration of a foreign body to the heart is a rare cause of chest
pain in adult patients. Various clinical manifestations have been
described in the literature, such as pericarditis and pleuritis, empyema and pneumothorax, or urgent presentation which may
require a surgical treatment like haemopericardium and cardiac
tamponade, endocarditis determining valve damage [1]. Different
types of foreign body and a variety of ways to reach the heart
have been described; the most common are direct or iatrogenic
implantation due to local trauma, intravenous migration from
another site, inhalation or may remain in the heart after medical procedure [2-5]. The diagnosis can be made with different
imaging modalities: radiography, computerized tomography and
echocardiography are main diagnostic modalities. Foreign body
can be managed conservatively, percutaneously or can be surgical removed. Treatment of this rare condition is mainly based on
clinical experience and this difficult decision should be made by
a multidisciplinary team. We present the case of an adult intravenous drug user who developed pericarditis with subsequent
cardiac tamponade, caused by embolization of a needle from the
femoral vein into his right ventricle with perforation of the free
wall (Central picture).
Case report
A 47-year-old male smoker with a history of Intravenous (IV)
drug use was admitted to the emergency department with chest
pain and dyspnea for three days. The patient had a history of Intravenous (IV) drug use that started at the age of 25 and continued over the next 12 years, after attending a rehabilitation clinic
and being managed by drug support services. Electrocardiography
(ECG) showed diffuse ST segment elevation, chest X-ray showed
mild pleural effusion and vascular congestion, transthoracic echocardiography showed mild to moderate haemopericardium, no
valvular disease, normal size and preserved systolic and diastolic
function of both ventricles, no evidence of a foreign body in the
heart or pericardium. No CT-scan was initially performed.
Initially, post-viral pleuro-pericarditis was thought to be present, so the patient was hospitalized and treated with anti-inflammatory therapy (ibuprofen 600 mg three times daily and colchicine 1 mg daily). At that time, the patient was taking Rivaroxaban
due to deep vein thrombosis diagnosed a few weeks earlier. During hospitalization, the patient remained clinically stable and the
last transthoracic echocardiography showed a regressive pericardial effusion.
For all these reasons, the patient was discharged home after
five days of medical therapy and clinical observation.
The next day he suffered a syncope and a chest pain attack
and was then readmitted to the spoke center. Blood pressure was
low, diaphoresis was evident, cardiac sounds were distant and attenuated but no murmurs were detected. The clinical signs were
suggestive of cardiac tamponade. He was admitted during the
night and there were no sonographers’ cardiologists at the spoke
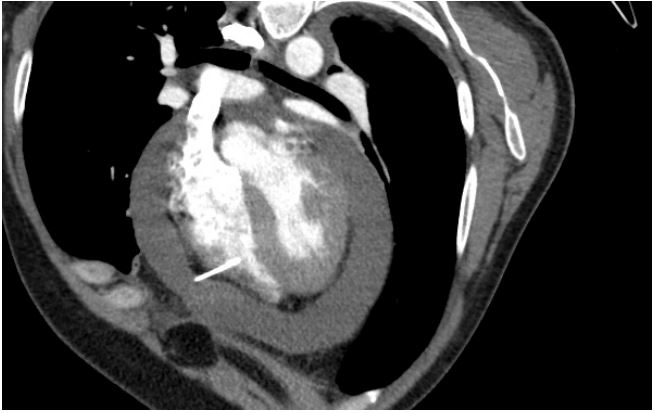
center, reason why a CT scan was performed, which confirmed
the suspicion and showed the presence of a thin metallic object
resembling a needle embedded in the right ventricular wall (Figure 1).
There was no way to drain the pericardial effusion immediately in the spoke center, either percutaneously or openly; instead,
the patient was immediately referred to our hub center and, in
consultation with our angiologist, a prothrombin complex concentrate was administered in the spoke center to prevent major
bleeding.
The patient arrived directly in the operating theatre half an
hour after the call to the cardiac surgeon. Due to the patient’s
life-threatening condition and the high risk of recurrence, it was
decided to proceed with surgical drainage and needle removal.
On arrival, the patient was obviously in a critical condition, with
oliguria and metabolic acidosis. A sternotomy was preferred over
a subxiphoid approach, due to the needle in place and recent use
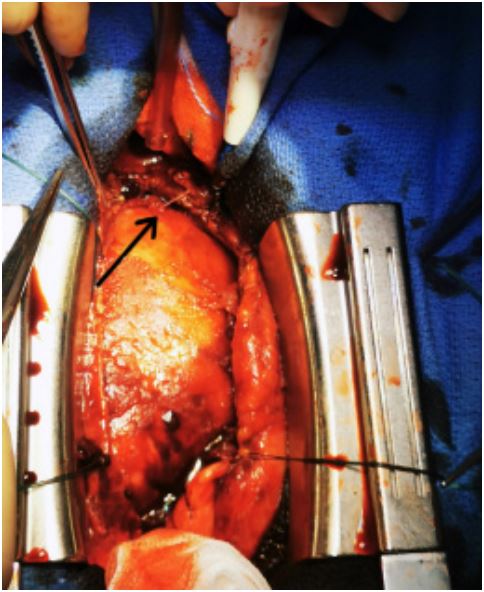
of anticoagulant. An emergency median sternotomy and pericardial opening with pressurised blood drainage was performed. The
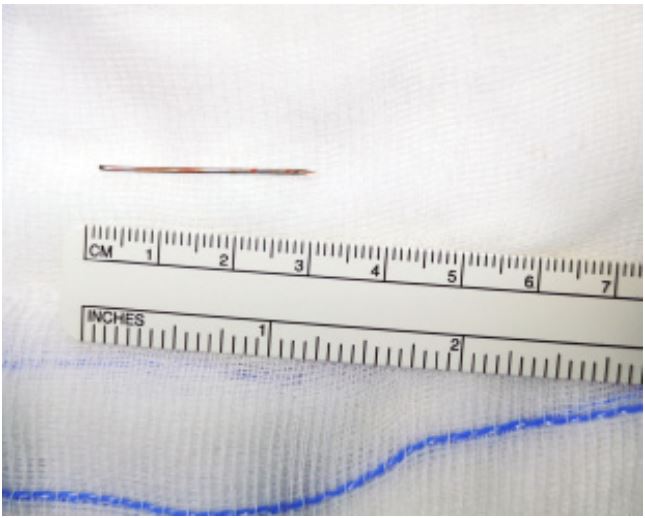
needle was found and removed immediately. No suturing was required. The tip of the perforator exited the right ventricle cavity
and perforated the free ventricle wall (Figure 2). The pericardium
was copiously irrigated; the pleural effusions were also drained
and four chest drains were placed. The chest was properly closed.
The procedure was performed with a pump on standby.
After the operation, the patient confirmed that ten years before the current event, three needles had broken off near his
femoral vessels, which he had a vascular surgeon monitor with
ultrasound at the spoke center. Immediately after surgery we performed a toxicology screening with negative result. A full body
CT had never been done before to look for more needles and it was never decided to remove them because the needles were in
difficult positions, one very deep near the great femur trochanter
and the other two near the femoral vein. After the operation, a
full body examination CT was done to confirm the position of the
needles.
The man recovered without problems and could be discharged
home.
Discussion
Needle embolism after IV drug use has already been described
[3]. In these cases, diagnosis can be difficult as the most common
symptoms are chest pain and dyspnea, but ECG and echocardiographic changes are not always present. It is very important to
take a detailed history of the patient, always considering the possibility of needle embolism in patients with a history of IV drug
use and chest pain [3,4]. In our experience, we were unaware of
the time of drug abuse, the direction of the needle, and the presence of two other needles near the patient’s femoral vein at the
time of surgery. In fact, during the operation we noted the direction of the needle from the inside of the ventricle to the outside,
so we suspect that the needle may have migrated from another
location.
There are no guidelines to support the removal of foreign bodies from the heart, either in symptomatic or asymptomatic patients, and the best strategy (removal or wait and see) is still debated. The most common approach is surgical, but the literature
also describes some cases that were treated conservatively [1]. In
this particular case, the conservative approach was not feasible
due to the rapidly deteriorating critical condition of the patient.
As we experienced in this case, the clinical picture can change
very rapidly, evolving from pericarditis to cardiac tamponade
within a few days, which is certainly favored by the use of anticoagulants. Considering this rare but life-threatening situation, it is
advisable to electively remove any known foreign body before it
can migrate, thus preventing such a serious complication, which
can even lead to the patient’s exitus.
Conclusion
The literature describes surgical removal as a difficult decision
and not always necessary, for example, when the needle is in a
stable and nonthreatening position and the patient is hemodynamically stable. The management of this rare condition and the
decision between surgical removal or conservative treatment
such as pericardiocentesis or medical therapy is a difficult decision that should be made by a multidisciplinary team.
Learning objectives
1. To identify an appropriate diagnostic and therapeutic course
in case of foreign body in the heart.
2. To recognize the importance of chest CT in cases of chest
pain in the absence of a clear diagnosis.
Disclosures: The authors have nothing to disclose.
Funding: No funding statement.
References
- Danek BA, Kuchynka P, Palecek T, Cerny V, Hlavacek K, et al. A Needle fragment embolism into the right ventricle: A rare cause of chest pain case report and literature review. Wien Klin Wochenschr. 2016; 128: 215-20.
- Arafat AA, Taha AM, Elkhouly AG, Elgalad AA. Can a foreign body migrate against natural body barriers? Ann Ped Surg. 2017; 13: 157-9.
- Hatcherson S, Venkata VS, Aedma S, Nalluri N, Sivadasan ML. Needle Embolism to the Heart: A Case Report and Review. Cureus. 2021; 13: e14469.
- Pólos M, Domokos D, Şulea CM, Benke K, Csikós G, et al. Needle in the heart: a rare case of cardiac tamponade caused by a migrated foreign body and mimicking ST segment elevation myocardial infarction. BMC Cardiovasc Disord. 2021; 21: 143.
- Ghatak A, Baik P, Cardoso R, Dobrinsky J, Kaynak H, et al. The story of the lost needle: Foreign body embolization to the heart. J Cardiol Cases. 2015; 11: 175-7.