Background
Small Cell Carcinoma (SCC) of the thymus is an exceedingly
rare diagnosis, occurring in 1 in 5.5 million patients [1]. Thymic
SCC is categorized by the World Health Organization as a poorly
differentiated, high-grade neuroendocrine carcinoma [2]. Thymic
SCC is typically aggressive and often demonstrates local tumor invasion and lymph node involvement upon diagnosis [3]. Due to
the low incidence of disease, there is limited data on thymic SCC
outcomes and no consensus exists regarding recommended treatment guidelines [4]. This case study describes the diagnosis and
management of thymic SCC incidentally found after trauma.
Clinical summary
A 69-year-old female presented to the Emergency Department
with chest pain that began after sustaining a fall. She did not have
any traumatic injuries upon workup but was incidentally found on
Computed Tomography (CT) to have a large, multilobulated cystic
mass in the anterior mediastinum. Further workup with Magnetic
Resonance Imaging (MRI) was performed, which showed a 7 cm x 8 cm x 8 cm mediastinal mass centered at the aortopulmonary
window (Figure 1). The mass was heterogenous and multiseptated, demonstrating internal necrosis and delayed enhancement.
A fine needle biopsy was non-diagnostic and an endobronchial ultrasound-guided biopsy of enlarged lymph nodes in levels
4L and 7 were negative for malignancy. Due to persistent chest
pain despite lack of traumatic injury, the patient was then taken
for surgical resection of the mediastinal mass for therapeutic and
diagnostic intent. Standard sternotomy was performed, and the
mass was noted to be contiguous with the thymus. Due to dense
adhesions, the mass was dissected along with part of the pericardium and a wedge of the left upper lung lobe. The left phrenic
nerve was involved with the tumor and sacrificed. The specimen
was removed en bloc, measuring 9.0 x 6.0 x 5.0 cm and demonstrating areas of focal hemorrhage and friable necrosis (Figure 2).
The patient had an uncomplicated post-operative course and was
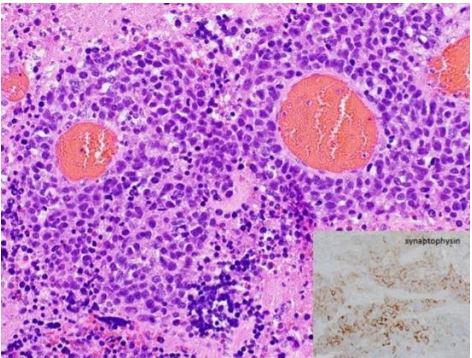
discharged home on postoperative day 4. Surgical pathology revealed high grade neuroendocrine carcinoma, measuring 9.0 cm
in greatest dimension, most consistent with thymic SCC. Focal involvement of the lung with fibrous adhesions was noted but all
margins and lymph nodes were negative for malignancy.
Upon diagnosis of thymic SCC, the patient was presented at
our multidisciplinary tumor board. A brain MRI was obtained to
complete staging, which revealed no metastatic disease. The decision was made to proceed with adjuvant chemotherapy with a
regimen including cisplatin and etoposide. Patient completed 3
out of 4 cycles but opted to discontinue further treatment due to
adverse effects. She continues to receive routine surveillance that
has been unremarkable. Patient is currently doing well without
recurrence 2 years post-operatively.
Discussion
Less than 400 cases of Neuroendocrine Tumors of The Thymus (NETTs) have been reported in the literature, of which only a
small fraction represent cases of thymic SCC [5]. NETT outcomes
vary based on histologic subtype, with thymic SCC demonstrating
a poor prognosis [6]. While the 5-year survival of other NETTs is
30-70%, that of the SCC subtype is 0% with median survival of
13.75 months [7]. When found, NETTs are relatively large tumors with a median size of 7.9 cm. Local invasion or compression lead
to symptoms like chest pain, dyspnea, or cough in nearly 40% of
patients [5,8]. However, a third of patients are asymptomatic and
diagnosed incidentally, as was the case in our report [5].
Diagnostic evaluation
Upon discovery of a mediastinal mass, diagnostic workup including imaging and tissue biopsy is recommended. The use of CT
or MR imaging techniques are typically used to assess the spread
and invasion of disease. Thymic SCC often present radiographically as a large, locally invasive mass in the anterior mediastinum
with heterogenous features and areas of necrosis, which was consistent with the characteristics found in our case study [5,9].
Tissue biopsy using core biopsy and parasternal mediastinoscopy have been recommended to obtain histologic diagnosis prior
to resection [5]. In our case, fine needle biopsy of the mass and
endoscopic ultrasound guided biopsy of suspicious lymph nodes
were initially performed. While the lymph node biopsies were
negative, the biopsy of the mass was indeterminate. Because of
this, further intervention was necessary for diagnosis. While we would have recommended further minimally invasive interventions for diagnostic purposes, our patient reported persistent
chest pain since her fall impacting her quality of life. She did not
have radiologic evidence of trauma upon imaging and the pain
was not resolving over time, so it was reasonable to believe that
the mediastinal mass could be causing this pain. Therefore, the
decision to proceed to diagnostic and therapeutic resection was
made. In our case, surgical pathology provided diagnosis of thymic SCC with R0 resection and negative lymph nodes. In addition,
complete resolution of chest pain was achieved after resection.
Disease management
Complete surgical resection has been associated with improved survival in studies involving patients with thymic SCC and
is recommended as the primary treatment for all patients with
NETT [5,6,10,11]. In cases of incomplete resection or debulking,
survival benefit is reduced or null [6,11]. The addition of lymphadenectomy to resection has been reported with mixed outcomes.
While European guidelines recommend including lymphadenectomy to the levels of N1 and N2 for NETTs and thymic carcinomas,
there is limited evidence on the survival benefits [6].
While the benefit of surgery has been demonstrated, the role
of chemotherapy and radiotherapy is largely unknown. In the neoadjuvant setting, chemotherapy and/or radiation may be helpful
in reducing tumor size and increasing rates of R0 resection in NETTs [5]. In the adjuvant setting, studies with patients who achieve
complete surgical resection have reported mixed findings. Some
studies found chemotherapy to be beneficial while others found
it to be a predictor of reduced survival [10,12]. Likewise, radiation after complete surgical resection has resulted in inconsistent
findings [11,13]. Literature describing the management of thymic
SCCs specifically is limited, as most studies include larger cohorts
that include multiple histologic categories. Terada performed a
review including 15 cases of thymic SCC. Of these, the most common chemotherapy regimen included a platin-based chemotherapy combined with etoposide [4].
Because patients with thymic malignancy can later be found
to have distant metastases, so the addition of adjuvant chemotherapy may be most appropriate in patient groups with highgrade disease, advanced staging, incomplete surgical resection,
or recurrence [14]. However, further research including prospective, randomized trials in thymic malignancies as well as studies
focused on thymic SCC is needed. As with all cases, it is important
to come to a treatment decision after a thorough discussion of
risks and benefits. In our case, the decision to pursue adjuvant
chemotherapy with carboplatin and etoposide was made.
Surveillance
Approximately 25% of NETTs are associated with MEN-1 syndrome [6]. Bohnenberger and Strobel report that the association
between MEN-1 and NETT is limited to typical and atypical carcinoid subtypes [7]. However, the studies describing this association often include a range of NETT histologic subtypes, most often
carcinoid in nature [15-17]. Literature describing thymic SCC cases
associated with endocrinopathies is limited. There are no guidelines or recommendations regarding the use of genetic testing in
thymic SCC. Thorough history and examination, as well as physician discretion, should be utilized.
Regardless of the management strategy selected for thymic
SCC, surveillance is recommended due to the high rates of recurrence and distant metastases found in NETTs [5]. Lau and colleagues recommend CT imaging of the head, neck, chest, abdomen, and pelvis at 6-12-month intervals. The addition of nuclear
medicine imaging, particularly Gallium-DOTATATE PET/CT, is helpful in cases of uncertainty or bony metastases [6].
Future studies and limitations
The literature describing thymic SCC is limited, and most studies include thymic malignancies of multiple categories within their
analyses. Further research investigating outcomes in this patient
group is needed, especially due to the poor prognosis associated
with this histologic subtype. While prospective, randomized control trials would be ideal, the rarity of this disease would likely
make this unfeasible. In the meantime, retrospective cohort studies are beneficial. This report is limited due to its nature as a case
report but contributes to the slowly growing pool of thymic SCC
patients in the literature.
Funding/Disclosures: None.
Informed consent statement: Written informed consent was
obtained from the patient for participation in this study.
References
- Gaur P, Leary C, Yao JC. Thymic neuroendocrine tumors: A SEER database analysis of 160 patients. Ann Surg. 2010; 251(6): 1117-1121. doi: 10.1097/SLA.0b013e3181dd4ec4
- Marx A, Chan JKC, Chalabreysse L, et al. The 2021 WHO Classification of Tumors of the Thymus and Mediastinum: What Is New in Thymic Epithelial, Germ Cell, and Mesenchymal Tumors? Journal of Thoracic Oncology. 2022; 17(2): 200-213. doi: 10.1016/j.jtho.2021.10.010
- Roden AC, Ahmad U, Cardillo G, et al. Thymic Carcinomas-A Concise Multidisciplinary Update on Recent Developments from the Thymic Carcinoma Working Group of the International Thymic Malignancy Interest Group. Journal of Thoracic Oncology. 2022; 17(5): 637-650. doi: 10.1016/j.jtho.2022.01.021
- Terada J, Toyoda Y, Takeuchi E, et al. Surgical resection combined with perioperative chemotherapy for a patient with locally recurrent, previously stage IV thymic small-cell carcinoma: A case report. Thorac Cancer. 2022; 13(23): 3415-3419. doi: 10.1111/1759-7714.14717
- Filosso PL, Ruffini E, Solidoro P, et al. Neuroendocrine tumors of the thymus. J Thorac Dis. 2017; 9: S1484-S1490. doi: 10.21037/jtd.2017.10.83
- Lau J, Ioan Cvasciuc T, Simpson D, C de Jong M, Parameswaran R. Continuing challenges of primary neuroendocrine tumours of the thymus: A concise review. European Journal of Surgical Oncology. 2022; 48(12): 2360-2368. doi: 10.1016/j.ejso.2022.07.017
- Bohnenberger H, Ströbel P. Recent advances and conceptual changes in the classification of neuroendocrine tumors of the thymus. Virchows Archiv. 2021; 478: 129-135. doi: 10.1007/s00428-021-03037-1/Published
- Scorsetti M, Leo F, Trama A, et al. Thymoma and thymic carcinomas. Crit Rev Oncol Hematol. 2016; 99: 332-350. doi: 10.1016/j.critrevonc.2016.01.012.
- Li J, Xia T, Zhang W, He P, Guan Y. Primary Small Cell Neuroendocrine Carcinoma of the Mediastinum: Computed Tomography and Histopathological Correlation. 2014. www.jcat.org.
- Kondo K, Monden Y. Therapy for Thymic Epithelial Tumors: A Clinical Study of 1,320 Patients from Japan. 2003.
- Wen J, Chen J, Chen D, et al. Evaluation of the prognostic value of surgery and postoperative radiotherapy for patients with thymic neuroendocrine tumors: A propensity-matched study based on the SEER database. Thorac Cancer. 2018; 9(12): 1603-1613. doi: 10.1111/1759-7714.12868
- Tang JY, Gao HJ, Shi GD, et al. Development and validation of a nomogram prognostic model for patients with neuroendocrine tumors of the thymus. Thorac Cancer. 2020; 11(9): 2457-2464. doi: 10.1111/1759-7714.13556
- Sullivan JL, Weksler B. Neuroendocrine Tumors of the Thymus: Analysis of Factors Affecting Survival in 254 Patients. Annals of Thoracic Surgery. 2017; 103(3): 935-939. doi: 10.1016/j.athoracsur.2016.07.050
- Midorikawa K, Miyahara S, Nishino N, et al. Analysis of 25 surgical cases of thymic neuroendocrine tumors and thymic carcinoma. J Cardiothorac Surg. 2024; 19(1): 225. doi: 10.1186/s13019-024-02723-w
- Singh Ospina N, Thompson GB, C Nichols F, D Cassivi S, Young WF. Thymic and Bronchial Carcinoid Tumors in Multiple Endocrine Neoplasia Type 1: The Mayo Clinic Experience from 1977 to 2013. Horm Cancer. 2015; 6(5-6): 247-253. doi: 10.1007/s12672-015-0228-z
- Jia R, Sulentic P, Xu JM, Grossman AB. Thymic Neuroendocrine Neoplasms: Biological Behaviour and Therapy. Neuroendocrinology. 2017; 105(2): 105-114. doi: 10.1159/000472255
- Ito T, Igarashi H, Uehara H, Berna MJ, Jensen RT. Causes of death and prognostic factors in multiple endocrine neoplasia type 1: A prospective study: Comparison of 106 men1/zollinger-ellison syndrome patients with 1613 literature men1 patients with or without pancreatic endocrine tumors. Medicine (United States). 2013; 92(3): 135-181. doi: 10.1097/MD.0b013e3182954af1.