Introduction
With the early detection of pulmonary malignant tumors in thoracic surgery, pulmonary segmentectomy has become a new surgical method in thoracic surgery [1]. However, segmentectomy requires thoracic surgeons to clearly understand the structure of pulmonary segments and the blood supply of blood vessels to ensure the smooth operation. Therefore, the study of the distribution of pulmonary arteries between segments has become an essential part. Ever want to get lung bronchus and vascular anatomy data was limited to a few bodies [2-5]. With the advent of three-dimensional Computed Tomography Bronchography and Angiography (3D-CTBA), we can more easily obtain lung anatomical data. With the continuous exploration of many researchers, lung anatomy has gradually become clearer. These studies have shown that the lung structure and blood vessels are extremely complex, and there are many variations, but the data of these studies are insufficient and no detailed arteriole classification is used [6,7]. Due to the existence of these positional variations, it will be difficult for the surgeon to identify the segmental bronchi and vessels during the operation. Moreover, due to the small volume of the middle lobe of the right lung, the residual lung tissue after the segmental surgery is smaller, and complications such as torsion and atelectasis are prone to occur after the operation. In this paper, we analyzed the changes of the vascular pattern of the right middle lobe artery in detail, and classified the vascular pattern of the right middle lobe artery with detailed arteriole for the first time. Preoperative chest thin layer CT and three-dimensional CT angiography, in the correct evaluation of right lung middle bronchial vascular anatomical types and clear the spatial location relationship of lung segment bronchial vessels, accurate implementation play an important role to guide the surgery.
Patients and methods
Patient preparation and examination
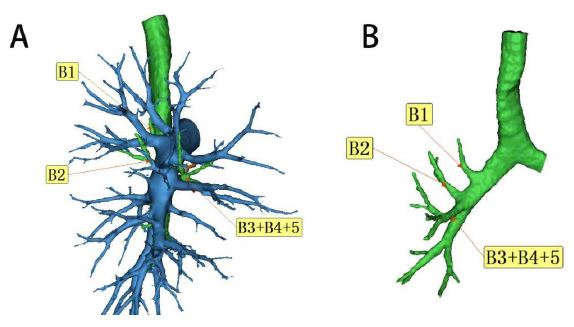
From October 2020 to October 2022, 540 patients (248 males and 292 females, with an average age of 56 years) were admitted to the Department of Thoracic Surgery of Hebei General Hospital. In one patient, there was a huge variation in the right middle pulmonary artery. There was no horizontal column in the right lung of the patient, and B3 and B4+B5 co-trunked, thus affecting the right middle pulmonary artery. It could not be typed to either type, so it was not included in the typing (Figure 1). All patients underwent sublobectomy (segmentectomy or cuneiform resection) and routine chest enhanced CT before surgery. All procedures involving human participants in this study accords with the declaration of Helsinki (revised in 2013). The Research Ethics Committee approved this retrospective study from Hebei General Hospital (No. 2023190). Because the study’s retrospective, agreed without the consent of the patients. The arterial changes in the Right Middle Lobe (RML) were classified and summarized.
Reconstruction of 3D-CTAB imaging
In the method of 3D reconstruction of the blood vessels in the middle lobe of human lung, X-ray computerized tomography equipment (SOMATOM Definition Flash, Siemens AG, Germany) was used to obtain the images of the patient’s chest enhanced CT during the arterial phase. The obtained data were transferred to a three-dimensional reconstruction software (Infer Operate Thorax Planning), which was used to convert the data into a three-dimensional structure vascular model. The three-dimensional reconstruction was completed by the thoracic surgeon, and the accuracy of the reconstruction was confirmed by mutual verification with the two-dimensional CT images.
Definition of arterial vessels in the middle lobe of the right lung (RML)
We used the same nomenclature to describe segmental structures used by Boyden et al. [2,3] and Yamashita [4]. In the classification, we found that A4 had more vascular branches, and we analyzed the blood vessels of A4 with various tiny arterioles. However, vascular branches of A5 are rare, and subsegments are distinguished only in isolated cases.
Statistics
All statistical analyses were performed using SPSS 26.0 (SPSS, Chicago, IL, USA).
Qualitative data is expressed in terms of the number of cases (percentage). The Pearson chi-square test was used to evaluate the significance of the dependence between groups. The P-value of less than 0.05 is considered statistically significant.
Results
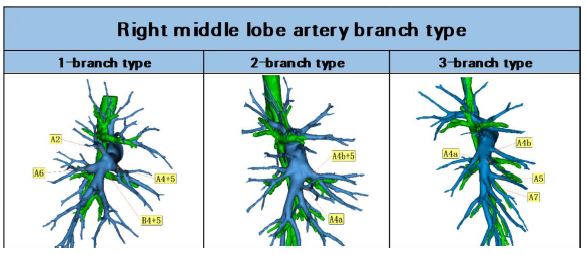
The results showed (Table 1) that the vascular classification of the middle lobe artery could be divided into 1-3 branch types (Figure 2): ① 1-branch type, that is, a large middle lobe artery trunk separated from the medial and lateral arteries, accounting for 32.6% of the total number of participants (n=176). ② 2-branch type, emanating from the right pulmonary artery respectively, the upper branch supplying the medial segment of the middle lobe and the inferior branch supplying the lateral segment, accounting for 61.1% (n=330); ③ 3-branch type accounted for 6.1% (n=33); These results are similar to those of previous studies. Thus, the 2-branch type is the most common type of the middle lobe artery, followed by the 1-branch type, and the 3-branch type is the least common. Ma’s study reported 4 branching of the artery in the right middle lobe (n=2, 0.5%) [7], but no such classification was found in this study. Among them, 12 cases had vascular walking similar to that of the left lung lingual segment.
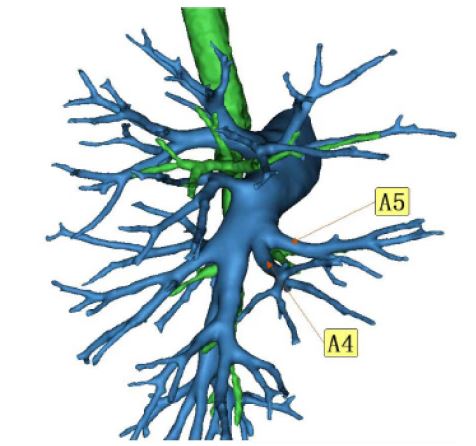
However, we found that a simple 1-3 branch types classification does not classify the complex right middle lobe vascular classification well. So we typed the right middle lobe vessels by finer arterioles. This is of great significance for understanding the vascular classification of the right middle lobe artery and guiding the delicate search and ligation of blood vessels in right middle lobe surgery. The results are shown in the table (Table 2). In the 1-branch type, this type of vascular walking was relatively simple, but in 5 patients, the blood vessels were V-shaped, emanating from a common root and immediately bifurcating into two blood vessels (Figure 3). Although these blood vessels have the same root, we need to treat them as two types of blood vessels during surgery.
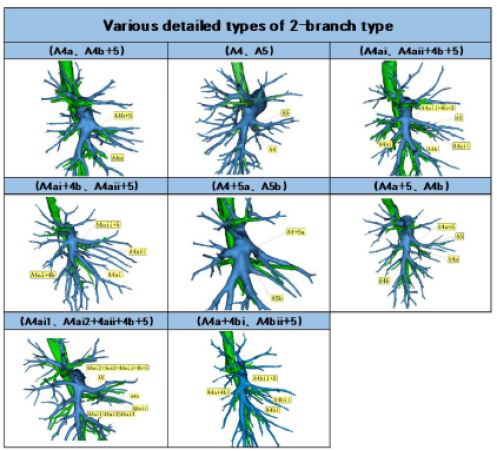
Among the 2-branch type (Figure 4), the most common type was (A4a, A4b+5), accounting for 46.1% (n=152) of the 2-branch type. followed by (A4, A5) classification, accounting for 37.6% (n=124); (A4ai, A4aii+4b+5) accounted for 11.2% (n=37); (A4ai+4b, A4aii+5) accounted for 1.8% (n=6); (A4+5a, 5b) accounted for 1.2% (n=4); (A4a+5, A4b) accounted for 0.9% (n=3); (A4ai1, A4ai2+4aii+4b+5) accounted for 0.9% (n=3); (A4a+4bi, A4bii+5) accounted for 0.3% (n=1).
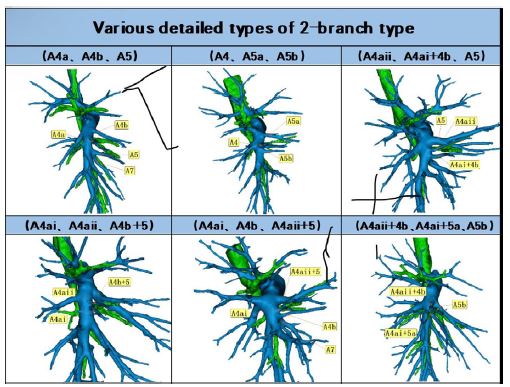
Among the 3-branch type (Figure 5), the most common type was (A4a, A4b, A5), accounting for 63.6% (n=21) of the 3-branch type. (A4, A5a, A5b) accounted for 12.1% (n=4); (A4aii, A4ai+4b, A5) accounted for 9.1% (n=3); (A4ai, A4aii, A4b+5) accounted for 6.1% (n=2); (A4ai, A4b, A4aii+5) accounted for 6.1% (n=2); (A4aii+4b, A4ai+5a, A5b) accounted for 3.0% (n=1).
Table 1: Proportion of different branch types and comparison with other studies.
|
Our study (n=540) NO. % |
Nagashima (n= 270) NO. % |
Ma (n=420) NO. % |
| 1-branch type |
176 |
32.6 |
79 |
29.3 |
128 |
30.5 |
| 2-branch type |
330 |
61.1 |
188 |
69.6 |
269 |
64 |
| 3-branch type |
33 |
6.1 |
3 |
11 |
21 |
5 |
Table 2: Detailed classification and proportion of each branch type.
|
NO. |
% |
| 1-branch type |
176 |
32.6 |
| 2-branch type |
330 |
61.1 |
| (A4a, A4b+5) |
152 |
46.1 |
| (A4, A5) |
124 |
37.6 |
| (A4ai, A4aii+4b+5) |
37 |
11.2 |
| (A4ai+4b, A4aii+5) |
6 |
1.8 |
(A4+5a, 5b)
(A4a+5, A4b)
(A4ai1, A4ai2+4aii+4b+5)
(A4a+4bi, A4bii+5)
3-branch type
(A4a, A4b, A5)
(A4, A5a, A5b)
(A4aii, A4ai+4b, A5)
(A4ai, A4aii, A4b+5)
(A4ai, A4b, A4aii+5)
(A4aii+4b, A4ai+5a, A5b) |
4
3
3
1
33
21
4
3
2
2
1 |
1.2
0.9
0.9
0.3
6.1
63.6
12.1
9.1
6.1
6.1
3.0 |
Discussion
The purpose of 3D reconstruction is to help the three-dimensional understanding of the pipeline structure, since all the reconstruction information comes from the chest CT cross-section, it is inevitable that the information will be lost during the reconstruction, so mastering the cross-section anatomy of the chest CT is the basis for constructing the three-dimensional structure of the pipeline [8]. The middle lobe artery has characteristic manifestations on chest CT, especially dynamic contrast CT, and surgeons should consciously pay attention to the variable image information before reading, deeply study its connotation, and combine three-dimensional imaging to construct the real origin, travel, and position relationship of lung duct structure, so as to effectively prevent intraoperative complications and accidents [9]. Lobectomy or segmentectomy has become a routine procedure in thoracic surgery. However, segmentectomy requires thoracic surgeons to have a clear understanding of the structure of the lung segments and blood supply to ensure the smooth operation of the operation, so the study of the distribution of pulmonary artery segments has also become an indispensable part. With the advent of 3D-CTBA, lung anatomical data can be obtained more easily, so this study used 3D-CTBA to analyze changes in the vascular pattern of the right middle lobe artery. For the first time, we have finely divided the right middle lobe artery by arterioles, and explored in detail the anatomical characteristics of the three vascular types.
The right middle lobe artery generally originates from the interlobar artery segment of the right pulmonary artery and is distributed to the medial and lateral segments of the right middle lobe. The results of this study showed that the 1branch type accounted for about 32.6% (n=176), which was the same as that of Nagashima (29.3%; P=0.336) and Ma (30.5%; P=0.484), no statistically significant difference. Among them, the lobes artery is relatively thick, all from the proximal segment of the pulmonary artery trunk, running above the middle lobe bronchus, and the posterior branch becomes the pulmonary artery, when performing lobectomy, this anatomical type is more conducive to surgical operation, and the upper approach method can be selected to give priority to the middle lobe artery, followed by the middle lobe vein and middle lobe trachea, and the lower approach method can be selected to give priority to the middle lobe vein, bronchi, and then the middle lobe artery.
We found that the proportion of 2-branch type was the highest (n=330, 61.1%), which was the same as that of Ma (64%; P=0.351), but significantly lower than Nagashima (69.6%; P=0.017). We found a total of 8 subtypes, which have not been reported in previous articles. The most common type was (A4a, A4b+5), acaccounting for 46.3% (n=152). This was followed by (A4, A5) typing, accounting for 37.2% (n=122). The anatomical characteristics of the 2-branch type blood vessels are usually above and outside the middle lobe bronchus, and their anatomical characteristics are as follows: the superior artery often originates from the proximal end of the pulmonary trunk and originates from the near horizontal fissure above the middle lobe bronchi, and the other artery, relatively thin, is located outside or below the middle lobe bronchi, and it should be noted that in the (A4, A5) classification, the two arteries are often of the same thickness. If a midlobectomy is planned, the inferior middle lobe artery can be severed preferentially, or the anterior inferior oblique fissure can be free before the artery is severed, and care should be taken to protect the artery and avoid collateral injury, especially when the lobe fissure is not well developed. At this time, it is equivalent to returning to the state of 1-branch type, because the other middle lobe artery is above the bronchi (the medial segment artery is dominant), it is very safe and reliable to dissect the middle lobe vein.
The total proportion of the 3- branch type was 6.1%, and there were 33 cases in this study, which was similar to that of Ma (5%; P=0.459), but significantly higher than Nagashima (1.1%; P=0.001). In this study, the proportion of this branch type is higher than that of other scholars, and it is also the first time that a deeper study of the 3-branch type has been carried out, and its anatomical characteristics are as follows: the first upper artery is a thicker single artery, which often originates from the proximal end of the pulmonary artery trunk, and most of them are medial arteries, which originate from the near horizontal fissure above the middle lobe bronchus, and the other two arteries are mostly lateral middle lobe arteries, usually thin, one is located on the outside of the middle lobe bronchus, and the other is located below the middle lobe bronchus. In the case of free oblique fissure, after severing one midlobe artery, it is necessary to be alert to the presence of another midlobe artery to avoid injury and bleeding. Among the 3-branche type, the most common type was (A4a, A4b, A5), accounting for 63.6% (n=21). In the 3-branche type, we find a peculiar phenomenon: A4 is co-trunked with A7. This was the case in only one case of the 2-branch type. It has also been mentioned in previous studies [6]. We further explored it and found that compared with the other three branches, the co-trunked probability of A4 and A7 was greater in the (A4a, A4b, A5) classification(p=0.047), the difference was statistically significant. In the case of free oblique fissures, it is necessary to be vigilant whether the inferior middle lobe artery is co-trunked with A7 to avoid injury and bleeding. This also means that if the 3D-CTBA is performed before surgery, the anatomical variation can be detected in advance, which can well avoid some bleeding risks.
Due to the existence of these variations, it will be difficult for the surgeon to identify the bronchial vessels of the lung segment of the right middle lobe during surgery, and because of the small size of the right middle lobe. In recent years, mid-lobe segment resection has also been frequently reported [10,11], and the residual lung tissue after lung segment surgery is smaller, and postoperative complications such as torsion and atelectasis are prone to occur. Therefore, preoperative thin-slice CT examination of the chest and 3D CT reconstruction are performed to correctly evaluate the anatomical type of bronchial vessels in the middle lobe of the right lung and clarify the spatial location relationship of the bronchial vessels in the lung segment, which plays an important role in guiding the successful implementation of the operation.
However, there are still some shortcomings in this study. First, in terms of sample size, this study only selected some cases that came to our unit for 3D reconstruction, although we have conducted a detailed study of the branches of the right middle lobe artery, but in order to fully use the 3D reconstruction to study the anatomy of the right middle lobe artery, further research with multiple centers and large samples is still needed. Second, in this study, we only performed a three-dimensional reconstruction of the artery in the middle lobe of the right lung, and the reconstruction of the bronchial in the middle lobe of the right lung is ongoing, and we should further study the relationship between vasculogenesis of the right middle lobe and bronchotyping of the middle lobe of the right lung. Thirdly, because this study is retrospective, this study was not combined with surgical data, and the effectiveness and safety of preoperative three-dimensional reconstruction in surgery could not be confirmed in actual cases.
Conclusion
We used a large number of 3D-CTBA images to explore the bronchial vascular pattern of RML and its frequency. Thoracic surgeons can use our data to guide delicate lobectomy and segmental resection.
Declarations
Conflict of interest: Author Bin Li is employed by Hebei Bio-High Technology Development CO., LTD. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding: This research was funded by Key Research and Development Program of Hebei Province (22377790D).
Data availability statement: Datasets generated and/or analyzed during the current study may be obtained from the respective authors upon reasonable request.
References
- Nakamura H, Taniguchi Y, Miwa K, et al. Comparison of the surgical outcomes of thoracoscopic lobectomy, segmentectomy, and wedge resection for clinical stage I non-small cell lung cancer. Thorac Cardiov Surg. 2011; 59. doi: 10.1055/s-0030-1250377
- Boyden EA, Hamle CJ. An analysis of variations in the bronchovascular patterns of the right middle lobe in fifty dissected and twenty injected lungs. J Thoracic Surg. 1951; 21(2): 172-188.
- Ferry RM, Boyden EA. Variations in the bronchovascular patterns of the right lower lobe of fifty lungs. J Thoracic Surg. 1951; 22(2): 188-201.
- Yamashita H. Variations in the pulmonary segments and the bronchovascular trees. Roentgenologic anatomy of the lung. Tokyo: Igaku-syoin. 1978.
- Maciejewski R, Sawa A. Relationships between divisions of the middle bronchus and vascularization patterns in the middle lung lobe. Scand J Thorac Card. 1993; 27. doi: 10.3109/14017439309099099
- Nagashima T, Shimizu K, Ohtaki Y, et al. Analysis of variation in bronchovascular pattern of the right middle and lower lobes of the lung using three-dimensional CT angiography and bronchography. Gen Thorac Cardiovas. 2017; 65. doi: 10.1007/s11748-017-0754-4
- Ma X, Lu T, Qin D, et al. Analysis of pulmonary artery variation based on 3D reconstruction of CT angiography. Front Physiol. 14 Front Physiol. 2023. doi: 10.3389/fphys.2023.1156513
- Koehler C, Wischgoll T. Knowledge-Based 3D Reconstruction and Visualization of Human Ribcage and Lungs IEEE Comput Graph. 2023. doi: 10.1109/mcg.2009.112
- Three-dimensional lung reconstructions for the localization of lung nodules to be resected during surgery.
- Zhang M, Wu Q, Ge M. Thoracoscopic right middle lobe sub segmentectomy: A single-center, retrospective review. JTCVS Tech. 13 JTCVS Tech. 2022. doi: 10.1016/j.xjtc.2022.03.004
- Yajima T, Shimizu K, Mogi A, et al. Thoracoscopic right middle lobe segmentectomy. Gen Thorac Cardiovas. 2019; 67. doi: 10.1007/s11748-018-0964-4