Introduction
The success of Arteriovenous Fistulas (AVFs) in hemodialysis patients is often dictated by inherent non-modifiable factors such as vein diameter, artery quality, diabetes status, sex, and the body’s propensity to heal [1,2]. Long-lasting functional AVFs are sometimes associated with complications such as infection, lymphedema, stenosis, aneurysm formation, ischemic neuropathy, thrombosis, congestive heart failure, and steal syndrome [1-3]. AVFs reduce digital arterial pressure, leading to ischemic hand symptoms ranging from pallor and cyanosis to ulcer and gangrene, due to the hemodynamic modifications caused by arterial shunting to the venous circulation [1,3-7]. Steal syndrome is characterized by the disappearance of pain when the venous limb is compressed or at the end of dialysis [6,7]. Proximal AVFs, old age, diabetes mellitus, cardiac dysfunction, and peripheral arterial disease are known predisposing factors [1,7,8].
Endovascular balloon dilatation of arterial stenosis or shunt ligation can be used to treat high flow steal caused by hyperfunctioning AVFs [4,5]. Venous limb ligation is the most effective treatment, which also corrects hand ischemia and vascular access loss [8,9]. Other procedures include fistula inflow redirection operations and flow restriction techniques using Distal Revascularization Interval Ligation (DRIL), Revascularization Using Distal Inflow (RUDI) for proximal fistulas, Proximalization of Arterial Inflow (PAI), and distal radial artery ligation for wrist fistulas [3,10,11]. Banding, prosthetic graft interposition, T-banding of the fistula and venous outflow, arterial stoma constriction, and fistula plication are other treatments to restrict the flow of a hyperfunctioning fistula [3,5,12-14].
This study describes a technique for partial AVF excision and re-closure to limit hyperfunction and improve upper limb distal arterial flow in hemodialysis patients. A clinical trial was conducted to assess feasibility, short-term efficacy, and complications.
Materials and methods
Patients
From January 2019 through September 2022, 1860 patients with native AVF were enrolled in the study at Alexandria University’s Vascular Surgery Unit, Department of Surgery, Faculty of Medicine, and Department of Experimental and Clinical Surgery, Medical Research Institute. After applying inclusion and exclusion criteria, only End-Stage Renal Disease (ESRD) with hyperfunctioning AVFs (n=60) that caused upper limb ischemia were enrolled as the study patients. Each participant voluntarily agreed to participate in the study after being given all relevant information about the study and given the opportunity to ask questions. The study was approved by the Alexandria University Faculty of Medicine’s Ethics Committee. Study patients were recruited and treated ethically per the World Medical Association’s Declaration of Helsinki [1].
Inclusion criteria
Patients with ESRD who met the following criteria and were receiving dialysis through a brachio-cephalic or brachio-basilic AVFs were included in the study.
1) Ischemia symptoms such as coldness, numbness, and isch ischemic pain at rest or while receiving dialysis.
2) Ischemia signs such as cold hands, cyanosis, ulceration, digital gangrene, and absent wrist pulses.
3) Clinical tests indicating a regained pulse after digital fistula compression denoting intact forearm arteries.
4) Duplex evidence of AVF hyperfunction of high flow in the fistula venous outflow and low wrist arterial flow, with or without reversal improvement with fistula compression.
Exclusion criteria
Patients who met the following criteria for distal arterial occlusive disease of the upper limb (affecting the radial or ulnar artery) were not included in the study:
1) Negative clinical test with no regained wrist pulses on fistula outflow compression.
2) Duplex evidence of radial and ulnar artery occlusive disease.
3) No improvement of wrist arterial flow on fistula compression, denoting the steal was not due to fistula hyperfunction or combined hyperfunction and distal upper limb arterial disease.
4) Having had synthetic shunt grafts.
5) Having major gangrene of the upper limb indicates amputation.
6) Having congestive heart failure.
Methods
Clinical and laboratory examinationsClinical and laboratory examinations
All study participants underwent history taking, a thorough clinical examination, and laboratory investigations. Moreover, they underwent a complaining upper limb duplex ultrasound to 1) measure flow volume (FV) (ml/min) through the fistula and venous limb outflow, 2) determine patency of distal arm vessels for exclusion of distal arterial disease, and 3) measure the distal arterial radial and ulnar artery Peak Systolic Velocity (PSV, cm/sec), recording the maximum wrist Peak Systolic Velocity (MW-PSV, cm/sec).
Steal syndrome symptoms and grading
• Study participants with steal syndrome were graded according to the severity of their symptoms as follows [1]: Grade I: Asymptomatic.
• Grade II: Mild, cold extremities; hand pulse improves after access is stopped.
• Grade III: Moderate, dialysis-related ischemic symptoms; hand-wrist pain.
• Grade IV: Severe, non-dialysis-related ischemic hand pain; finger ulcers or gangrene.
Surgical methods
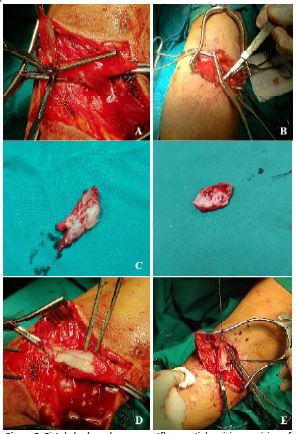
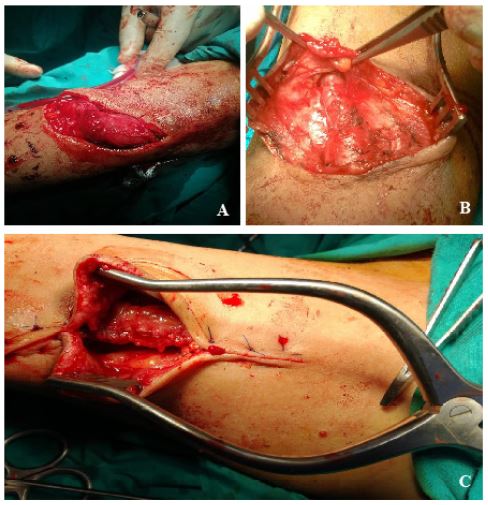
• The patient underwent pre- and intra-operative FV measurements to facilitate differentiated and effective therapy for the protection of their brachial AVF. An antecubital skin incision is used to expose the target fistula under general or local inter-scalene nerve block, with the patient lying supine. The target fistula is dissected to uncover its body and arterial and venous limbs. Figure 1A shows how the venous and arterial limbs were exposed to allow control of the proximal arterial, distal arterial, and venous limbs. Figure 1B shows how control of the venous outflow from one side and the entire fistula body from the other is possible.
• The anterior wall of a portion of the fistula body and its nearby venous limb outflow were clamped with an angled DeBakey clamp in a side-biting motion. Atraumatic vascular clamping was applied by partially occluding the fistula and attempting various levels of occlusion until achieving a level at which the wrist pulse was restored along with a working fistula (i.e., thrilling fistula with regained wrist pulse). Clinical evidence of hand reperfusion included the presence of a palpable wrist pulse and a pulse oximeter reading of 90 or higher. The ideal fistula outflow resizing that eliminated steal and maintained shunt performance would be determined by the degree of partial occlusion shown in Figure 2A and B, and the control of the fistula limbs using atraumatic vascular clamps is shown in Figure 2C.
• Removal of an ellipse of the fistula body and its venous outflow limb defined by the side-biting resizing clamp, as shown in Figure 3A-E.
• The fistula body and outflow limb are closed using continuous polypropylene sutures, as shown in Figure 4, followed by suction drainage, and wound closure.
Patients’ follow-up
Twelve months after surgery, all patients were monitored for:
• Dialysis access function and relief of ischemic manifestations of the upper limb.
• Duplex scanning immediately after stitches removal and before fistula use in dialysis to measure FO-FV and the MW-PSV to detect the changes from the preoperative values.
• Procedure complications include fistula occlusion, infection, hemorrhage, recurrent steal, and reperfusion edema.
Statistical analysis
The SPSS statistical package was used for the analysis of the data (Ver. 20.0, Armonk, NY: IBM Corp). Numbers and percentages were used to describe qualitative data. Range (minimum and maximum), mean (± standard deviation), and the Paired Students’ t-test were used to characterize the quantitative data. Statistical significance was considered at p values less than 5%.
Results
After excluding ESRD patients with heart failure, upper limb distal arterial disease, and significant gangrene, the number of hyperfunctioning fistulae that caused an upper limb ischemia was 60 (24 men and 36 women), which amounted to 3.23% from the 1860 native AVFs carried out in the two study centers at Alexandria University for four years. Twenty-seven of these 60 ESRD patients on regular hemodialysis (45%) had previously failed AVFs.
Table 1: Descriptive and clinical characteristics of End-Stage Renal Disease (ESRD) patients (n=60) with hyperfunction Arteriovenous fistulas (AVFs).
| Parameter |
Number(%) |
| Age (year)* |
49.86±10.08 |
| Sex |
| Male |
24(40%) |
| Female |
36(60%) |
| Comorbidities |
| Diabetes mellitus |
45(75%) |
| Hypertension |
48(80%) |
| Ischemic heart disease |
27(45%) |
| Chest disease |
6(10%) |
| Smoking |
18(30%) |
| History of previous access |
| Ipsilateral radiocephalic |
6(10%) |
| Ipsilateral brachiocephalic |
6(10%) |
| Contralateral fistula |
18(30%) |
| Previous ipsilateral central catheter |
30(50%) |
| Previous contralateral central catheter |
60(100%) |
| Clinical staging(Symptoms) [9] |
| Stage I: Asymptomatic |
0 |
| Stage II: Mild(pain during dialysis) |
30(50%) |
| Stage III: Moderate (hand-wrist pain) |
27(45%) |
| Stage IV: Severe(finger ulcers or gangrene) |
3(5%) |
*Age is expressed as a mean ± standard deviation (SD)
Table 2: Procedure outcomes and clinical complications after partial Arteriovenous Fistulas (AVF) excision and re-closure to limit the hyperfunction causing a steal syndrome in hemodialysis patients (n=60) over a 12-month follow-up period.
| Assessment category |
Number (%) |
| Operative |
|
| Bleeding |
0 |
| Nerve injury |
0 |
| Postoperative mortality |
0 |
| Clinical outcome |
|
| Pain disappearance |
45(75%) |
| Pain improvement |
12(20%) |
| Healing of ischemiclesions |
3(5%) |
| Patency |
60(100%) |
| Complications |
|
| Limb loss |
0 |
| Wound infection |
12(20%) |
| Swollen hand |
30(50%) |
| Recurrence of symptoms |
0 |
| Re-intervention |
0 |
Table 1 shows the descriptive and clinical characteristics of the study patients, including a wide age range (24-64) and an average (±SD) of 49.86±10.08 years. Eighteen of the patients were smokers (30%), 6 had COPD (10%), 27 had coronary artery disease (45%), and 45 had diabetes (75%). The treatment indication was hand ischemia, in all studied patients, due to hyperfunctioning native AVFs. That is, the vascular access in 36 patients (60%) was a hyperfunctioning brachio-cephalic arm fistula, while in the remaining 24 patients (40%), it was a superficialized brachio-basilic fistula. With a mean of 14.95±8.82 months, the length of their dialysis through these procedures ranged from 6 to 36 months. The most common complaint among study participants was discomfort during dialysis (Stage II in 30 patients, 50%), hand-wrist pain (Stage III in 27 patients, 45%), and a small gangrenous patch on one or two fingers (Stage IV in only three patients, 5%).
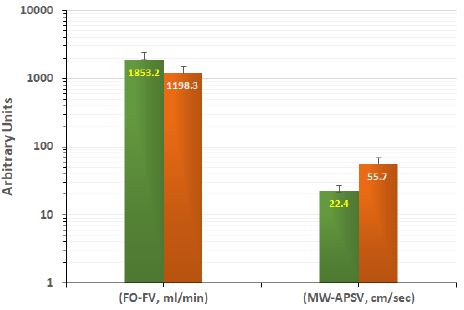
Clinical outcomes following AVF creation for dialysis are shown in Table 2, both immediately after surgery and during the 12-month clinical follow-up period. There was no obvious bleeding, nerve damage, or postoperative mortality during any of the operations. The reported assisted primary patency of the procedure was 100% within 12 months postoperatively and had zero reintervention rate. Thereby, all cases were clinically successful (100%): 45 patients had their wrist pain completely relieved; 12 patients had their wrist pain improved, and 3 patients had their fingertip ulcers completely healed. Moreover, 30 patients (50%) with swollen hands during the follow-up period may have undergone revascularization; this includes 27 patients with Stage III and 3 patients with Stage IV. Figure 5 shows that the mean postoperative FO-FV was 1198.30±311.77 ml/min, which is significantly lower (p< 0.002) than the mean preoperative FO-FV of 1853.20± 552.08 ml/min. In contrast, there was a significant postoperative increase in MW-PSV from 22.40±4.52 to 55.70±12.24 cm/sec (p< 0.002) after the partial AVF excision procedure.
Discussion
AVFs can cause reduced blood flow distal to the arteriovenous anastomosis, leading to hypoxia, ischemia and necrosis in diabetics and elderly people, known as the steal syndrome [2]. Despite evidence showing that AVFs do not usually compromise hand perfusion, between 1.6% and 8% of patients still experience unilateral hand ischemia [2,11]. The percentage of hyperfunctioning fistulae responsible for upper limb ischemia among native AVFs at two study centers was 3.23%. The low incidence of severe clinical manifestation of a high flow steal, caused by hyperfunctioning brachial AVF, and the exclusion of distal arterial disease and AV graft patients, were the reasons for the limited number of study patients. Unlike similar studies reporting low numbers [5,15], Miller et al. reported a larger number of patients (n=114), including low and high flow steal patients and patients with AV grafts [16].
The median age and male-to-female ratio of our patients are consistent with those of other studies [5,13,15], and the prevalence of diabetes and hypertension among our patients (75%) is consistent with the etiology of ESRD [17]. El-Laboudy et al. and Schneider et al. previously treated patients with hyperfunctioning native AVFs and found that cardiac overload was the main indicaindication, which they corrected by placing a synthetic T-shaped band around the fistula [5,13]. However, the current study excluded patients with congestive heart failure due to their late presentation, rendering surgery intolerable. Alexandria University’s policy is not to create fistula in patients with low cardiac reserve or heart failure.
The steal syndrome was treated with a variety of methods, but DRIL is only used to treat hand ischemia. Banding reduces the outflow of AVFs and protects the distal limb’s arterial supply by using a synthetic ring, which is prone to prestenotic dilatation, band displacement, and puncture site complications [18,19]. In addition, the arterial blood supply to the hand may be affected during the DRIL procedure due to its duration and technical difficulty. Synthetic grafts and PAI/RUDI techniques both have significant complications [20,21]. The current study found that a partial AVF excision procedure was effective for treating hand ischemia caused by hyperfunctioning native AVFs without the use of synthetic grafting or their related complications.
AVF creation for dialysis resulted in 100% assisted primary patency within 12 months, with 45 patients experiencing complete wrist pain relief, 12 patients experiencing improved wrist pain, and 3 patients having fingertip ulcers completely healed (Table 2). Similar clinical outcomes were seen using T-shaped banding, polytetrafluoroethylene circular banding, and Minimally Invasive Limited Ligation Endoluminal-Assisted Revision (MILLER)-banding. Schneider et al. reported that 33% of 22 patients with high flow steal from native AVF needed a reintervention following T-banding [5], while El-Laboudy et al. reported a 5.3% rate of re-banding following circular banding [13]. Miller et al. also reported that 3% of patients experienced operative technical failure due to bleeding, and 6% of patients required reintervention to treat an inadequate clinical response or to treat occlusion, resulting in secondary patency of 89% in 6 months in the high flow steal group [16].
Table 2 shows that 30 patients (50%) with swollen hands (27 with Stage III and three with Stage IV) may have experienced revascularization after receiving conservative treatment. Twelve patients (20%) experienced mild to moderate surgical wound inflammation, successfully managed with empirical antibiotic treatment. During the 12 months of follow-up, there were no reports of limb loss, subsequent bleeding, deep infections, recurrent ischemia symptoms, or requirements for reintervention. FO-FV after partial AVF excision agrees well with similar drops after T-banding, circular banding, and MILLER-banding [5,13,16]. Hand ischemia was significantly correlated with an MW-PSV of less than 40 cm/sec in patients with AVFs [22], and a significant difference between dialysis patients without steal and those who experienced dialysis-induced hand ischemia (55 vs. 36 cm/sec, p<0.01) was reported [23]. Thus, partial AVF excision can be used to treat fistula hyperfunctioning-induced hand ischemia and cardiac overload without the use of a synthetic band. It employs native tissues to constrict the fistula by longitudinal suture after excising a portion during a trial and create a relatively long-lasting outflow restriction. Besides, inflow or outflow arterial anastomosis was not addressed; consequently, it has no effect on the treated limb arterial anatomy.
Conclusion
Partial AVF excision is a practical technique that allows for efficient narrowing of fistula outflow and effective treatment of steal syndrome caused by hyperfunctioning fistula with minimal complications. It avoids interference with the upper limb’s natural vascular anatomy and repercussions. Unlike different banding procedures, the technique employs no synthetic material, lowering potential infection risk. After resizing, the continuous longitudinal suturing of the fistula, which tightens fibrotic circumferential narrowing of the AVF outflow, does not slip and requires no repositioning. It provides a stable flow limitation expected to be constrained by the residual flow determined during the resizing procedure. We believe future studies may include a long-term follow-up of patients also suffering cardiac overload secondary to hyperfunctioning fistulas.
Declarations
Authors’ contributions: Sameh M. Ali: Conceiving and designing the study, collecting the data, surgical procedures, analyzing and interpreting the data, and writing the original draft. Amr M. Salem: surgical procedures. Mohamed E. Salem: Providing critical revisions and approving the final manuscript. Ehab I. Mohamed: Formal statistical analysis, visualization, providing critical revisions, and writing the final manuscript. All authors have read and approved the final manuscript.
Declaration of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding sources: This research received no specific grant from public, commercial, or not-for-profit funding agencies.
References
- Masud A, Costanzo EJ, Zuckerman R, Asif A. The complications of vascular access in hemodialysis. Semin Thromb Hemost. 2018; 44(1): 57-59.
- Stolic R. Most important chronic complications of arteriovenous fistulas for hemodialysis. Med Princ Pract. 2013; 22: 220-28.
- Anaya-Ayala JE, Pettigrew CD, Ismail N, et al. Management of dialysis access-associated “steal” syndrome with DRIL procedure: challenges and clinical outcomes. J Vasc Access. 2012; 13(3): 299-304.
- Valentine RJ, Bouch CW, Scott DJ, et al. Do preoperative finger pressures predict early arterial steal in hemodialysis access patients? : A prospective analysis. J Vas Surg. 2002; 36: 351-6.
- Schneider CG, Gawad KA, Strate T, et al. T-banding: A technique for flow reduction of a hyperfunctioning arteriovenous fistula. J Vasc Surg. 2006; 43: 402-5.
- Brown PW, Mitchell DC. Central Venous and Dialysis Access. In: Loftus I, Hinchliffe R. editors. A companion to specialist surgical practice: vascular and endovascular surgery, (6th Ed.) China: Elsevier. 2019; 251-265.
- Yeager RA, Moneta GL, Edwards JM, et al. Relationship of hemodialysis access to finger gangrene in patients with end-stage renal disease. J Vasc Surg. 2002; 36: 245-9.
- Van Hoek F, Scheltinga MR, Kouwenberg I, et al. Steal in hemodialysis patients depends on type of vascular access. Eur J Vasc Endovasc Surg. 2006; 32: 710-17.
- Tordoir JH, Dammers R, van der Sande FM. Upper extremity ischemia and hemodialysis vascular access. Eur J Vasc Endovasc Surg. 2004; 27: 1-5.
- Letachowicz K, Kusztal M, Gołębiowski T, et al. External dilator-assisted banding for high-flow hemodialysis arteriovenous fistula. Renal Failure. 2016; 38: 1067-70.
- Inston N, Schanzer H, Widmer M, et al. Arteriovenous access ischemic steal (AVAIS) in haemodialysis: a consensus from the Charing Cross Vascular Access Masterclass 2016. J Vasc Access. 2017; 18: 3-12.
- Kok HK, Maingard J, Asadi H, et al. Percutaneous dialysis arteriovenous fistula banding for flow reduction - a case series. CVIR Endovascular. 2018; 1: 27.
- El-Laboudy ME, Sorour WA, Tawfik AM. Is polytetrafluoroethylene circular banding an effective technique for treatment of high-flow vascular access-induced steal syndrome? Egy J Surg. 2020; 39(2): 387-92.
- Karaca OG, Kunt A, Koc A. Treatment of steal syndrome in patients with arteriovenous fistula: Narrowing the arterial part of anastomosis. Nat Vasc Endovasc Surg Society. 2018; 27: 166-71.
- Mestres G, Fontseré N, Bofill R, et al. treatment of vascular access-related steal syndrome by means of juxta-anastomotic vein interposition of a prosthetic graft segment. Nefrologia. 2014; 34(2): 235-42.
- Miller GA, Goel N, Friedman A, et al. The MILLER banding procedure is an effective method for treating dialysis-associated steal syndrome. Kid Int. 2010; 77: 359-66.
- El Ghoul B, Daaboul Y, Korjian S, et al. Etiology of end-stage renal disease and arterial stiffness among hemodialysis patients. BioMed Res Int. 2017. https: //doi.org/10.1155/2017/2543262
- Murray BM, Rajczak S, Herman A, Leary D. Effect of surgical banding of a high-flow fistula on access flow and cardiac output: intraoperative and long-term measurements. Am J Kidney Dis. 2004; 44: 1090-6.
- Meyer F, Muller JS, Grote R, et al. Fistula banding-Success-promoting Approach in Peripheral Steal Syndrome. Zentralbl Chir. 2002; 127: 685-8.
- Callaghan CJ, Mallik M, Sivaprakasam R, et al. Treatment of dialysis access-associated steal syndrome with the “revision using distal inflow” technique. J Vasc Access. 2011; 12(1): 52-6.
- Thermann F, Wollert U, Ukkat J, Dralle H. Proximalization of the arterial inflow (PAI) in patients with dialysis access-induced ischemic syndrome: first report on long-term clinical results. J Vasc Access. 2010; 11(2): 143-9.
- Karundenga BS, Muradib A, Kekalihc A. Correlation Between Hand Ischemia Questionnaire and Peak Systolic Velocity of Radial Artery and Ulnar Artery in Hemodialysis Patients with Upper Arm Native Fistula Arteriovenosa. JINASVS. 2020; 1(1): 1-5.
- Vaes RHD, Tordoir JH, Scheltinga MR. Blood flow dynamics in patients with hemodialysis access-induced hand ischemia. J Vasc Surg. 2013; 58: 446-51.